
Abstract
Background
In North Africa, where healthcare disparities are widespread, the burden of migraine is particularly underrecognized. This review explores the current landscape of migraine care in North Africa, identifying gaps in diagnosis, treatment access, healthcare infrastructure, and education, while highlighting opportunities for improvement. A narrative synthesis of recent literature, national surveys, and regional expert insights was conducted, with a focus on migraine prevalence, health system structure, treatment availability, and public awareness in North African countries. Migraine prevalence in North Africa ranges from 17% to over 30%, with most patients relying on over-the-counter medications and traditional therapies due to limited access to trained neurologists and low public awareness. Major barriers include geographic disparities, shortages in the neurology workforce, inadequate training at the primary care level, and financial constraints. Specialized headache services remain scarce outside capital cities.
Conclusion
Improving migraine care in North Africa requires integration into primary care, expanded specialist training, digital health solutions, and culturally tailored advocacy, supported by regional collaboration and research.
This is a visual representation of the abstract.
Introduction
In spite of the fact that migraine is one of the most prevalent neurological disorders globally and that it contributes significantly to disability being ranked as the second leading cause of years lived with disability (YLDs), 1 migraine remains underdiagnosed, undertreated, and inadequately understood in many regions, especially in low- and middle-income countries.
Although migraine is increasingly recognized as a major health issue, region-specific data from North Africa remains limited with scarce data on migraine prevalence, diagnosis, and treatment. North Africa region includes the northern portion of the African continent, which is a unique region bridging the Arab world and Africa from East and Europe and Africa from West regions. It includes Egypt, Libya, Sudan, Morocco, Algeria, Tunisia, and Western Sahara.
In the analysis of Global Burden of Disease 2019 data, examining the neurological disease burden across 21 countries in North Africa and the Middle East between 1990 and 2019 found that migraine was the second leading cause of Disability-Adjusted Life Year (DALYs) in persons 20–59 years of age in the region, following stroke. The age-standardized DALY rate for migraine was 601.4 per 100,000 population, the highest among all global super-regions and the burden of migraine (DALYs, YLDs, incidence, and prevalence) was more than doubled between 1990 and 2019. They also reported that unlike conditions such as stroke or epilepsy, migraine-related DALY rates did not decrease over time and that the increase reflects a rising burden of YLDs associated with migraine, rather than mortality. 1
This region presents unique challenges and opportunities in migraine care due to socioeconomic conditions, varying levels of healthcare infrastructure, high rates of consanguinity increasing the likelihood of multiple family members being affected by migraine and cultural and religious attitudes and beliefs toward health especially headache.
This review explores the current state of migraine care in North Africa, identifies key challenges, and proposes locally relevant strategies to improve care. By examining the current state of migraine diagnosis, treatment, and healthcare infrastructure, this review will highlight the current status and gaps of migraine care as a proposal for improving care for migraine patients. This will help guide future research, policy decisions, and support healthcare professionals in the region thus improve migraine management.
Epidemiology of migraine in the North Africa
Accurate data on the epidemiology of neurological disorders especially headache in developing countries remain scarce, largely due to limited healthcare resources and a shortage of trained health professionals and neurologists. 2 A recent population-based national survey conducted in 2024 in Morocco using the Global Campaign against Headache methodology found that 30% of adults needed migraine-specific healthcare, suggesting a major mismatch between need and access where access remained limited. The study also calculated that 7.0–8.4% of all time in the population was lost to headache-related disability (across paid work, household tasks, social/leisure activities). Chronic headache (≥15 days/month) was reported in 10.5% of participants, and approximately 30% of the adult population were estimated to require headache-related clinical care. 3
In Egypt, migraine prevalence is 17–20.9%, but access to specialized care is limited outside major cities such as Cairo and Alexandria.4,5 In two studies conducted in two different Egyptian governorates (Fayoum and Assiut governorates), over 60% of migraine sufferers did not seek medical advice, relying instead on over-the-counter (OTC) painkillers and believing headaches to be incurable.6,7 In Upper Egypt regions, care often falls to non-neurologist practitioners (e.g., family medicine, ENT, ophthalmology), leading to significant diagnostic and treatment gaps. 8 Preventive migraine treatments are provided to only about 8.5% of patients in some local studies. 6
A recent national cross-sectional study by Amir et al. 4 in Egypt reported a migraine prevalence of 20.9% among Egyptian adults, with nearly half of patients experiencing severe disability and high rates of comorbid insomnia, depression, and anxiety. This study provides foundational data underscoring the seriousness of migraine as a major public health issue in Egypt. The recent study on the burden of hidden migraine across eight Arab nations, including Egypt, Libya, Algeria, and Sudan, demonstrated that more than two-thirds of migraineurs experienced moderate to severe disability, underscoring the widespread under recognition of migraine in the region. 9
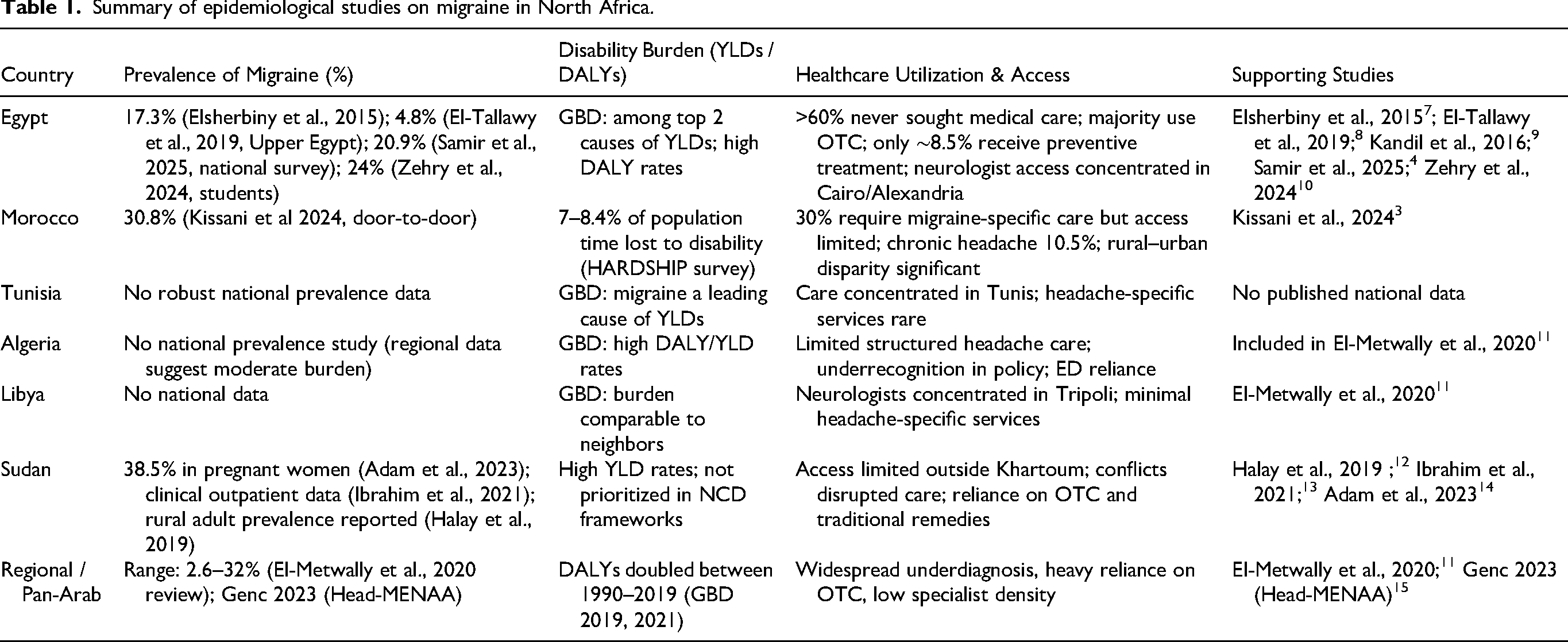
Table 1 summarizes the available epidemiological studies from North Africa. This table highlights the absence of comprehensive national studies on migraine in several North African countries, notably Libya and Tunisia, where published data remains unavailable.
Summary of epidemiological studies on migraine in North Africa.
Healthcare infrastructure
The healthcare services in North African countries, in general, face significant challenges despite the high burden of the disease. This might be mainly due to financial constraints and inequitable access to medical services, particularly in rural and underserved areas.
In migraine care, healthcare services in North Africa are generally structured within a tiered system; however, significant gaps and imbalances persist across all levels. Primary care services often lack adequate training in headache diagnosis and management, leading to frequent underdiagnosis or misdiagnosis of migraine. Due to physician shortages and system inefficiencies, many migraine patients turn to pharmacists or traditional healers for symptom relief. This often leads to overuse of analgesics and increased risk of medication-overuse headache (MOH).
Referral pathways to specialized care are frequently inefficient or unclear, and access to neurologists or headache specialists is limited, especially outside major urban centers. At the tertiary level, while some academic and private institutions offer more specialized services, these are typically concentrated in capital cities and are inaccessible to large segments of the population due to financial, geographical, or systemic barriers with neurologist density remaining low, with long waiting times for consultations. This fragmented structure contributes to delayed treatment initiation, suboptimal care, and a high burden of disability among migraine patients.
The structure of migraine care in North African countries generally follows a tiered model (Figure 1).

A flow diagram of patient care pathways in North Africa.
Initial Point of Contact: Pharmacies and Self-Care: For the majority of individuals, the patient journey begins with self-treatment using OTC analgesics. Community pharmacies are the most accessible and frequently used resource, where pharmacists provide initial advice and medication using especially the cheaper options.
Primary Care Physicians: When OTC treatments fail, patients may seek help from a general practitioner (GP). Primary Care Physicians manage a large volume of migraine cases but often face challenges due to limited specialized training in headache disorders. This contributes to underdiagnosis, misdiagnosis, or suboptimal treatment with adding burden on migraine stigma plus risk of MOH. Specialized Neurological Care: Patients with severe, chronic, or treatment-resistant migraine are referred to neurologists. Access to this level of care is highly concentrated in major urban centers such as Cairo, Alexandria, Tunis, Algiers, and Rabat, where specialized neuroscience centers and dedicated headache clinics are more likely to be found especially in university-based clinics. These facilities offer advanced diagnostic tools and a broader spectrum of therapeutic options. Advanced and Multidisciplinary Care: In a very few highly specialized centers, a multidisciplinary approach may be available, involving neurologists, pain management specialists, physiotherapists, and psychologists. For the most intractable cases, advanced options like neurosurgery might be considered, though this is very rare if any in some countries.
Geographic Disparities:
Urban–rural divide: Specialized neurological care is concentrated in major cities (e.g., Cairo, Rabat, Algiers), leaving rural and remote populations underserved. A comprehensive survey of neurological services across 50 African countries revealed a stark urban–rural imbalance, with neurologists predominantly based in capital cities and major metropolitan areas leaving vast segments of the population underserved in rural areas.
16
Neurology Workforce Shortage:
Improving access to migraine care in North Africa is closely tied to the development and distribution of a well-trained healthcare workforce. However, the region faces several systemic challenges that limit the effectiveness of current human resources in addressing the high burden of headache disorders.
Across North African countries, the number of neurologists per capita is significantly below global averages. The median number of neurologists per 100,000 population is very low in Africa (0.03 vs. 4.84 in Europe). 16 A study done by Kissani and his colleagues in Africa 17 suggested that African nations could be divided into four levels according to the number of neurologists per nation (From level A with the highest number of neurologists [more than 201 neurologists per country] to level D with the lowest number [no neurologists]). Most neurologists are concentrated in large cities and university-affiliated hospitals, leaving rural and underserved regions with minimal or no specialist coverage. This urban bias creates long waiting times and significant geographic barriers for patients seeking migraine care. In Egypt, while tertiary centers in Cairo, Alexandria and six other governorates provide neurological care, many rural governorates lack consistent access to neurologists. In Morocco and Tunisia, neurologists are mainly clustered in capital regions, and headache-specific services are rare even in specialist clinics.
Inadequate primary care capacity
Most GPs and even neurologists receive little to no structured training in headache diagnosis or management. Undergraduate and postgraduate medical curricula in the region often lack dedicated modules on headache medicine, and continuing medical education (CME) opportunities remain scarce. A 2024 Moroccan study noted that even in tertiary centers, few providers routinely use standardized diagnostic criteria such as International Classification of Headache Disorders, 3rd edition ICHD-3. 3
General practitioners and frontline providers often lack training in evidence-based migraine care, leading to underdiagnosis and misuse of treatments. Also, a survey done in Egypt suggested that many GPs are unaware of evidence-based treatment pathways for acute and preventive migraine management. 18
Gender inequities
Migraine disproportionately affects women, yet cultural norms and healthcare access barriers may delay or prevent care-seeking, particularly in rural or conservative areas.
A study in three Upper Egypt villages, when testing barriers to basic health services provided to females in general, found 30% of women cited distance and transportation issues, over 40% cited high cost, and about 25% needed family permission or were deterred by lack of female physicians when seeking basic healthcare. While not migraine-specific, it demonstrates how sociocultural and structural barriers hinder women's general access to care—relevant to migraine care too. 19 Women also report poverty, low education levels, and restricted mobility as key impediments to accessing health services. 20
Financial and insurance limitations
Out-of-pocket costs dominate healthcare spending in many North African countries. Headache care is rarely prioritized in public insurance schemes, and many cannot afford preventive therapies, neurologist consultations or even GP.21,22
Social stigma
Migraine is still widely misunderstood as a nonserious condition. This reduces both the demand for and investment in care infrastructure and may cause patients to avoid seeking care due to fear of dismissal or misdiagnosis.
Availability and use of evidence-based treatments
Table 2 listed all evidence-based migraine treatments, showing whether the treatment is available, reimbursed, or has any within-country/region variability considerations in North Africa.
List of all evidence-based migraine treatments within North African countries.

Sociocultural barriers
Due to out-of-pocket medicine and lack of awareness, many individuals turn to traditional remedies, including Hijama (wet cupping), 23 which is widely practiced for headache relief across the region, being particularly popular in Egypt, Morocco, Algeria, and Sudan. 24 It has also religious background in some countries. Very few studies were conducted on Hijama with one study demonstrating a 66% decrease in headache severity in migraine and tension type headaches after wet cupping therapy compared to baseline measurements. 23
Tying cloths around the head tightly is used by a widespread folk practice to relieve throbbing or pulsating pain. This was first started in Ancient Egyptian remedies and were written in Papyrus with a small crocodile around the tying cloth. 25
Herbal medicine—such as preparations of nigella sativa (black seed), peppermint, and ginger—is also commonly used, often based on generational knowledge rather than clinical evidence.
Acupressure and Head Massage (Ruqyah-based) performed at specific “energy” or pressure points; sometimes done with Quranic recitation (Ruqyah) for spiritual and physical relief.
These practices vary significantly by region, with higher reliance in rural and conservative communities where access to neurologists and preventive medications is limited. Cultural beliefs and the stigma surrounding neurological disorders further influence treatment-seeking behavior, often delaying access to evidence-based care.
While traditional approaches such as hijama, herbal remedies, and spiritual healing remain culturally significant and widely practiced, current international guidelines (International Headache Society [IHS] and European Headache Federation [EHF]) emphasize that these methods lack robust evidence and should not replace established, evidence-based therapies for migraine.
Advocacy, initiatives and future plans
Education in migraine
Although education in headache and migraine for GPs and neurologists has improved within the last decade, a number of challenges / gaps remain.
The Headache Chapter of the Egyptian Society of Neurology, Psychiatry, and Neurosurgery (ESNPN) actively organizes prominent events centered on migraine management, including the annual MENA Headache Conference and EgyHeadache conference. The 5th EgyHeadache conference took place in June 2025 in Cairo. In 2018, the society launched the public awareness campaign “Migraine is Not Just a Headache,” which engaged regional experts and leveraged social media platforms such as Facebook and Instagram. The campaign also enlisted key opinion leaders and celebrities to enhance visibility and motivate public engagement.
Additionally, the Education in Headache for Healthcare Professionals in Africa (EHHPA) is a free, annual virtual symposium aimed at building clinical capacity across the continent, including North Africa. The program focuses on headache classification, diagnosis, treatment, and advocacy. Since its inception in 2021, EHHPA has been supported by the African Academy of Neurology, the World Federation of Neurology, and the IHS. It attracts a wide range of participants—including neurologists, trainees, GPs, and nurses.
North African neurology residency programs (e.g., Cairo University, Tunisian institutes) offer general neurology training, but structured headache-specific modules or fellowships are not standard. The Egyptian Headache Chapter under ESNPN is the only regional body specifically focused on headache education and advocacy in North Africa, though it offers no formal certification pathway, and there are currently no nationally recognized certifications in headache medicine in North Africa, and most neurologists gain headache expertise through general training or informal mentorship rather than formal credentials.
Advocacy and initiatives
The IHS has supported migraine-friendly environment awareness campaigns all over the world. In Egypt and Morocco, this initiative was implemented in collaboration with local professional societies such as the ESNPN and included outreach through media, educational materials, and policy discussions.
Egypt:
Public Awareness Campaigns: The “Migraine is Not Just a Headache” campaign launched in 2018 by the Headache Chapter of the ESNPN aimed to reduce stigma, educate the public, and encourage early diagnosis and treatment. This campaign leveraged social media (Facebook and Instagram) and featured local celebrities, neurologists, and key opinion leaders to increase its reach. Cultural Barriers: Migraine is increasingly recognized as a disabling neurological disorder, particularly in urban centers. However, it remains underprioritized in national healthcare policy, with little integration into chronic disease programs or insurance coverage schemes. For only one year, the anti-CGRP was supported in university insurance and then withheld due to financial constraints. Advocacy and Policy Engagement: Egyptian neurologists have advocated for inclusion of migraine in primary healthcare algorithms and the expansion of neurology residency content to cover headache management more comprehensively.
Morocco
Public Awareness Campaigns: Migraine awareness events are occasionally held in major hospitals in Rabat and Casablanca, often around International Migraine and Headache Awareness Week. These are typically sponsored by the Moroccan Society of Neurology and pharmaceutical companies. Cultural Barriers: Migraine is often underreported due to stigma, especially among women. Cultural beliefs may delay care-seeking, with preference given to traditional medicine (herbal infusions, cupping, or talismans) before biomedical consultation. Advocacy and Policy Engagement: Morocco lacks a national headache strategy, and neurologists are unevenly distributed, making access to specialized care difficult in rural areas.
Algeria
Public Awareness Campaigns: Migraine is still viewed by many as a minor ailment rather than a neurological condition. Although some urban clinics have dedicated headache services, headache is not formally included in national health strategies. Advocacy and Policy Engagement: Headache-related content is occasionally included in national neurology conferences and CME sessions. No large-scale national awareness campaigns have been reported.
Sudan
Public Awareness Campaigns: Public migraine awareness is low, particularly outside Khartoum. Limited internet access and sociopolitical instability restrict media-based campaigns. Advocacy and Policy Engagement: Headache disorders are not considered a priority in the national noncommunicable diseases’ (NCD) framework. Also, due to political conflicts, no medical care was available for the last couple of years.
Libya and Tunisia
Public Awareness Campaigns: There are few to no published reports on public migraine awareness or structured advocacy initiatives. Neurological services are largely urban-based (Tripoli, Tunis), and migraine receives minimal political or media attention. Advocacy and Policy Engagement: In both countries, awareness of migraine as a disabling condition remains low, and cultural normalization of chronic headache among women continues to delay diagnosis.
Future Directions:
Suggested plan includes:
Highlight telemedicine initiatives as a feasible means of bridging the urban–rural care gap, referencing examples of teleneurology programs piloted in Egypt and Morocco. Emphasize regional training collaborations, such as the EHHPA program, which provides structured headache training accessible to GPs and neurology residents across North Africa. Recommend integration of headache care into existing NCD programs, drawing parallels with how hypertension and diabetes care models have been scaled in primary care networks. Create National Programs for Headache Disorders It's time for migraine and other headache conditions to be officially included within national strategies tackling chronic diseases. Each country should work toward its own set of practical, resource-aware clinical guidelines for both acute and preventive treatment. Cooperation with Ministries of Health is essential to bring headache care into the primary care level, where most patients first seek help. Strengthen Specialist Networks Across the Region Some countries in the region still lack organized headache societies. We need to support the formation of these groups where they're missing and enhance the work of existing bodies—like Egypt's Headache Chapter under ESNPN. In addition, creating certified headache training programs or fellowships for GPs and neurologists, especially with support from bodies such as IHS or EHF, will help expand the number of trained specialists. Use Telemedicine to Close the Urban–Rural Gap Most specialized care is found in capital cities, leaving remote areas underserved. By expanding tele-neurology and launching e-consultation services, we can allow GPs in rural clinics to access expert advice and improve care quality without requiring patients to travel far. Embrace Digital Tools and AI Technology can help where human resources are limited. We should support the development of digital tools that assist primary care doctors in diagnosing and managing headache disorders. AI and machine learning also have the potential to identify regional trends in migraine patterns and treatment response—this is an area North African researcher should start engaging with more actively. Improve Training and Public Awareness Headache medicine should be a formal part of undergraduate and postgraduate medical education. On the community level, more outreach is needed through culturally appropriate education campaigns—whether through local workshops or affordable brochures in Arabic and French those explain what migraine is and how it can be treated. Encourage Local Research and Data Collection There's a clear lack of structured data on migraine care and outcomes in the region. We need collaborative projects to establish regional headache registries and push for funding to support population-based studies, especially in countries such as Libya and Sudan that remain underrepresented in the literature. Acknowledge and Study Traditional Practices Many patients in North Africa turn to traditional treatments such as hijama (wet cupping), herbal remedies, or essential oils. Rather than ignoring these, we should study them properly to assess their safety and efficacy. If proven useful, they can be incorporated into broader care plans in a way that respects both evidence and culture.
Conclusion
In North Africa, migraine continues to be largely overlooked and poorly managed, even though it places a heavy burden on people's lives—especially women and those living in rural or underserved areas. Challenges such as limited resources, unequal access to care, and low public awareness persist. Still, there is real potential to make meaningful improvements. By including migraine in broader health policies, training more specialists, using digital and telehealth tools, and respecting local cultural approaches to care, we can take important steps toward better and fairer treatment. Collaborating across countries in the region and building research tailored to our populations will be key to lasting progress.
Public health relevance
Migraine remains underdiagnosed and undertreated across the region.
This review presents an overview of the healthcare infrastructure, workforce, and treatment availability for migraine in North African countries.
Barriers to care include limited access to neurologists, urban–rural disparities, gender inequities, and underuse of evidence-based treatments.
Traditional medicine and sociocultural beliefs often influence health-seeking behavior, especially in underserved populations.
National headache strategies, improved medical education, and the adoption of telemedicine are urgently needed to improve migraine care.
This is the first regional review focusing specifically on migraine services in North Africa and offers recommendations tailored to the local context.
Footnotes
Ethical considerations
Institutional Review Board approval was deferred for this narrative review paper.
Consent for publishing
Yes.
Author contributions
The author was the only contributor to this manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used for this article may be obtained from the author with a reasonable request.