
Abstract
Purpose:
The aim of this study is to analyze the effect of internal limiting membrane peeling in removal of idiopathic epiretinal membranes through meta-analysis.
Methods:
We searched PubMed for studies published until 30 April 2018. Inclusion criteria included cases of idiopathic epiretinal membranes, treated with vitrectomy with or without internal limiting membrane peeling. Exclusion criteria consisted of coexisting retinal pathologies and use of indocyanine green to stain the internal limiting membrane. Sixteen studies were included in our meta-analysis. We compared the results of surgical removal of epiretinal membrane, with or without internal limiting membrane peeling, in terms of best-corrected visual acuity and anatomical restoration of the macula (central foveal thickness). Studies or subgroups of patients who had indocyanine green used as an internal limiting membrane stain were excluded from the study, due to evidence of its toxicity to the retina.
Results:
Regarding best-corrected visual acuity levels, the overall mean difference was –0.29 (95% confidence interval: –0.319 to –0.261), while for patients with internal limiting membrane peeling was –0.289 (95% confidence interval: –0.334 to –0.244) and for patients without internal limiting membrane peeling was –0.282 (95% confidence interval: –0.34 to –0.225). Regarding central foveal thickness levels, the overall mean difference was –117.22 (95% confidence interval: –136.70 to –97.74), while for patients with internal limiting membrane peeling was –121.08 (95% confidence interval: –151.12 to –91.03) and for patients without internal limiting membrane peeling was –105.34 (95% confidence interval: –119.47 to –96.21).
Conclusion:
Vitrectomy for the removal of epiretinal membrane combined with internal limiting membrane peeling is an effective method for the treatment of patients with idiopathic epiretinal membrane.
Introduction
Epiretinal membrane (ERM) is a quite common disorder of the vitreomacular interface. Studies have reported the prevalence of ERM, ranging from 7.0% to 11.8% and have shown differences in prevalence across ethnicities.1,2 Systemic factors have also been found to be associated significantly with the formation of the membrane like age and hypertriglyceridemia. 3 Its presence can cause visual impairment which can be significant and affect the quality of life of patients, requiring surgical treatment for the peeling of the membrane. Current knowledge about the pathogenesis points to a pathologic proliferation of cells (glial, retinal pigment epithelium cells, and myofibroblasts) that migrate through defects in the internal limiting membrane (ILM).4,5
In cases of idiopathic ERMs, the traction exerted on the retina causes the proliferation of Müller cells through cellular protein mediators (GFAP, vimentin) in a process called gliosis. These defects may occur in the absence of any pathologic situations near retinal vessels. Larger breaks may occur due to posterior vitreous detachment (PVD) in paravascular areas.6–8
Moreover, during vitreoschisis, when it occurs anterior to the level of hylocytes, a cellular layer is left on the macula. 9 Hylocytes lying on the macular surface proliferate, recruit glial cells and induce collagen fibers contraction. 10
Advances in optical coherence tomography have revealed detailed features of macular anatomy. These features serve as prognostic factors for visual acuity (VA) recovery after surgical removal of ERMs. Best-corrected visual acuity (BCVA) and central foveal thickness (CFT) are the commonest factors examined for the assessment of patients with ERM.11–15 BCVA is measured in logarithmic scale for statistical analysis. CFT is measured using spectral domain optical coherence tomography (SD-OCT).
Indocyanine green (ICG) is a dye that has been widely used for the staining of ILM in vitreoretinal surgery. However, due to findings pointing the retinal toxicity of this dye, during the past years, it has been mainly replaced by trypan blue and brilliant blue G for ERM surgery.
The aim of this systematic review and meta-analysis was to study the effect of ILM peeling in surgical removal of ERMs.
Methods
Search strategy and selection criteria
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We considered all studies regarding surgical treatment of patients with macular pucker comparing membrane peeling with or without ILM removal but also studies of surgical removal with ILM removal standalone. We searched PubMed using the following keywords (terms): (epiretinal membrane OR macular pucker) AND (ILM) AND (peel or peeling). We searched for studies published in English language, until 30 April 2018. The first search retrieved 337 studies. Three-hundred and seven papers were excluded after title/abstract screening. Thirty articles were read in full text, 12 were excluded for ICG being used for ILM peeling and 2 during data extraction because standard deviation values, necessary for statistical analysis, were missing. Finally, 16 studies were included in meta-analysis16–31 (Figure 1).
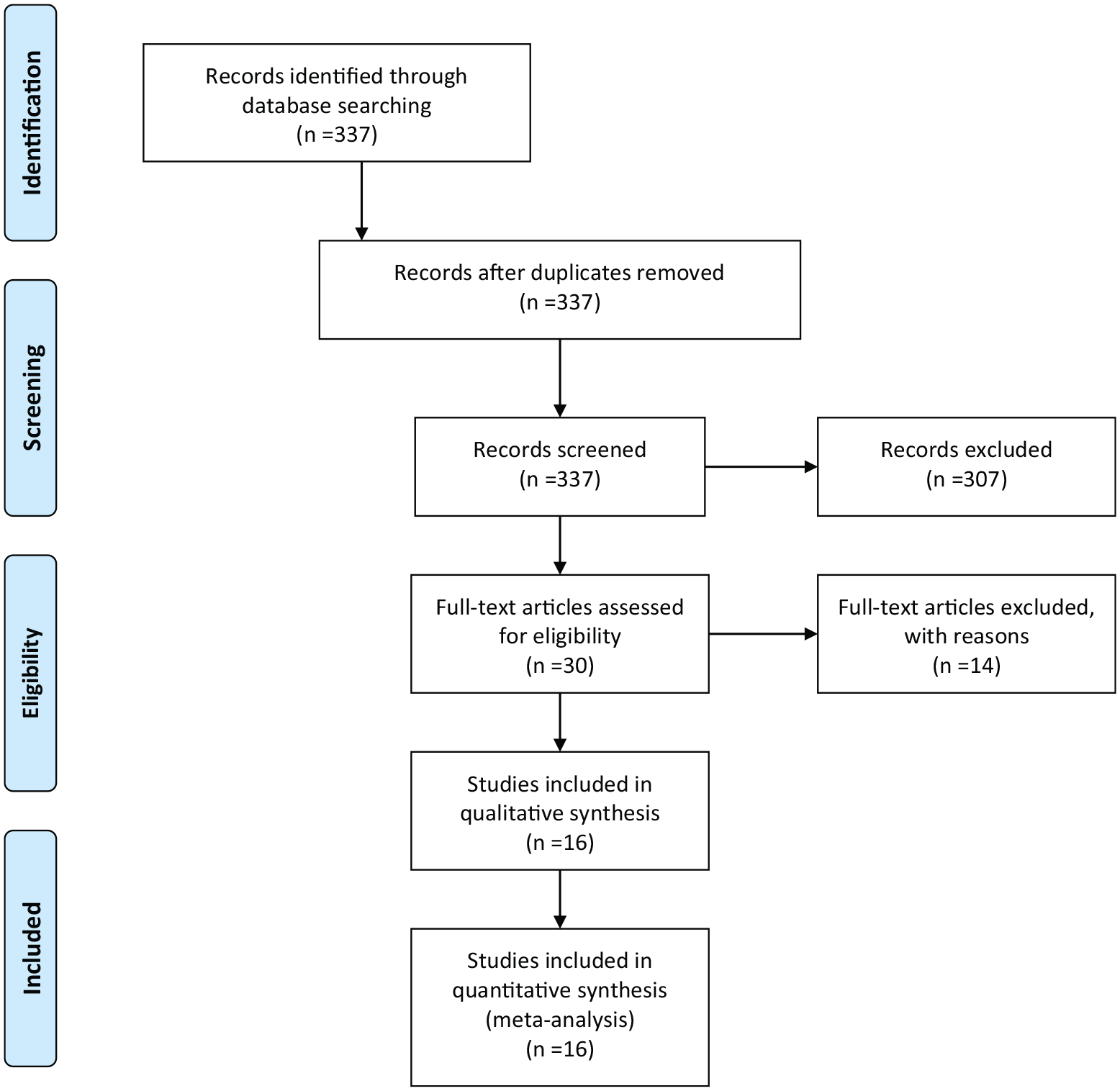
PRISMA Flow Diagram.
Inclusion criteria included cases of idiopathic ERMs, treated with vitrectomy with or without ILM peeling and assessed for logMAR BCVA and foveal thickness measurement. Exclusion criteria consisted of coexisting retinal pathologies and the use of ICG to stain the ILM. Studies (or subgroups of studies) where ICG had been used were excluded from the meta-analysis.
Data extraction
The data were independently extracted by two reviewers and rechecked after the first extraction. We recorded information on study characteristics and demographics such as authors, publication year and journal, sample size, treatment modality (with or without ILM peeling) preoperative and postoperative VA in LogMAR, preoperative and postoperative central macular thickness in μm. Totally 16 studies were included16–31 (Tables 1 and 2).
Data extracted regarding BCVA in logMAR.

BCVA, best-corrected visual acuity; ILM, internal limiting membrane; TA: triamcinolone; BBG: brilliant blue G; PMID: PubMed IDentifier.
Data extracted regarding CFT in μm.

CFT, central foveal thickness; ILM, internal limiting membrane; PMID, PubMed IDentifier; TA, triamcinolone; BBG, brilliant blue G.
Statistical analysis and meta-analysis
We used mean BCVA and CFT, standard deviations, and sample sizes reported in the individual studies to calculate effect size in means of mean difference. Mean differences and 95% confidence intervals (CIs) in after/baseline BCVA and CFT levels were calculated. A random effects model (DerSimonian Laird method) and the generic inverse variance method were used since the heterogeneity was moderate to high. Statistical level significance between after/baseline BCVA and CFT levels was set at 0.05. We checked for heterogeneity with Cochran’s Q-test, where p < 0.10 denotes statistically significant heterogeneity and quantified the degree of heterogeneity with the I 2 index. 32 Increased I 2 index corresponds to increased heterogeneity, and values of 25%, 50%, and 75% are considered as low, moderate, and high heterogeneity, respectively. 33 Egger test and Begg & Mazumdar test were used for the estimation of publication bias (p > 0.1 in both tests indicates the absence of publication bias. Statistical analysis was performed with OpenMeta(analyst) software.
Results
All studies found a statistically significant increase (p < 0.05) in postoperative BCVA and decrease in postoperative CFT levels versus preoperative levels. Regarding BCVA levels, the overall mean difference was –0.29 (95% CI: –0.319 to –0.261), while for patients with ILM peeling was –0.289 (95% CI: –0.334 to -0.244) and for patients without ILM peeling was –0.282 (95% CI: –0.34 to –0.225; Figure 2). Moderate heterogeneity between studies was found in all cases (I 2 = 66.4% for all patients, I 2 = 68.5% for patients with ILM peeling and I 2 = 67.5% for patients without ILM peeling). There was publication bias (p = 0.011 for Egger test and p = 0.002 for Begg & Mazumdar test). In addition, regarding CFT levels, the overall mean difference was –117.22 (95% CI: –136.70 to –97.74), while for patients with ILM peeling was –121.08 (95% CI: –151.12 to –91.03) and for patients without ILM peeling was –105.34 (95% CI: –119.47 to –96.21; Figure 3). Low to high heterogeneity between studies was found (I 2 = 76.3% for all patients, I 2 = 82.8% for patients with ILM peeling and I 2 = 2.4% for patients without ILM peeling). There was publication bias (p = 0.001 for Egger test and p = 0.003 for Begg & Mazumdar test).
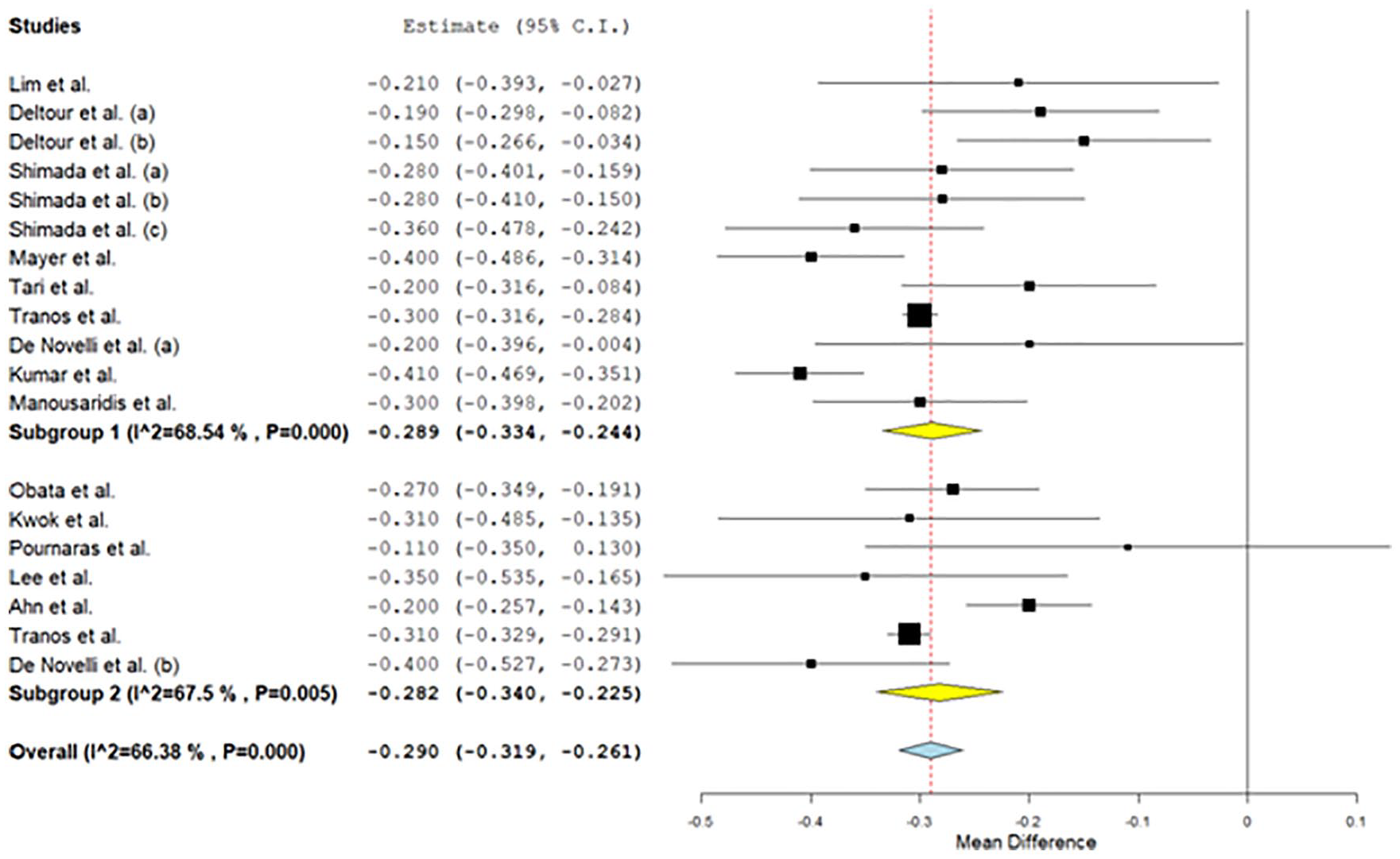
Results for preoperative–postoperative BCVA.

Results for preoperative-postoperative CFT.
The risk of bias assessment was performed according to Newcastle Ottawa scale for non-randomized controlled trials (Table 3). For randomized controlled trials, we used the Cochrane risk of bias tool (Table 4).
Risk of bias – Newcastle Ottawa Scale.

NOS: Newcastle Ottawa Scale
A study can be given a maximum of one star for each numbered item within the Selection and Outcome categories.
A maximum of two stars can be given for Comparability.
Cochrane Risk of Bias.

: low risk of bias; –: high risk of bias, ?: unclear risk of bias.
Discussion
The ILM peeling for ERM removal is still a debate among vitreoretinal surgeons. However, the fact that ILM patches are peeled along the ERM peeling is proved through histopathology. The rationale for the ILM peeling is that it serves as a scaffold for cell proliferation and that it may bring remains of the ERM. Many studies have shown the superiority of ILM peeling in terms of recurrence rates.26,34–36 On the contrary, the removal of ILM affects the retinal cells, as it consists of Müller cell footplates. Studies have shown anatomical and functional alterations because of that however without affecting the final visual outcome of the intervention.24,37
So far, the meta-analyses published38–41 include studies that were carried out using ICG. Taking into account the proven toxicity of this dye, we considered conducting a meta-analysis including only either studies that did not use ICG at all, or parts of studies in case the authors discriminated groups using this dye or not.
The purpose of this article was to investigate the effect of the removal of ILM in the surgical treatment of ERMs regarding the anatomical and functional results. The technique of ILM removal is not new; however, through the years, there have been several dyes used to assist the peeling. ICG dye has been used widely in the past in order to stain ILM. However, its use has been dropped due to its toxic effects for the retina.42,43 Toxicity is attributed to ICG’s direct biochemical effects causing inner retinal cell defects and apoptosis of retinal pigment epithelium (RPE) cells, through alterations in protein expression. 44 It is concentration and exposure time dependent.45,46 ICG can also enhance light toxicity. 47
Brilliant blue is found to have great affinity with ILM 48 and is safer to use in comparison with ICG.49,50 When compared to triamcinolone for ILM peeling in cases of idiopathic macular holes, brilliant blue was found to be an effective alternative with good or even better anatomical and functional results.51,52 It is also superior for the visualization of the vitreomacular interface. 52
Pars plana vitrectomy with ILM peeling is a broadly performed surgical intervention for posterior pole pathologies. 53 Nevertheless, the peeling of the ILM results in changes of the nerve fiber layer (RNFL) due to exerted mechanical forces. The early changes consist of swelling of the arcuate nerve fiber (SANFL). 54 It is described as hypofluorescent arcuate striae in infrared and autofluorescence imaging that corresponds to hyper-reflection on spectral domain OCT. 55 SANFL is suspected to be initiated at the point of forceps grasping rather than the ILM peeling traumatizing Müller cells’ footplates. Moreover, it resolves after a period of 2–3 months without affecting VA. 53 After that period, dimples within the inner retina might appear, forming dark arcuate striae. This phenomenon is called dissociated optic nerve fiber layer (DONFL). It has been suggested that the pattern of DONFL is not actually damage, but it occurs from the irregular distribution of Muller cells which is denser among nerve fiber buntles. 56 Despite these changes, DONFL is found not to affect VA.57,58 On the other hand, ERM removal with ILM peel, inspite of the visual gain may result in subtle multifocal ERG abnormalities detectable in 12 months after surgery. 16 Regarding glaucoma patients, vitrectomy for ERM removal with ILM peeling is in general a safe procedure. Transient changes in temporal nerve fiber layer thickness do not affect VA, 59 and visual fields do not deteriorate after vitrectomy for ERM with ILM peeling. 60
An important limitation, concerns the fact that there are only few studies with histopathologic analysis for determining the extent of simultaneous ILM peel during ERM peeling. Also, it is unclear whether surgeons checked for positive ILM staining after the ERM removal. Brilliant blue facilitates the identification of residual ILM with double staining. 19 It has been shown that in the majority of cases, ILM parts are removed along with the ERM. 61 Histopathologic analysis confirms the use of dyes for the identification of ILM as a reliable method. 62
Regarding risk of bias non-randomized controlled trials were assessed for selection, comparability, and exposure, whereas randomized controlled trials were assessed for random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. The main weakness of our study is that only three of the studies included were randomized control trials. Investigators either applied one of the mentioned techniques or due to the use of ICG-assisted ILM peeling, one of the groups of patients was excluded. More randomized controlled studies are needed in order to get more safe results after comparing the two methods.
Conclusion
Both methods are effective in terms of improvement in VA and reduction of macular thickness. More randomized controlled studies are needed in order to compare the two techniques.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.