
Abstract
Background
Headaches are more prevalent in women, causing male underrepresentation in studies. This study aimed to characterize men with headache at two tertiary headache clinics (one public, one private) and explore sex differences.
Methods
Retrospective exploratory study. Sociodemographic and clinical data, including ICHD-3 diagnosis and treatment, were collected from clinical files of patients’ consultations between nov/2023 and nov/2024.
Results
Among 700 patients, 112 (16.0%) were men. Men were older at first appointment (48.2 vs 42.6 years, p < 0.001), had later symptom onset (36.0 vs 26.4 years, p < 0.001), more often unfulfilled specific headache diagnostic criteria (10.7% vs 8.3%, p < 0.001) and had higher frequency of trigeminal autonomic cephalalgias (20.4% vs 1.3%, p < 0.001) and cranial neuralgias/facial pain (9.0% vs 2.9%, p = 0.003), the latter explained by a higher age at symptom onset at a regression analysis. Men were more likely to have no preventive medication prescribed (36.6% vs 21.4%, p = 0.001) and less often overused analgesics (10.5% vs 28.1%, p < 0.001). Migraine was the most common diagnosis (42.0% men vs 73.3% women), with less chronic migraine in men (16.7% vs 37.6%, p = 0.004).
Conclusions
Findings reveal sex differences in age, diagnoses, and treatment, highlighting the need for sex-focused research and personalized clinical approaches.
This is a visual representation of the abstract.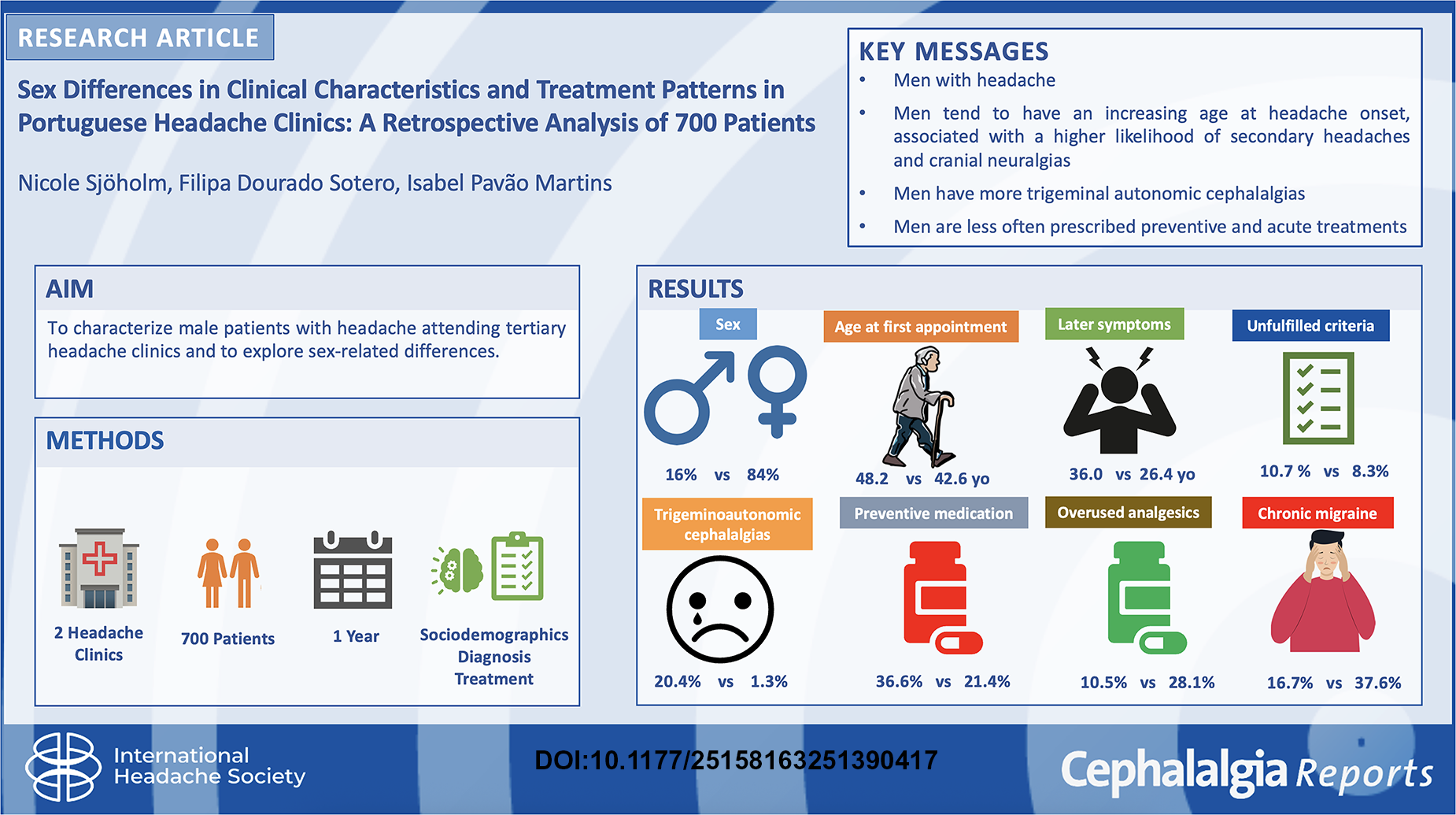
Introduction
Primary headaches are more prevalent in women,1–3 except for cluster headache,1–4 and these differences have been related to numerous factors such as sex hormones, the calcitonin gene-related peptide (CGRP) and even brain structure. 5 A recent systematic review reported that migraine is three to four times more prevalent in women than men after puberty, with women experiencing more severe, longer-lasting attacks and greater disability, differences likely influenced by hormonal fluctuations, though mechanisms remain unclear. 6 This was the only systematic review that specifically addressed this topic, underscoring the scarcity of research and reinforcing the need for the present study.
Less is known about sex differences in rarer or secondary headaches. Moreover, social stigma—headache often seen as a “female disorder”—may contribute to underdiagnosis and reduced healthcare-seeking among men, 7 leading to their underrepresentation in consultations and research.
This study aims to characterize a sample of male patients followed in two tertiary headache clinics, hypothesizing a different distribution of diagnoses and treatment.
Methods
This retrospective observational study was conducted in two tertiary headache centers in a public and a private hospital. The study was exploratory with the primary aim of comparing sex differences in headache clinical features that could generate further hypothesis. No formal a priori hypothesis was defined, and therefore a sample size calculation was not conducted beforehand. Since we verified an approximate male-to-female proportion of 1:10, we established that the study should enroll at least 100 male patients to enable statistical comparison.
Clinical data was extracted from clinical records from the most recent consecutive patients attending specialized headache consultations, starting in November/2024 and going backwards until November/2023. All adult patients (≥18 years) with headache were included regardless of having an established diagnosis. Variables recorded were: sex, occupation, age at headache onset, age at first consultation, diagnosis established by neurologist according to ICHD-3 8 and treatment. Patients with multiple headache diagnoses were counted and each diagnosis was recorded in a separate line to allow for the comparison of all diagnosis (number of diagnoses was superior to the number of patients). For migraine, additional data included aura, episodic vs chronic subtypes, and prescribed acute/preventive medication. Broad onset age terms (e.g., “childhood,” “adolescence”) were standardized (e.g., 10 or 15 years). Data from the most recent and complete visit was prioritized.
Data was analyzed with IBM SPSS Statistics (v29). Descriptive statistics were used, with continuous variables presented as mean, standard deviation (SD) or median and interquartile range. Categorical variables were reported as counts and percentages. Group comparisons were performed using Chi squared test, Student's t-test, or Mann–Whitney test. Missing values for each variable were compared between males and females for significant differences (Table 1). Statistical significance was set at p < 0.001 (two-tailed) with 95% confidence intervals to account for the number of comparisons performed. A post hoc regression analysis was performed to find explanatory factors for specific findings.
Demographics, clinical features and treatment characteristics of patients according to sex.
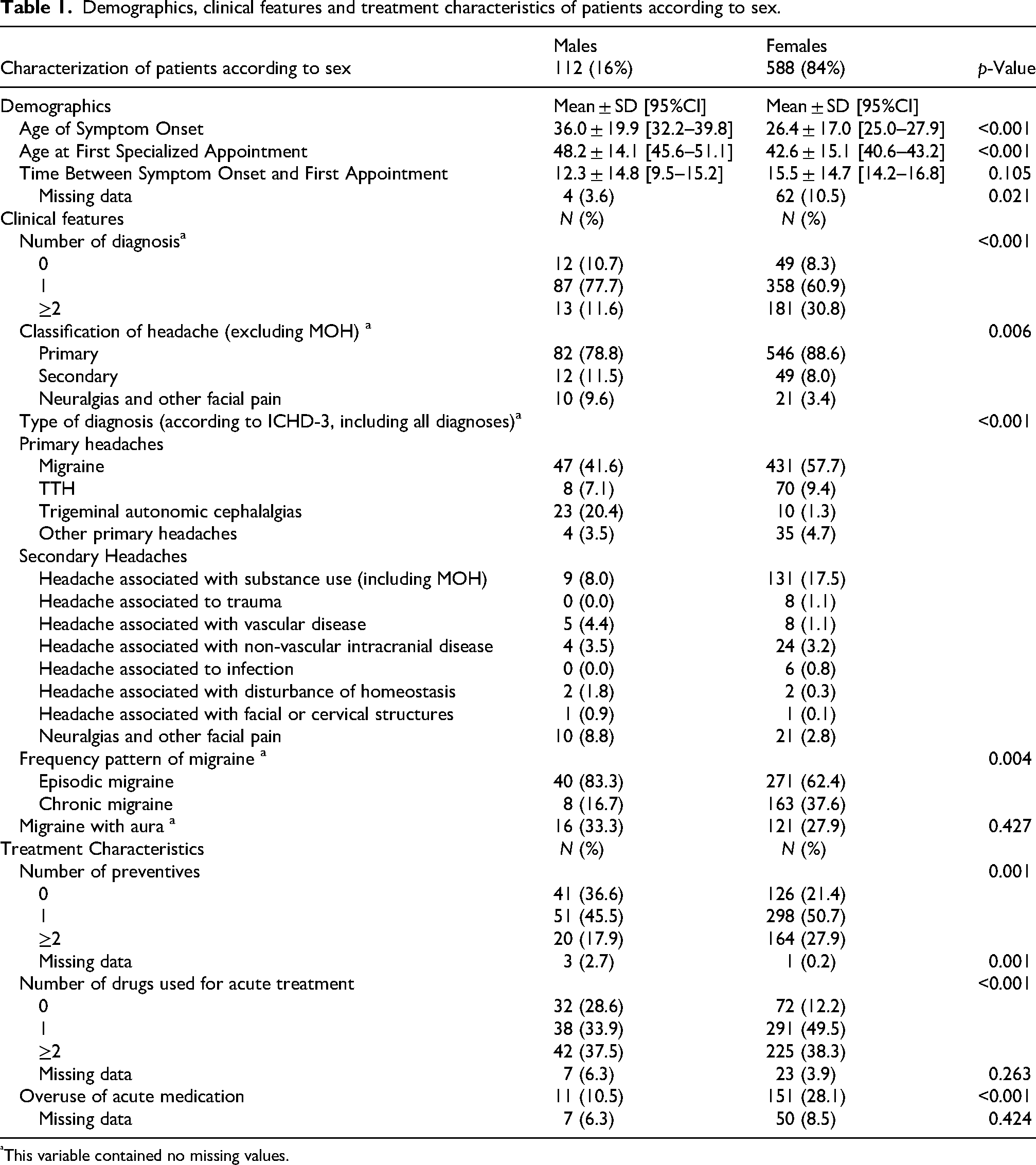
This variable contained no missing values.
Results
A total of 700 patients were included, 16% men, whose proportion was significantly higher in the private (26.3%) compared to the public hospital (12.2%) (p < 0.001). There were several sex-related differences in the clinical features (Table 1).
Male patients were on average 10 years older than females at symptom onset and 6 years older at the time of first appointment, regardless the healthcare setting. The interval between symptoms onset and first visit was similar among sexes. Men more frequently lacked an established diagnosis.
Women had a higher frequency of migraine while men presented higher rates of trigeminal autonomic cephalalgias and neuralgias (Table 1). Medication overuse was more common in females and, after excluding it (since it is typically a consequence of a primary headache disorder), there was a significant difference between men and women in the secondary headaches (11.5% men vs 8% women) and cranial neuralgias (9.6% vs 3.4%, respectively) compared to primary headaches (p < 0.006).
Men reported a lower percentage of prescribed preventive and acute treatment compared to women, being more likely to take no preventive medications and no acute medications.
Regarding migraine, men showed significantly less chronicity, but no differences in aura (p = ns). Preventive drugs differed between sexes (p < 0.001), with male preponderance regarding antihypertensives (16.7% vs 9.1%), such as angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, calcium channel blockers (11.5% vs 5.2%), and Gepants (9.0% vs 2.3%), but lower use of Anti-CGRP mAbs (monoclonal antibodies) among men (2.6% vs 8.1%).
For acute treatment, men presented a higher prescription of triptans (58.4% vs 44.9%, p = 0.002) and gepants (6.5% vs 2.8%, p = 0.002) than women.
Two binary logistic regressions were undertaken to verify if sex was the main explanatory factor for secondary headaches in general (compared to primary, after excluding MOH) and for cranial neuralgias (compared to primary headaches). Diagnostic group was entered as the dependent variable. Sex and age of symptom onset and age at first consultation were entered as independent variables. For cranial neuralgias, a higher age of onset (51.70 ± 17.98 vs 24.16 ± 15.3 years, on average) was the main explanatory factor (OR = 1.077, p < 0.001 [95% CI 1.074–1.121]), rather than sex (OR = 0.412, p = 0.037 [95% CI 0.179−0.148]) or current age. A similar result was obtained for secondary headaches, with higher age at onset (39.73 ± 19.78 years in secondary vs 24.16 ± 15.26 years in primary) being the only significant factor (OR = 1.066, p < 0.001 [95% CI 1.039–1.094]), but not sex nor age at consultation.
Discussion
The present results indicate several differences between men and women attending tertiary headache clinics. Men represent a small proportion of patients, report a later symptom onset, are less likely to fulfill criteria for a specific diagnosis, have a different proportion of trigeminal autonomic cephalalgias and cranial neuralgias/facial pain, fewer drugs prescribed, and tend to have less chronic migraine.
This study confirmed a strong female predominance in headache consultations, with a male-to-female ratio of 1.5:10, consistent with the higher global prevalence of headache disorders, especially migraine and TTH in women.1–3
Regarding age at symptom onset and seeking medical care, male patients were older than females at both time points, consistent with migraine studies showing a peak prevalence in women that coincides with cyclic hormonal changes during adolescence and early adulthood, while men's migraine has a fluctuating nature with longer remissions alternating with relapses. 2 Despite evidence that men are less likely to seek care, 9 both sexes sought or were referred to specialized consultation after a similar delay. Patients may have consulted other clinicians beforehand, but this information was not systematically recorded. Future prospective studies with targeted data collection could clarify prior healthcare-seeking behaviors.
In our study, men were more likely to lack an established diagnosis, echoing findings from the CaMEO study, where men were less likely to be diagnosed with migraine despite seeking care. 9 Although our sample included other headache types, the trend persisted. Since both men and women were observed by the same clinicians, this difference may eventually reflect more atypical presentation, or reduced symptom reporting by men, confounding diagnoses—patterns previously noted in migraine. 10 Furthermore, the higher prevalence of rarer headache types among men may contribute to delayed diagnosis, particularly in settings less familiar with these conditions.
Men also used fewer preventive medications, consistent with previous migraine research.5,9 This may indicate milder disease, lower impact of headache or easier symptom control, aligning with prior evidence of a lower risk of migraine recurrence in this group. 1 However, since standardized impact questionnaires were not systematically gathered, we cannot attribute a specific explanation for this finding. Similarly, men also used fewer acute medications, reinforcing the pattern of lower overall treatment in this group.
Notably, men had a higher proportion of cranial neuralgias and secondary headaches in general when MOH was excluded. As these are linked to identifiable underlying causes, they may be more preventable with appropriate management. However, these differences seemed to be driven by a higher age at symptom onset. It may also mean that patients with a higher age (difficult to define, but well under 65 years old) presenting in headache clinic may warrant particular attention due to possible more serious underlying conditions. Given that some specific diagnoses were found mainly among male patients—namely, headache attributed to carotid artery dissection, arteriovenous malformation (AVM), intracranial glioma, and sleep apnea—the identification of associated risk factors may be crucial. However, potential vascular risk factors were not systematically assessed in our study, due to its exploratory nature without a priori hypothesis.
In what concerns migraine, it is thought that the pathophysiology of sex-related differences in chronic migraine is associated with the impact of sex hormones, neural substrates, and neuroendocrinology, such as the higher CGRP levels in women than in men. 11 We observed that chronic migraine was significantly more frequent in women, consistent with known associations in episodic-to-chronic conversion.11,12
The higher prescription of antihypertensive preventives in men may reflect either an avoidance of adverse events of other prophylactics, its prescription for concurrent hypertension, or lower response to other drugs, which was not specifically sought.5,11
Triptans are indicated for severe migraine attacks or when NSAIDs are ineffective, based on level A evidence. 13 Interestingly, men reported greater triptan use—contrasting with prior studies showing higher use among women. 11 Despite known pharmacokinetic differences between sexes, achieving higher plasma concentration values in women, 5 outcomes appear similar, 14 therefore we consider that this disparity may be explained by differences in prescription patterns or in triptans’ access, which may vary across countries or healthcare systems.
Since it has been previously shown that CGRP participates in the pathophysiology of migraine, the development of CGRP-targeted therapies has been met as a promising therapeutic approach for migraine. Gepants are alternative to triptans to mitigate adverse effects. 13 In this study, men had more gepants but less mAbs prescribed as preventive treatment. This may relate to the earlier introduction of mAbs compared to gepants, and their preferential prescription to chronic resistant migraine, more common in women. However, it also reinforces the need to assess sex-specific preferences and response, considering the sexual dimorphism of the trigeminovascular pathway, which plays a significant role in CGRP release. 15 A recent study in male and female rats found that females’ trigeminal ganglia express significantly higher mRNA levels of RAMP1, a key CGRP receptor component, suggesting a potentially greater treatment response in females. 16 Additionally, gepants versus mAbs prescription may be related to availability and cost barriers since, at the time of data collection, the cost of gepants was not reimbursable in the healthcare system this study was conducted at (University Neurology Clinic).
A key strength of this study is its large, well-defined sample, with all patients diagnosed by a neurologist using ICHD-3 criteria, ensuring diagnostic accuracy. The focus on sex-based differences in headache characteristics and care addresses the common underrepresentation of men, with a substantial male cohort. Including a wide spectrum of headache types provides a more comprehensive understanding of headache disorders, including rarer and less studied forms.
As a retrospective observational study, causality cannot be inferred. The sole reliance on clinical records is a limitation, as data quality depends on patient self-report, clinician documentation, and researcher interpretation. It is also important to note that patients referred to specialized headache centers often have more complex, refractory, or chronic headache conditions, which may contribute to selection bias and limit generalizability, especially regarding healthcare systems in which referrals process may differ from the one in Portugal, where patients are referred to public hospital after failed primary care/general neurology management, while patients can access directly private hospital (Figure 1). Additionally, given that this is a two-center study, the generalizability of the findings may be limited.

Flow diagram: patient enrolment with Portuguese healthcare system.
The absence of standardized and validated headache impact measures—such as the Migraine Disability Assessment score or the Headache Impact Test—represents a limitation, not allowing a meaningful comparison of headache burden. However, these are not systematically used in consultations nor registered on clinical records.
We also recognize limitations regarding statistical analysis, namely the risk of type I error due to the multiple pairwise comparisons. We addressed this by adjusting the p-value for multiple comparisons. Additionally, results may have been influenced by the handling of missing data, as some sex differences were observed regarding prescribed preventive and acute treatments. However, the analysis of missing data per sex can provide valuable information. It may imply that either data gathering may be more difficult in men or that the significance patients attribute to information is different. We acknowledge that some findings—particularly those from subgroup comparisons—should be interpreted with caution and considered preliminary, warranting confirmation in future studies with appropriate design and statistical control.
Conclusions
These results demonstrate sex-related differences in the age of symptoms onset, diagnostic proportions and treatment patterns among patients with headache, highlighting the need for more studies that include sex and age as variables. They also underscore the importance of physicians being aware of these sex differences in clinical practice, in order to proportionate a more individualized approach to these patients.
Highlights
Men were less likely to have an established diagnosis.
Men tend to have an increasing age at headache onset and this is associated with a higher likelihood of secondary headaches and cranial neuralgias.
Men preponderance was seen among trigeminal autonomic cephalalgias.
Men were less frequently prescribed both preventive and acute treatments.
Footnotes
Abbreviations
Ethical considerations
This study was conducted in agreement with its protocol and complying with the Declaration of Helsinki, the good clinical practice and all applicable regulations and laws. All patient-level identifiers were codified for deidentification to protect patients’ privacy. The local ethics committees of both hospitals authorized the study protocol (licenses no 276/24 and 14/2024/47635239).
Consent to participate
The need to obtain patients’ consent was waived.
Consent for publishing
Yes.
Author contributions
NS collected data, built the database, and wrote the manuscript. IPM also contributed to data collection. All authors contributed to statistical analysis, read, reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Pseudo-anonymized datasets created and/or analyzed during the current study are only available from the corresponding author on reasonable request.