
Abstract
Background
Many studies have found that migraine with aura (MA) is a risk factor of stroke, but the relationship between stroke and migraine without aura and tension-type headache is unclear. The aim of this study was to investigate whether primary headache disorders, including subtypes of migraine, increase the risk of ischemic or hemorrhagic stroke.
Methods
This large population-based 13-year follow-up study used baseline headache data from the third Trøndelag Health Study (HUNT3) performed between 2006 and 2008. The HUNT3 headache data were linked to the Norwegian National Stroke Register that includes stroke diagnoses recorded from 2013 until December 2021. The association between stroke and headache status was investigated in individuals aged ≥20 years without stroke at baseline. Prospective associations were evaluated using multivariable Cox proportional hazard models with 95% confidence intervals. Separate sub-group analyses by age and sex were performed.
Results
Among 37,364 included participants, 50% were younger than 55 years. A total of 1095 (2.9%) developed stroke after a median of 9 years. In the multi-adjusted model, reporting MA at baseline was associated with increased risk of stroke at follow-up (HR 1.59, 95% CI 1.14–2.21) compared with those without headache. The increased risk of stroke was most evident among individuals <55 years with MA (HR 2.18, 95% CI 1.24–3.82) and among women (HR 1.70, 95% CI 1.12–2.59). Migraine without aura (MO), tension-type headache (TTH) and unclassified headaches were not associated with increased risk of stroke.
Conclusions
During 15 years of follow-up, individuals with MA were more likely to suffer from stroke compared to those without headache. The relationship with MA was even stronger in women, and for young individuals aged <55 years. Individuals with MO or TTH were not associated with increased risk of stroke.
Introduction
Migraine is a primary headache disorder holding the second place for the most common cause of disability, and takes the first place for women under 50 years. 1 Likewise, stroke is the second leading cause of death and the third most common cause of disability. 2 As a leading cause of disability, both migraine and stroke have a substantial impact on the quality of life and have considerable burden to the society.3,4
Increasing number of studies have investigated the associations between migraine and stroke, and many studies, including two meta-analyses have reported increased risk of stroke among individuals with migraine with aura (MA).5–10 Greater risk of stroke was particularly found in individuals aged less than 45 years, women, oral contraceptive users, and smokers. 6 A recent follow-up study from South Korea that included individuals aged >40 years also showed 35% greater risk among migraineurs. 11 The mechanisms that link migraine to stroke is complex and incompletely understood. Shared pathological mechanisms have been suggested justified by shared genetic risk factors, cortical spreading depression, hypercoagulation, vasospasm, endothelial dysfunction, and higher prevalence of traditional cardiovascular risk factors both in migraine and stroke.12,13
The association between stroke and headache types including migraine without aura (MO) and tension-type headache (TTH) and in sub-group of population by age and sex is less clear. Migraine is more prevalent in women, 14 and the majority of studies have been performed in women and were restricted to certain age groups. In addition, some follow-up studies evaluating stroke risk in migraineurs have included individuals with non-migraine headache in the control group.11,15 To the best of our knowledge, the risk of stroke in TTH has not been evaluated previously despite the fact that several large studies have been conducted.5,11,15 Furthermore, the incidence of new-onset stroke in migraine needs to be estimated in a large-scale population-based study. This large population-based 15-year follow-up study aimed to investigate whether migraine, subtypes of migraine and TTH were associated with an increased risk of stroke. We also evaluated whether the association vary by sex or age group.
Materials and methods
Study design
This large-scale prospective population-based study used baseline data from the third Trøndelag Health Study (HUNT3) performed between October 2006 and June 2008. 16 The HUNT3 data were linked to the Norwegian National Stroke Register that have collected stroke data at a national level since January 2013 on an individual level, and our study is based on the confirmed stroke cases until December 2021.
Participants
Included in HUNT3 survey were all residents aged ≥20 years in Nord-Trøndelag. A more detailed description of the HUNT survey is found elsewhere. 17 The Norwegian National Stroke Register included all patients over the age of 18 years admitted to Norwegian hospitals with a stroke diagnosis. However, in the present study, only individuals aged ≥20 years in HUNT3 were considered for the occurrence of stroke.
Participants in the present study included individuals answering headache questionnaire during HUNT3 with risk of stroke until 2021. Excluded from the study were HUNT3 participants with no response to headache questions, and individuals with previous history of stroke and or myocardial infarction.
All inhabitants of the Nord-Trøndelag County aged ≥20 years were invited to complete extensive questions concerning health-related problems in two sets of questionnaires (Q1 and Q2). The first questionnaire (Q1) was enclosed with the invitation letter for clinical examination. The second questionnaire (Q2) was handed after the clinical examination and was instructed to complete it at home and return by mail. The Q2 included a total of 14 questions that were designed to evaluate whether the person suffered from headache and fulfilled the International Classification of Headache Disorders, third edition (ICHD 3) criteria for migraine or TTH. 18 Participants invited for brief medical examination included measurements of height, weight, and blood pressure. The stroke diagnosis was extracted from the Norwegian National Stroke Register for the period between 2013 and 2021. A linkage between the HUNT data and Norwegian National Stroke Register on an individual level was performed by using Norwegian personal identification number.
Headache diagnoses
The headache diagnoses were based on a self-administered headache questionnaire, and individuals who answered “yes” to the question “Have you suffered from headache during the last 12 months?” should answered 13 additional questions. Individuals who answered “no” were included in the “No headache” control group. The classification of headache types was based on the ICHD 3, 18 except for migraine diagnosis accepting attack duration less than 4 h because not specifically asking for untreated headache attacks in Q2. 19 Headache suffers were classified as migraine, tension-type headache (TTH), and unclassified headache. The diagnoses were mutually exclusive. The questionnaire-based diagnosis of migraine included those with attack duration < 72 h, at least two out of the four characteristics; pulsating quality, unilateral location, moderate to severe intensity, and headache aggravated by physical activity. In addition, during headache, at least one of the two characteristics; nausea or vomiting during headache, and/or hypersensitivity to light or noise. Participants with migraine reporting visual disturbance before migraine attacks were classified as MA, the remaining as MO. In opposite, the diagnosis of TTH included those reporting at least two of the following characteristics; bilateral location, pressing pain quality, mild to moderate intensity, and headache not aggravated by physical activity. Excluded from the diagnosis of TTH were those who reported nausea or vomiting or photophobia and phonophobia. Unclassified headache included mainly those with probable migraine or probable TTH.
The headache classification used in HUNT3 has previously been validated against interviews performed by neurologists. 19 For any headache, sensitivity was 88% and specificity 86% (kappa statistic was 0.70); for migraine, sensitivity was 51% and specificity 95% (kappa statistic was 0.50), 19 and for migraine with aura (MA), sensitivity was 50% and specificity 95% (kappa statistic was 0.44). In individuals with headache ≥1 day per month, the figures changed to 58% and 91% (kappa statistic of 0.54) for migraine, and to 96% and 69% (kappa statistic of 0.44) for TTH. 19
Stroke diagnoses
The Norwegian National Stroke Register was started in 2012 as a pilot project including 13 hospitals, and from 1st of January 2013, the register was established as a national quality register and included all hospitals in Norway. 20 All patients over the age of 18 years admitted to Norwegian hospitals with a stroke diagnosis (ICD10 code I61, I63, I64) are included in the stroke registry. Patients hospitalized with acute stroke after a traumatic head injury, stroke related to intracranial tumors, and ischemic stroke following a subarachnoid hemorrhage were excluded from the Stroke Register. The validation study showed that the Norwegian Stroke Registry was highly correct (positive predictive value 98.6% and specificity 100%) and almost complete (sensitivity 88.1%). 20
Confounders
Identification of the potential confounding variables in the present study was based on previous knowledge of possible risk factors for primary headache disorders and stroke. The variables considered to be potential confounders and available in our data set were age, sex, body mass index (BMI), smoking status, physical activity, alcohol consumption, cholesterol, high blood pressure, and Hospital Anxiety and Depression scale (HADS) score.19,21 Use of over the counter (OTC) medications or blood pressure medications were also evaluated. BMI was categorized as <25 kg/m2, 25–29.9 kg/m2 or ≥30 kg/m2. Blood pressure measurement and total cholesterol level were investigated as a continuous variable. Smoking status in HUNT3 was categorized as never smoked, former smoker, daily smoker, or smoking occasionally. The category “former smoker” was corrected for answers reported in HUNT1 and HUNT2. Occasional smoker was defined as those who smokes occasionally during the parties/vacation but not daily. Likewise, alcohol consumption was categorized as abstaining (no alcohol during last year or never drank alcohol), light drinking (<1 time per week), moderate drinkers (1–3 times per week) and heavy drinkers (4–7 times per week). Physical activity during leisure time was categorized as no physical exercise, ≤ 1 times per week, 2–3 times per week and almost every day.
Data analysis
Descriptive statistics for categorical variables are presented as numbers and percentages, and for continuous variables as means ± standard deviations (SD). Cox's proportional hazards regression model was used to estimate the hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between headache disorders and stroke. Time was defined as year from baseline period June 2008 to diagnosis of stroke until December 2021. We censored participants without stroke until the end of follow-up (December 2021). The HR of stroke was evaluated by headache subtype (migraine, MA, MO, TTH, and unclassified headache), comparing those who were headache free as the reference category. The cox-proportional hazard regression model assumption was assessed by the global test based on Schoenfeld residuals in adjusted models. No statistically significant violation was found. The analysis was initially adjusted for age (continuous variable) and sex, and subsequently for other potential confounders including smoking status and BMI. Other covariates such as high blood pressure (continuous variable), physical activity, alcohol consumption, cholesterol, HADS score, OTC medications or blood pressure medications were also evaluated. In supplementary analyses, evaluating the impact of age, we used median age of 55 years as cutoff. A previous study reported a difference in migraine stroke association by presence or absence of migraine features, particularly nausea/vomiting. 22 Thus, we performed supplementary sensitivity analyses, to evaluate the impact of accompanying symptoms, we sub classified migraineurs by absence of absence of nausea/vomiting, but presence of photophobia and phonophobia. The statistical software used for analysis was STATA 17.0 (StataCorp LP, College Station Texas, USA).
Ethics
HUNT3 was approved by the Norwegian Data Inspectorate, the Norwegian Health Authority, and the Regional Committee for Ethics in Medical Research. The Regional Committee for Ethics in Medical and the Nord-Trøndelag Health Research has approved the present study (ID 478096). All participants provided written informed consent prior to inclusion. The principles outlined in the Declaration of Helsinki were followed.
Results
In the HUNT3 study, 50,806 (54%) out of 93,860 invited individuals answered Q1, whereof 39,696 (42%) answered headache questionnaire in Q2 (Figure 1). Excluded from the present study were 11,110 HUNT3 participants without response to the headache questions, and 2332 persons with headache response who self-reported stroke or myocardial infarction at baseline in HUNT3 (Figure 1). Thus, a total of 37,364 with headache status with the risk of stroke were included in the analysis (Figure 1). Based on the Norwegian National Stroke Register, a total of 1095 (2.9%) developed stroke after a median of 9 years, 945 (86%) were ischemic, 141 (13%) hemorrhagic and 9 (1%) were unspecific.

Flowchart of the study participants in HUNT3 and confirmed stroke cases during follow-up period until 2021.
The demographic and clinical characteristics for 37,364 included individuals according to headache status are presented in Table 1. Over two third of participants reporting migraine and TTH were women and were younger than 55 years. Mean BMI and total cholesterol were identical in all headache groups. Participants reporting MA had a higher proportion of daily smokers (24%) compared to headache free individuals (15%). Compared to individuals who did not answer the headache questionnaire (n = 11,110), individuals who responded to the headache questions (n = 39,696) were somewhat older and less likely to smoke (Supplementary Table 1).
Characteristics of participants in HUNT3 at risk of stroke until 2021.

TTH = Tension type headache; MA = migraine with aura; MO = Migraine without aura; BMI = body mass index; HADS = Hospital Anxiety and Depression Scale; ¶Cholesterol measured in mmol/L, *Alcohol abstainers during last year.
Headache status and risk of stroke
Migraine
MA was associated with a higher risk of stroke (HR 1.54, 95% CI 1.15–2.06) in model 1 adjusted for age and sex (Table 2). The corresponding HRs in model 2 and model 3 with additional adjustment for potential confounders were respectively 1.55 (95% CI 1.16–2.08) and 1.59 (95% CI 1.14–2.21). In contrast MO was not associated with increased risk of stroke (HR 0.90, 95% CI 0.59–1.38). Interestingly, in sensitivity analyses identifying migraine by presence of photophobia or phonophobia but without nausea/vomiting, MA had significantly increased risk of stroke (HR 2.26, 95% CI 1.49–3.41) (Table 3), and the risk was especially high among women with aura (HR 2.57, 95% CI 1.58–4.16) and those aged less than 55 years (HR 2.42, 95% CI 1.19–4.91) (Supplementary Table 2). Additional analyses by stroke type showed significant association for ischemic stroke with MA (HR 1.65, 95% CI 1.21–2.24), but no association for hemorrhagic stroke (HR 0.96, 95% CI 0.35–2.64) (Supplementary Table 3 & 4). Further analysis on hemorrhagic versus ischemic stroke showed no significant association by headache types (Supplementary Table 5).
Hazard ratio (HR) of stroke with 95% confidence interval (CI) in relationship with headache type in HUNT3.
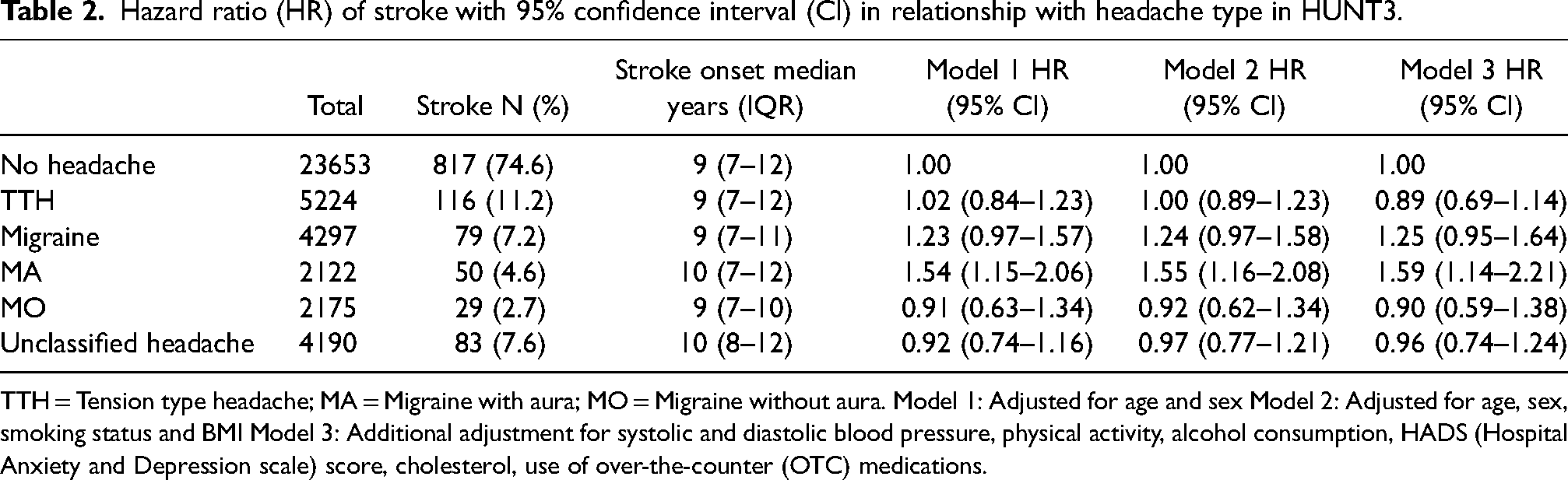
TTH = Tension type headache; MA = Migraine with aura; MO = Migraine without aura. Model 1: Adjusted for age and sex Model 2: Adjusted for age, sex, smoking status and BMI Model 3: Additional adjustment for systolic and diastolic blood pressure, physical activity, alcohol consumption, HADS (Hospital Anxiety and Depression scale) score, cholesterol, use of over-the-counter (OTC) medications.
Hazard ratio (HR) of stroke with 95% confidence interval (CI) in relationship with headache type in HUNT3. Migraine classified by presence of photophobia/phonophobia but without nausea/vomiting.

TTH = Tension type headache; MA = Migraine with aura; MO = Migraine without aura. Model 1: Adjusted for age and sex Model 2: Adjusted for age, sex, smoking status and BMI Model 3: Additional adjustment for systolic and diastolic blood pressure, physical activity, alcohol consumption, HADS (Hospital Anxiety and Depression scale) score, cholesterol, use of over-the-counter (OTC) medications.
Among individuals aged <55 years, MA was associated with increased risk of stroke (HR 2.18, 95% CI 1.24–3.82) compared to headache-free participants (Table 4). Conversely, among individuals ≥55 years, no association between MA and risk of stroke was found. Furthermore, in the sub-group analysis by sex, only women with MA were at higher risk for stroke (HR 1.70, 95% CI 1.12–2.59), whereas no significant association was identified in women with MO (Table 4). The risk of stroke among women with MA was highest among those aged less than 55 years (HR 3.14, 95% CI 1.48–6.65) (Supplementary Table 6).
Hazard ratio (HR) of stroke with 95% confidence interval (CI) in relationship with type of headache in HUNT3 separated by age and sex.

TTH = Tension type headache; MA = Migraine with aura; MO = Migraine without aura. Model 1: Adjusted for age and sex Model 2: Adjusted for age, sex, smoking status and BMI Model 3: Additional adjustment for systolic and diastolic blood pressure, physical activity, alcohol consumption, HADS (Hospital Anxiety and Depression scale) score, cholesterol, use of over-the-counter (OTC) medications.
TTH and unclassified headache
TTH and unclassified headache were not associated with increased risk of stroke, neither for ischemic nor for hemorrhagic stroke or in the sub-group analysis by sex or age. Overall, the HRs were respectively 0.89 (95% CI 0.69–1.14) and 0.96 (95% CI 0.74–1.24) (Table 2).
Discussion
In this large-scale population-based 13-year follow-up study, MA had 59% increased risk for stroke, most evident in individuals aged <55 years and among women. Individuals aged <55 years with MA had greater than two-fold higher risk of stroke compared to headache-free participants. No increased risk of stroke was found for MO and TTH.
Migraine and stroke
In contrast to previous studies,5,8–10 no significant association was found between total migraine (combined MA and MO) and risk of stroke. Three longitudinal cohort studies in respectively South Korea, Denmark and Taiwan reported increased risk of ischemic stroke among migraineurs with HRs ranging from 1.18 to 2.26.5,8,10 Likewise, a case-control study in the US also showed a significant association between migraine and stroke (HR 1.54, 95% CI 1.16–2.05). 9 In the sub-group analysis by aura status, studies from Korea and Denmark showed an increased risk of stroke for individuals both with (HRs 1.44 to 2.49) and without aura (HRs 1.15 to 1.81),5,10 whereas the other two studies reported increased risk only for MA (HRs 1.64 to 2.78).8,9 The differences in the results could partly be explained by methodological differences because several studies are prone to selection bias. Most of the available studies identified migraine disorders from the medical registers or insurance claims.5,8,10 The South Korean study selected participants with migraine diagnosis who were treated at least twice during the study period. 10 Using such strategy, individuals with migraine with frequent attacks may be overrepresented and milder migraine underrepresent. 10 Some studies have acknowledged the unknown validity for migraine diagnosis, and that results are prone to Berkson's bias.5,8 In contrast, the present study used a self-administered headache questionnaire to diagnose types of headaches in the entire population. Furthermore, several outcomes were measured in the Danish and the US study, including myocardial infarction, stroke, peripheral artery disease, claudication, venous thromboembolism, heart failure and AF,5,9 and the outcome that occurred first decided the diagnosis. In contrast, stroke was the only outcome measured in the present study. Stroke diagnosis in the present study was identified from the validated Norwegian National Stroke Registry, whereas the US study used self-reported data for cardiovascular events and later confirmed by medical records. 9 Likewise, in a Taiwanese study, stroke diagnosis was based on hospitalization claim. 10 The headache diagnoses in the present study were questionnaire-based, without optimal sensitivity of the migraine diagnosis, which probably at least partly may explain the lack of significant association between total migraine and stroke. Individuals with infrequent mild symptoms may have been included in the “no headache” control group which might lead to underestimation of the association between migraine and stroke.
Migraine with aura and stroke
Previous studies,5,8–10 including two meta-analyses6,7 have consistently shown greater risk of stroke in individuals with MA compared to those without aura. The US study reported a significant association between migraine with visual aura and ischemic stroke (HR 1.7, 95% CI 1.2–2.4) but not in individuals without visual aura (HR 1.2, 95% CI 0.8–1.7). 23 The migraine diagnosis in this study was based on headache questionnaire administered in late midlife, the authors have acknowledged the possible recall bias. 23 Data from the Women's Health Studies that included women aged ≥45 years observed increased risk of unspecified stroke and ischemic stroke only among women with MA (HRs ranging from 1.53 to 2.08).15,22,24,25 One of this study observed the strongest association between MA and ischemic stroke among individuals with a low risk of vascular events as measured by Framingham risk score. 25 The result in the present study is in accordance with most of the studies and demonstrates that only subtype MA is associated with an increased risk of stroke. In our supplementary analysis, individuals with MA defined by presence of photophobia or phonophobia but without nausea/vomiting had even greater risk of stroke. Similarly, the risk of stroke was more pronounced in the absence (HR 3.27, 95% CI 1.93–5.51) of nausea/vomiting than in presence (HR 0.91, 95% CI 0.43–1.93) in the Women's Health Study. 22 The differences in the inclusion criteria, definition of variables, discrepancy in lifestyles, as well as genetic background should be considered when interpreting the study. Unlike the present study, Women's Health Studies in the US were conducted among health professionals aged >45 years, thus young women with migraine were underrepresented. Consistent with our findings, a recent meta-analysis including all these studies suggested significant association only between MA and ischemic stroke. 7 The HRs for ischemic stroke in people with MA was 1.67 (95% CI 1.26–2.22) and for those without aura was 1.18 (95% CI 0.94–1.49). 7
Stroke by sex and age
Few studies reported migraine and stroke relationship by age and sex. In our subgroup analysis stratified by age and sex, only individuals with MA aged <55 years and women were at greater risk of developing stroke. The risk of stroke among women with MA was highest among those aged less than 55 years. Consistent to our findings, available evidence indicates a strong association in young people and in women.5,7,8,10 The Nurse's Health Study that included US female nurses aged 25–42 years showed 1.6-fold increased risk of stroke in people with migraine disease. 26 The Women's Health Study also agrees that the risk of ischemic stroke is twice as high in young women (<55 years) with MA compared to non-migraineurs. 15 A study in Denmark, Taiwan and South Korea that included both men and women reported greater than 2-fold increased risk of ischemic stroke among women with migraine,5,8,10 and the greatest risk was observed in women aged less than 45 years, particularly among those with aura.5,8,10 A recent meta-analysis including 18 cohort studies demonstrated that only women with migraine had a significant association with stroke (HR 1.32, 95% CI, 1.10–1.59) but not men (HR 1.53, 95% CI 0.74–3.17). 7 Since migraine is more prevalent in women with estimated women-to-men ratio of 3–4:1, 14 the association is uncertain for men. Although insignificant, we observed men with MA had 55% increased risk of stroke compared to those without headache. Thus, we performed additional analysis for men by age, the risk in men aged <55 years increased to 64% but the results were still not statistically significant (HR 1.64, 95% CI 0.70–3.86). Consistent with our data, no significant association was found among individuals aged >55 years. 8 One of the reasons could be that the occurrence of MA decreases in older age, and the effect of MA as a risk factor for stroke decreases with age. 27 Our study including previous evidence support a difference in migraine-stroke link by age and sex, highest risk among women below 55 years old with MA, suggesting a mechanism dependent to sex and age. Since migraine prevalence is high among childbearing age, thus affects during pregnancy and among oral contraceptive users. We do not have data on oral contraceptive use to present in this study.
TTH and stroke
No increased risk of stroke was observed for TTH. This is likely due to the absence of the complex vascular and neurological changes in TTH that are prominent in migraine. 28 In particular MA is linked with vascular risk factors such as smoking and hormonal changes, which are known to increase the risk of stroke. 29
Underlying mechanism
The exact mechanism underlying the association between migraine and stroke is still not clear and is likely to be multifactorial. Several cardiovascular risk factors, such as smoking, BMI, hypertension, diabetes, and hyperlipidemia have been linked with migraine.30–32 Our results after adjustment for most of the traditional risk factors demonstrated a significant association between MA and stroke, particularly in young women with MA. Several studies including meta-analysis have shown that the risk was even higher in women with MA who use oral contraceptives and are smokers.6,33–36 This indicates an interaction between hormonal changes and MA that increase the risk of stroke in young women. Furthermore, it has been suggested that coagulation abnormalities and endothelial dysfunction play a significant role in the pathogenesis of ischemic stroke.10,37 Patients with MA had a higher prevalence of hypercoagulation including endothelial dysfunction and are susceptible to thrombosis.38,39 Interestingly, a previous HUNT-based study has reported more pronounced elevated Framingham risk score in MA compared to other headache types. 40 Furthermore, cortical spreading depression (CSD), a self-propagating wave of depolarization across cerebral cortex has been associated with MA which plays a significant role in the pathophysiology of ischemic stroke. 41 Additionally, the shared genetic factors may also explain the association between migraine and stroke.42,43 Furthermore, several studies have suggested the relationship between stroke and patent foramen ovale (PFO), and migraineurs particularly MA are at higher risk of PFO.44,45 Moreover, several studies have suggested increased risk of stroke for those with higher migraine frequency and active migraine status,22,36,46 but no data is available on whether migraine prophylaxis drugs such as anti-thrombotic or statin therapy reduces the risk of stroke. 7
Strengths and limitations
Our study has several strengths, including population-based study with follow-up for 15 years, large number of participants with a broad age range, available stroke data on all participants, and use of validated headache questionnaires. Headache status including migraine sub-types were classified based on ICHD3 criteria. Stroke diagnosis was identified from the quality Norwegian National Stroke Registry, reducing the risk of misclassification compared to self-reported data. Excluding stroke events, the first four years reduces the possibility for reverse causation. 47 Our study is the first study evaluating the relationship between stroke and headache types including TTH. Furthermore, we evaluated stroke risk by aura status, following a separate analysis by age and sex groups. However, several limitations should be considered when interpreting the results. First, generalization of the results to the entire population must be done with caution because only 40% of the invited population answered headache questions and were included in the present study. Nevertheless, small differences for demographic characteristics were observed among individuals who answered headache questions compared to those who did not, and the risk of stroke was similar in both groups. Furthermore, the HUNT3 non-participant study showed no large difference in headache between HUNT3-participants and non-participants (42.1% vs 44.7% in women and 27.8% vs. 27.3% in men), and the migraine prevalence was also similar (10.9% vs. 11.8% in women and 5.0% vs 5.3% in men). 48 Second, self-administered headache questionnaire with moderate sensitivity for the diagnosis of migraine and migraine with aura was used, and the misclassification cannot be ruled out. It is important to note the possibility of misclassification of participants with migraine status due to low sensitivity would likely dilute a migraine stroke association. Further, migraine manifestation vary by age, 49 and the ongoing treatments might improve the migraine symptoms which is not considered in the present study and may dilute the magnitude of migraine. It is known that some aura characteristics are difficult to differentiate from symptoms of transient ischemic attack, and the latter is a risk factor for stroke. 50 Although with some symptomatic overlap, we believe that this would be a rare situation knowing that the average age of migraine onset and vascular events differ. Furthermore, the prevalence of MA (5.7%) and incidence of stroke (2.9%) is similar to those seen in other large population-based studies in Denmark.51,52 In addition, only individuals reporting visual aura were categorized in the MA group because information about sensory symptoms had very low sensitivity. Thus, the results for MA in the present study should be evaluated with caution. Third, the present study included only confirmed stroke cases registered in the hospitals. We cannot rule out the possibility that some individuals may have had mild stroke without seeking for medical attention. This could have underestimated the stroke incidence. Fourth, we do not have stroke data for the first 4 years of follow-up (2008- 2012) because the National Stroke Registry has data only from 2013. Thus, it is difficult to predict whether the inclusion of stroke diagnoses during the first four years would have changed our results, and in which direction. The present study also lacks data on recurrence of stroke during follow-up and endpoint. Fifth, analysis was adjusted for several important confounding factors, but we were unable to evaluate some of the recognized risk factors which may confound or mediate the association between headache disorders and stroke, such as use of hormonal contraceptives, use of medications including triptans, and NSAIDs (non-steroidal anti-inflammatory drugs).53–55 However, migraine specific drugs are used by both with and without aura, it seems an unlikely explanation to our results.
Conclusions
In conclusion, in this large-scale population-based follow-up study we found that MA was associated with increased risk for stroke, in particular among young women with MA. Further studies are required to investigate the complex migraine pathophysiology and to better understand the nature of the association of migraine with stroke, particularly for MA. Our investigation further warrants an evaluation on whether changes in migraine patterns and prevention of migraine may lead to beneficial effects on stroke risk.
Clinical implications
Individuals suffering from migraine with aura are at increased risk of developing stroke, independent of traditional risk factors. Clinicians should consider further investigations and prevention in young women with migraine with aura which had the greatest the risk of stroke. No evidence was found for stroke risk among individuals with migraine without aura or tension-type headache.
Supplemental Material
sj-docx-1-rep-10.1177_25158163241295735 - Supplemental material for Headache disorders and risk of stroke: A register-linked HUNT study
Supplemental material, sj-docx-1-rep-10.1177_25158163241295735 for Headache disorders and risk of stroke: A register-linked HUNT study by Samita Giri, Erling Tronvik, Håvard Dalen, Hanne Ellekjær, Alexander Olsen, and Knut Hagen in Cephalalgia Reports
Footnotes
Abbreviations
Acknowledgements
The Trøndelag Health Study (HUNT) is a collaboration between HUNT Research Centre (Faculty of Medicine and Health Sciences, The Norwegian University of Science and Technology NTNU), Trøndelag County Council, Central Norway Regional Health Authority, and the Norwegian Institute of Public Health.
Author's contribution
SG, ET, HD & KH: Study concept and design. SG & KH: Data analysis and interpretation of data. SG: Drafted the manuscript. ET, HD, HE, AO and KH: Interpretation of data and critical review of the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
Part of the dataset supporting the conclusions of this study is available on request to the corresponding author. Some of the data are the property of HUNT research center and can only be accessed through direct contact with the research center.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
HUNT3 was approved by the Norwegian Data Inspectorate, the Norwegian Health Authority, and the Regional Committee for Ethics in Medical research. The Regional Committee for Ethics in Medical and the Nord-Trøndelag Health Research has approved the present study (ID 478096) on May 16, 2022. All participants provided written informed consent prior to inclusion. The principles outlined in the Declaration of Helsinki were followed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.