
Abstract
Purpose:
This study aims to estimate the crude and standardized prevalences of cataract and its related factors among old people in northern parts of Iran.
Methods:
This cross-sectional study was carried out among 397 people aged 60 and older in northern Iran. Required information about treated and nontreated cataract was collected using a standard checklist. The World Standard Population was applied for direct standardization.
Results:
The standardized prevalence (95% confidence interval) of cataract among men, women, and all people were 27.5% (21.2–33.8), 30.9% (24.5–37.4), and 29.1% (24.6–33.6), respectively. Based on multivariate logistic regression models, age over 75 years (OR = 3.03, 95% CI: 1.21–7.59), living alone (OR = 4.89, 95% CI: 1.86‒12.86), diabetes mellitus (odds ratio = 19.10, 95% confidence interval: 8.13–44.89), rheumatoid arthritis (OR = 7.76, 95% CI: 2.32–25.99), history of infectious diseases (OR = 4.02, 95% CI: 1.35‒11.98), hypertension (OR = 3.19, 95% CI: 1.59–6.42), history of ophthalmic surgery (OR = 2.83, 95% CI: 1.29–6.16), history of sedative drug use (OR = 2.71, 95% CI: 1.35–5.47), history of vitamin supplementation use (OR = 0.21, 95% CI: 0.08–0.55), and familial history of cataract (OR = 2.81, 95% confidence interval: 1.38–5.72) increased the odds of cataract. Our multiple logistic regression model explained 53% of the variation in developing cataract.
Conclusion:
Our study showed that the prevalence of cataract in the study population was relatively high. We also found that aging, living alone, diabetes mellitus, rheumatoid arthritis, hypertension, infectious diseases, ophthalmic surgery, sedative drugs and familial history of cataract were the risk factors of cataract and vitamin supplementations were its protective factors.
Introduction
Blindness is an important source of fear in the elderly second only to death. Cataract is one of the main causes of vision loss. 1 It is defined as clouding of the lens and is one of the most common preventable causes of disability in the elderly in developing and developed countries.2–4
Approximately 285 million people are suffering from visual impairment, more than 39 million of whom are blind. Despite the implementation of the ‘Vision 2020’ program for reduction of preventable visual disorders, refractive disorders and cataract are still responsible for 80% of the causes of visual impairment in the world. Half of them are due to cataract.5–7
In a study carried out in the rural areas in north-east of Iran, 17.6% of cases with visual impairment were due to cataract. 7 Also, cataract with 30.7% was the leading cause of visual impairment in Saudi adults. 8 In a study in Nepal, frequency of cataract in subjects over 60 years with bilateral low vision was 68.07%. 9
In Peru, the age–sex standardized prevalence of bilateral blindness was estimated at 2.1%. 10 Results of a study conducted in Iran showed different prevalences of cataract regarding sex. It also revealed a higher chance of developing nuclear, cortical, and posterior subcapsular cataract (PSC) among smokers compared with nonsmokers. 11
There are no sufficient evidences in case of prevalence and related factors of cataract among Iranian elderly. Considering the extent of geographical, climatic, cultural, and ethnical situation of Iran, estimating the sex–age standardized prevalence of cataract as well as relevant risk factors is necessary. Such information provides reliable evidences which are suitable for planning preventive programs as well as designing appropriate analytic researches. This study aimed to estimate crude and standardized prevalence of cataract and its associated factors among elderly population in northern Iran.
Methods
This cross-sectional study was carried out in a ‘day clinic’ (a clinic with limited services and facilities) in northern Iran (Mazandaran-Chaloos). The most patients referred to this clinic were patients from Chaloos and Noshahr in Western Mazandaran province including 111,542 and 138,913 population, respectively.
This study was conducted based on the Declaration of Helsinki. The study was approved by Mazandaran University of Medical Science Ethics Committee (Ethical Code: 546). Informed consents were obtained from all participants. A grant for this study was provided by Student Research Committee of this institute.
The study population was aged 60 and older. The required sample size for the detection of 50% (maximum prevalence), 95% confidence level, and accuracy of 0.05 based on the one-sample proportion formula was estimated at 397. Using the consensus method, from January 2016, the target population was entered into the study until providing the required sample size which was ended in May 2016. The information was collected using a checklist designed based on the available literature. The checklist included questions regarding demographic characteristics, history of communicable and noncommunicable diseases, ophthalmic problems other than cataract, history of ophthalmic surgery, history of blunt ophthalmic trauma, history of daily consumption of corticosteroids, vitamin supplementations (B, C, E), and sedatives (at least 6 months), daily fat consumption, daily fruit/vegetable consumption, history of alcohol consumption and cigarette smoking, history of working in open places or living in tropical areas of southern Iran, daily exercise, history of frequent X-ray imaging of the head, history of contact lens use, using personal antisolar protective instruments such as hat and glasses, familial history of cataract, residence area (urban/rural), and history of having cataract (operated and non-operated).
Statistical analysis
Data analysis was performed using SPSS version 22 software (SPSS Inc., Chicago, IL, USA). Study variables were described as percent frequency, mean, standard deviation, minimum, and maximum. Mean age of the participants was compared between groups using independent t test. Frequency of categorical variables was compared between groups using chi-square test. Multiple logistic regression models were applied to estimate the effect of different variables controlling for potential confounders. All variables showing significant association with cataract in the univariate models (p < 0.1) were entered into the multivariate models. The goodness of fit for these models was assessed using Nagelkerke’s R2. To adjust the effect of age and sex on the prevalences, direct standardized prevalences were estimated based on Segi’s World Standard Population per 100,000. 12
Results
Totally, 397 patients aged over 60 referring to Imam Reza day clinic in Chaloos, Mazandaran (northern Iran) were recruited in the study. Of them, 205 (51.6%) were female. Mean, standard deviation, minimum, and maximum age for them were 69.1, 7.1, 60, and 90 years, respectively. Men were slightly older than women, but the difference was not statistically significant (69.17 ± 7.16 versus 69.04 ± 7.02, p = 852).
Crude prevalences of cataract among men, women, and all population were 28.6%, 31.2%, and 29.9%, respectively. Controlling for age and sex, the standardized prevalences [95% confidence intervals (CIs)] were 27.5% (21.2–33.8), 30.9% (24.5–37.4), and 29.1% (24.6–33.6), respectively. The observed difference regarding sex was not statistically significant (p = 0.576). The affected eye was the left eye in 23 (5.8%), right eye in 26 (6.5%), and both eyes in 70 (17.6%) patients. Mean [standard deviation (SD)] ages of those with and without cataract were 71.07 (7.72) and 68.25 (6.62) years, respectively (p = 0.001). Mean (SD) body mass indexes (BMIs) for patients with and without cataract were 26.54 (4.92) and 26.21 (3.94), respectively (p = 0.483).
Based on the results of univariate analyses, prevalence of cataract was higher among rural residents than urban residents (33.3% versus 27.8%, respectively, p = 0.240), obese patients than normal BMI patients (35.7% versus 26.8%, respectively, p = 0.374), low-income persons than high-income ones (36.7% versus 28.6%, respectively, p = 0.100), diabetic patients than nondiabetics (72.4% versus 19.9%, respectively, p < 0.001), hypertensive patients than normotensives (60.8% versus 20%, respectively, p < 0.001), and patients with rheumatoid arthritis than those without (76% versus 26.9%, respectively, p < 0.001). Details of the other investigated factors are presented in Table 1.
Characteristics of patients with and without cataract.

BMI, body mass index.
Adjusting the effect of potential confounders using multiple logistic regression models, the odds of developing cataract was higher in patients aged over 75 years [odds ratio (OR) = 3.03, 95% CI: 1.21–7.59], patients living alone (OR = 4.89, 95% CI: 1.86‒12.86), diabetic patients (OR = 19.10, 95% CI: 8.13–44.89), patients with rheumatoid arthritis (OR = 7.76, 95% CI: 2.32–25.99), patients having history of infectious diseases (OR = 4.02, 95% CI: 1.35‒11.98), hypertensive patients (OR = 3.19, 95% CI: 1.59–6.42), patients with history of ophthalmic surgery (OR = 2.83, 95% CI: 1.29–6.16), patients with history of sedative consumption (OR = 2.71, 95% CI: 1.35–5.47), patients using vitamin supplementation (OR = 0.21, 95% CI: 0.08–0.55), and patients with a positive familial history (OR = 2.81, 95% CI: 1.38–5.72). More than 53% of the variation in cataract development was explained by our final multivariate model (Table 2).
Factors related with the prevalence of cataract after applying multiple logistic regression.

CI, confidence interval; OR, odds ratio.
It should be noted that although aspirin had a protective effect on developing cataract (p < 0.001), controlling the effect of potential confounders showed no association between aspirin use and cataract (p = 0.162).
Discussion
This cross-sectional study was conducted in an area with Mazandarani ethnicity in north of Iran. Our study showed that approximately 30% of over 60-year-old patients referred to the study day clinic had suffered from cataract. We also found that the chance of developing cataract was more common among patients aged over 75, single patients, diabetics, patients with rheumatoid arthritis, infectious diseases, hypertension, history of ophthalmic surgery, history of using sedatives, and familial history of cataract. In addition, the odds of cataract was lower among patients using vitamin supplementation.
In a population-based study conducted by Panday and colleagues, 13 during a 6-year period among population aged over 60, the incidence of cataract was 15.62% (45 out of 359). It was lower than that estimated in this study. However, we estimated the prevalence of cataract instead of the incidence reported in their study. In diseases such as cataract, the prevalence generally represents higher estimates than the incidence. Another reason for such heterogeneity was the difference in the study populations which was clinic based in our study. Tang and colleagues reported that the prevalence of cataract (cortical, nuclear, PSC, and post-surgical) among Chinese rural residences aged more than 45 was 44% (883 out of 2006). They also reported the prevalences of cataract among patients aged 60–64, 65–69, 70–74, 75–79, and over 80 at 53.5%, 74.2%, 77.4%, 90%, and 96.2%, respectively. 14 These estimates were higher than the estimates in this study. Another population-based study in India showed the age–sex standardized prevalence of operated and non-operated cataract as 72.7%. 15 The corresponding figure in a different population-based study carried out in China was 38.1%. 16 A cross-sectional study conducted in Oman among 11,413 people in 1997 showed the prevalence of cataract as 29.3 per 1000 population. 17 Prevalence of cataract among Taiwanese people aged more than 40 during the last decade (2001, 2009, and 2013) was 10.7% (2001), 13.3% (2009), and 11.84% (2013), respectively. 18
Prevalence of cataract among 35- to 64-year-old men and women in Lithuania was reported as 17.8% and 18.6%, respectively. 19 These rates were similar to the prevalence estimated in this study. In Chinese people aged more than 30, prevalences of cataract among the total population, men, and women were 20.8%, 17.6%, and 23.6%, respectively. 20 In South Korea, 42.28% of people aged more than 40 had cataract. The corresponding rates for Korean men and women were 40.82% and 43.62%, respectively. 21 Low estrogen level during menopause may be an explanation for lower risk of cataract in women. 22
Results of previous studies reporting the related factors of cataract are presented in Table 3.13,15,21,23–29 In the study conducted by Hankinson and colleagues (nurses health cohort), during 434,680-person-year follow-up, 448 patients with cataract were diagnosed. No protective effect of aspirin consumption for at least 20 years was found in that study. 23 That was in keeping with our study in which no effect of aspirin was observed in multivariate regression models. However, in univariate analysis, a significant effect was observed. It should be noted that the Hankinson and colleagues’ 23 study was a prospective cohort which was expected to be more reliable than our cross-sectional study. In total, evidences regarding the protective effect of aspirin were low according to our comprehensive search.
Risk factors of cataract according to the results of the other studies.
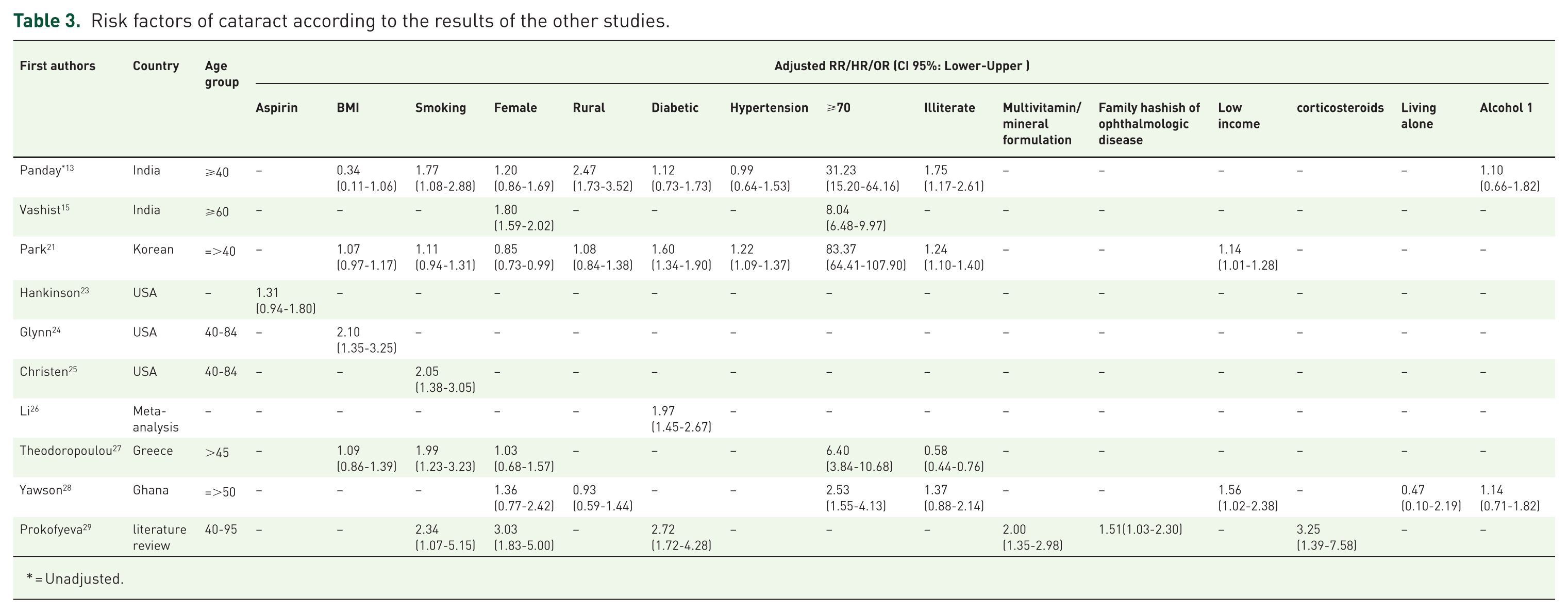
= Unadjusted.
Based on the results of the physician health cohort, BMI was a risk factor of cataract so that the risk of cataract was increased to 12% per two-unit higher BMI level. 24 This study did not show a significant effect of BMI.
Christen and colleagues indicated that in the above-mentioned cohort cigarette smoking was a risk factor for cataract which was in contrast to our results. Age difference of the study populations might be an explanation for such variation, because smoking is less common in the elderly. 25 Results of a meta-analysis showed that diabetic patients had approximately twofold higher chance of developing cataract compared with nondiabetic subjects 26 which is similar to our findings.
Results of a cohort reported an association between radiation particularly to head and neck following computed tomography (CT) and developing cataract. This study reported a 76% higher risk of cataract following imaging. It also showed that the frequency of cataract was increased with the number of CT scanning. 30 Although frequent imaging of the head increased the risk of cataract, controlling the effect of the confounders did not show a significant association.
A study carried out in Greece indicated that aging and cigarette smoking were the risk factors of cataract, while low literacy level was a protective factor. 27 Similarly, Yawson and colleagues 28 found old age as a risk factor for cataract among people over 50 in Ghana. A review study carried out in Europe showed that smoking, diabetes mellitus, multivitamin and corticosteroid consumption, female sex, and familial history of ophthalmic disorders increased the risk of cataract. 29 Finally, Park and colleagues 21 observed other factors such as low family income, low literacy level, hypertension, and old age as the risk factors for developing cataract.
This study was carried out among patients referring to a day clinic, and therefore the results might have poor reliability due to different characteristics of the study population with general population. Underestimation of some factors due to recall bias and self-reporting was another limitation of the study.
In conclusion, our study showed a relatively high prevalence of cataract in the study population. We also found aging, living alone, some infectious and noncommunicable disorders, ophthalmic surgery, sedatives, and positive familial history as the risk factors of cataract and vitamin supplements as the protective factor of cataract. Further prospective cohorts as well as clinical trials are recommended to help us in providing better estimates of the effects of these factors.
Footnotes
Acknowledgements
The authors would like to thank the research deputy of the Mazandaran University of Medical Sciences as well as the managers and ophthalmologists of the Imam Reza Clinic.
Funding
This study was carried out with Financial support of Mazandaran University of Medical Sciences, but the authors did not received financial support for the publication of this manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.