
Abstract
Purpose:
In cluster headache, patients often describe a ramp up period with initially milder headache and then build up to a persistent and severe pattern. It is possible that within the early ramp up, patients may be more treatment responsive. We propose to study if response to therapy for prevention of cluster headache is dependent on timing from onset of cluster cycle.
Methods:
We will conduct a prospective observational cohort study, where we examine the relationship between timing of start of preventive medication and likelihood of response to treatment. We will look at individuals exposed within 10 days of onset of cluster cycle, versus those exposed after 10 days, to preventive medication.
Results:
We plan to enroll patients into the study and present data on completion.
Conclusion:
We aim to study the relationship between cluster headache onset and response to therapy. We propose that there is some data to suggest that earlier in cycle cluster headache may be more easily prevented, and we aim to study this relationship systematically. This is an important question that can influence treatment decisions in clinical practice, as well as clinical trial design.
Introduction
In cluster headache there are many factors that may influence treatment response including age, cigarette smoking, associated headache features (nausea or restlessness), and headache subtype (episodic or chronic).
1
–5
We propose another predictive feature in episodic cluster headache: time from the beginning of the headache bout. In episodic cluster headache there are headache bouts as well as remission periods lasting at least 3 consecutive months every 15 months.
6
In a scoping review of all preventive studies done in cluster headache by one of us,
7
we came across multiple trials in cluster headache where episodic cluster headache patients treated earlier in a bout were more likely to respond to preventive therapy. When patients were treated with melatonin
The possible mechanism behind the timing is unclear but it should be noted that there are two well-known shifts in attacks for episodic cluster headache patients. First, outside of a bout a patient’s headache triggers, such as alcohol and nitroglycerin, have no effect. Second, inside of a bout patients often describe a ramp up phenomenon, where the headaches become more frequent over time and in some cases become longer and more intense. 12,13 These shifts imply changes in neural sensitivity, and it is possible that treatment is more effective before the neurons have changed their sensitivity.
We hypothesize that earlier initiation of preventive treatment in a cluster headache cycle may lead to quicker onset of treatment response (Figure 1). We aim to study this in an observational prospective cohort pilot study where the treatment effect is compared in participants who are exposed to preventive medication in the first week of a cluster headache cycle versus those who are exposed later. If indeed treatment effect is greatest in the first week of a cluster cycle, commencement treatment, paradigms for these patients would have to be adjusted to reflect this fact and future clinical study designs may need to be adjusted. We have utilized recommendations for cluster headache trial design in creating this protocol. 14
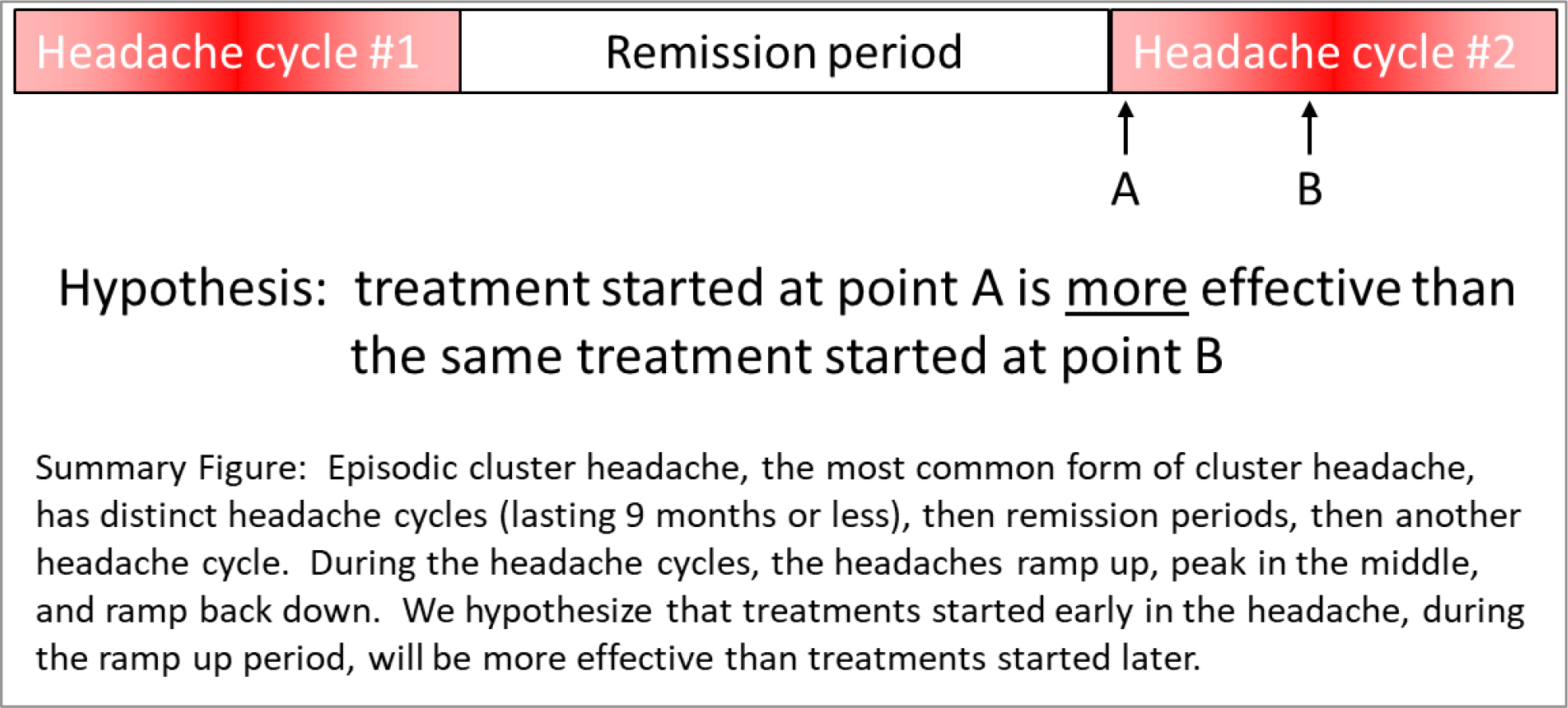
Hypothesis. If early prevention is more effective, this straightforward intervention could improve the success of both clinical care and clinical trials. Below we describe our protocol for this observational study.
Methods
Study cohorts
Inclusion criteria: 1. At least 18 years of age. 2. A diagnosis of episodic cluster headache by a neurologist or headache specialist either at a clinic visit or via phone interview according to the International Classification of Headache Disorders (ICHD)-3. 3. Based on duration of previous cycle, the current headache cycle will last at least another 3 weeks.
Exclusion criteria: 1. A history of untreated or undertreated severe psychiatric disease as determined by the study team. 2. Active pregnancy. 3. Participants who are not likely to be able to fill out the online questionnaire.
Study description
This will be an observational prospective longitudinal cohort pilot study with a retrospective baseline. The exposure of interest will be medication in the first 10 days of a cluster cycle versus later. We will follow participants prospectively with a questionnaire. Exposure is considered “early” if preventive medications in the list of included medications are given in the first 10 days of cycle onset, as “late” if given after day 10 of cluster cycle onset. The outcomes assessed will be timeline of cessation of attacks preventively, timeline to achieving a significant acute response, and weekly headache count (Figure 2). We have submitted this trial for approval at both our institutions, and it has been approved by our ethics committee. There is currently no funding for this study.

PICO question for our study. Considerations for our study. We present our study population, interventions and comparisons for our cohorts and the outcomes we will study.
There will be no randomization in this study, as this is an observational design. To counter the lack of randomization we will do propensity score matching. We will include variables thought to be effect modifiers in cluster headache: age, nausea, restlessness, and smoking. 15
Participants will be longitudinally followed for the duration of the present cluster cycle with a daily online diary. Participants will be blinded to the timing portion of this study: specifically, they will not know that investigators are looking for variability in treatment response relative to when in the cluster cycle a participant is treated with prevention.
The preventive therapies will be started as part of routine clinical practice, but to be allowed in our study have to will be one be four commonly recommended cluster headache medications, either given alone or concurrently: 16 –18 verapamil, steroids by mouth or occipital nerve injection, melatonin, and galcanezumab. 5 We will allow into the study and further consider in secondary sensitivity analysis other medications that are commonly used: lithium, topiramate, zonisamide, gabapentin, pregabalin, indomethacin, erenumab, fremanezumab, and eptinezumab. We will only allow these medications in the study if in sensitivity analyses the addition of these medications does not change the outcome of the study.
Outcomes will be measured with a daily diary. We define a cluster bout as having started when having a 7/10 intensity headache, and no longer than 48 hours without headache if not on preventive therapy. The baseline headache period will be retrospective, including 5 prior days of headache frequency as reported during screening interview. As this is an observational design, we will not withhold treatments, and a pseudo-baseline of the first week of treatment may obscure an early medication effect (in the first week in the study) in group 1. We will ask participants to record daily headache count and duration to tabulate 50% responder rate in weeks 1, 2 and 3 of treatment while in study compared to baseline, and weekly headache count. We will also ask participants: if their acute treatments are effective (defined as decreased from severe or moderate to mild or no pain within 30 minutes) and if they used their backup medication. The analysis of preventive treatments will be done in all headache participants, and we will only use those whose headaches are >45 min for the analysis of acute therapies. 15
Planned analysis
Primary outcomes
We will measure 50% responder rate (defined as decrease in number of headaches of at least 50% between baseline and week 2) between group 1 (those who started therapy
We will also measure the difference in number of weekly headaches over the first 2 weeks of treatment between group 1 (those who started therapy
Secondary outcomes
We will measure the percentage of attacks aborted within 30 minutes of acute therapy use over the first 2 weeks of treatment between group 1 (those who started therapy
We will also measure the rate of use of back up acute therapy over the first 2 weeks of treatment between group 1 (those who started therapy
There will be sensitivity analysis done including into the analyses proposed above, including those participants starting medications commonly used but without RCT evidence. If sufficient data is available, this analysis will be done by individual therapy.
Sample size calculation
We utilized the formula provided for test of proportions, as this is our proposed primary analysis. 19 We consider a power of 90%, alpha two tailed of 0.05, and we are assuming 50% responder rates when treated within 10 days of cluster cycle onset of 80%, 11 but later treatment in cluster cycle this value was only 45%. We estimated we would need 35 patients per group, for a total sample size of 70. As mentioned previously, we will not use participants on non-approved medications/treatments in the primary analyses. We estimate these would make up only 20% of the entire group, and so our total sample size would be 84. Additionally, we will increase the sample size estimate 20% when doing propensity score matching, and this would increase our sample size to 102. The calculations were done with an online calculator. 20 We estimate that we can achieve this sample size at 2 years and will plan to enroll for that duration of time.
Statistical calculations
For the primary outcome of 50% responder rate between baseline and weeks 1, 2 and 3 for those who started therapy within 10 days of cycle commencement or those who started later we plan to do a Chi-square test.
For the primary outcome of weekly headache count in those started on prevention at week 1 and those started after, we will do an exact Poisson test of two samples. This analysis has been suggested in previous RCTs in cluster headache. 21
For the secondary outcome of time to significant acute improvement in cluster headache, we will do a Cox proportional hazards model with use of therapy in week 1 versus later if the requisite assumptions hold. Otherwise, we will do a Chi-square test.
For the secondary outcome of rate of use of backup acute medication, we will do Chi-square test, those in week 1 of their cluster cycle versus those in week 3.
For the primary outcome of 50% responder rate we will also do a Chi-square test for non-approved versus approved medications as part of our sensitivity analysis.
We will report p values with confidence intervals where available, and odds ratios with confidence intervals where available. For our propensity score matching we will include variables thought to be effect modifiers in cluster headache: frequency and duration of attacks, duration of cluster disease, and smoking. 15
Study administration
Standard questionnaires to be filled out at entry into study and daily were designed, Data collection will occur in REDCap. Once the data collection has been completed, we will transfer the data into Excel sheets and R where the statistical analysis will be done.
We will obtain informed consent online from these participants when starting the questionnaire (subject information and informed consent form appended). We will allow for participant withdrawal/discontinuation on the questionnaire provided on RedCap.
Design limitations
This trial protocol is limited by the observational prospective cohort study pilot design, we are not recruiting patients to enroll and possibly withhold treatment and randomize, but rather observing clinical practice.
Clinical implications
We aim to study the relationship between cluster headache onset and response to therapy, and we propose that with treatment earlier in cycle, the cycle may be more easily prevented.
This is an important question that can influence treatment decisions in clinical practice, as well as clinical trial design.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.