
Abstract
Background:
Primary stabbing headache (PSH) is a rare primary headache presenting with short, stabbing pain sensations of unknown etiology. Owed to the rare prevalence of the disease, only limited data exists on possible treatment options. The most cumulative expertise exists for indomethacin as a potential treatment in PSH. However, known side effects and long-term tolerability issues have urged the FDA to restrict the use of indomethacin as long-term medication. In about 35% of the cases indomethacin does not provide sufficient relieve, demanding for efficacious and well tolerable alternatives.
Case:
Herewith we report a case of a young female adult presenting with PSH treated with melatonin resulting in an outstanding and long-lasting response. The patient has a rare underlying genetic disorder leading to facial dysmorphia, which according to the scarce literature, is not associated with PSH so far, but requires extensive exclusion of secondary causes of headaches.
Conclusion:
Given the exceptional tolerability of melatonin with low concern even on a long-term use, we discuss an indomethacin trial in PSH might be a diagnostic approach rather than a therapeutic one in the future.
Keywords
Introduction
Primary stabbing headache (PSH) 1 is described by the International Classification of Headache Disorders 2 as transient headache presenting with localized pain of short duration and irregular frequency. The irregular stabs reported in PSH occur in variable locations and sometimes are associated with dizziness, vomiting, photophobia or phonophobia (Table 1). The prevalence of PSH is higher in females (6:1) and estimated between 0.2% and 35% 3,4 in the general population. However, the higher prevalence could be due to referral bias. It is more likely the real number locks in somewhere around the 1% mark. PSH is an independent primary headache syndrome that can be distinguished from trigeminal autonomic cephalalgias (TACs) and migraine by the absence of accompanying trigeminal-autonomic symptoms and the duration and presentation of pain. Co-occurrence of PSH with other primary headache disorders like migraine is possible (40%). 3 Up to date, the underlying pathology of PSH has yet to be discovered. Pharmacological interventions used to successfully treat PSH may provide an insight in its genesis.
For the treatment of PSH the first line constitutes indomethacin with an estimated response rate of about 60%. 3 For all other agents, there is only scarce data from small observational studies and case reports. 5 From these, PSH patients not responding to indomethacin can undergo a trial of another non-steroidal anti-inflammatory drug (NSAID), Onabotulinumtoxin type A (BoNTA), gabapentin, topiramate, acetazolamide, nifedipine or melatonin.
The occurrence of primary headache syndromes in conditions with craniosynostosis is highly underreported in the literature. The Saethre-Chotzen syndrome (SCS) 6 is an autosomal dominant inherited condition characterized by craniosynostosis, predominantly of the coronal suture leading to a widely varying malformation. These malformations can include facial asymmetry, ptosis, strabismus, small ears with prominent crus, hypertelorism and broad nasal bridge. Further patients might also present with syndactyly between second and third fingers and duplicate first toe. Intellectual disability or delayed intellectual development have been reported. Lesser reported signs are short stature, hearing loss or heart defects. The condition has a prevalence of 1–9/100,000 living births and is caused by a point mutation in the TWIST1-gene (7p21) coding for a helix-loop-helix transcription factor in the differentiation of cell lines. The outcome usually is excellent if patients receive early corrective surgical treatment. Data on headache in SCS mainly focus on secondary headache attributed to intracranial pressure in patients with untreated or inconsistently treated craniosynosthosis. 7 No study so far described the manifestation of PSH/primary headache syndromes in SCS.
Case description
A 17-year-old female with a genetically confirmed (De-novo mutation in the TWIST1-gene) diagnosis of SCS first presented at the neurosurgical outpatient department with new headaches in the past 6 months. The patient underwent a fronto-orbital advancement (FOA) surgery at the age of 12 months due to craniosynostosis. FOA is a commonly used operative method to reshape and reposition the cranial bones of the forehead and orbits in infancy utilizing a bicoronal incision, allowing for unrestricted growth of intracranial structures. 8 Other disease features included hypertrichosis, syndactyly, myopia and astigmatism on both eyes, as well as a N. frontalis suspension due to congenital ptosis on the left eye. The patient exhibited no pronounced intellectual developmental disorder and school performance was unremarkable.
Due to the new headache, the patient was referred to the tertiary headache outpatient clinic for further attendance. The medical history revealed that the leading symptom were headache attacks that would follow no distinct distribution over the scalp, appearing randomly throughout the day. Attack duration was described as short (few seconds) and attacks could not be triggered by either coughing, exercise, cold stimuli, or Valsalva maneuver. Medication overuse was not reported at any time in the patient’s medical history. The pain was not dependent on the patient’s position. The headache characteristics were described as stabbing with a frequency of many a day to several an hour and an intensity of up to 7/10 at the NRS. No further concomitant symptoms, that is, no trigeminal-autonomic symptoms were reported. Besides these singular stabs a holocranial dull-pressing pain of low intensity was present irregularly with a high frequency (≥15 days/months) most of the days of the months. No other new deficits were reported. Paracetamol or NSAIDs were not beneficial.
Neurological examination was normal except for a known vertical ophthalmoparesis and ptosis on the left eye, hypertelorism, a strabismus sursoadductorius left and syndactyly on all extremities related to the underlying SCS-related dysmorphia. Palpation of the scalp and the patients’ sutures was normal, the pain could not be triggered by external stimulation. Supramaximal thermo- or electrostimulation was not performed in clinical routine.
From the typical characteristics, a primary stabbing headache was suspected. Secondary causes of stabbing headaches are rare but must be excluded before diagnosis. The most important are ischemic stroke, intracerebral hemorrhage, infectious disease, cerebral vein thrombosis, cerebral aneurysm, or other vascular pathology as well as neoplasms and autoimmune disease such as giant cell arteritis, multiple sclerosis, and lupus erythematosus. 3 Thus, we performed cerebral MR scans (T1, T2, T2*, TOF venography, DWI) that showed no pathological findings, particularly no signs of increased intracranial pressure, tumor, vascular pathologies. Extensive ophthalmologic examination revealed no sign of autoimmune disorder or vasculitis.
Laboratory findings showed no signs of acute or chronic infection and only mild anemia with hemoglobin of 115 g/L. An electroencephalography revealed increased frontotemporal theta activity on both hemispheres, but no epileptiform discharges.
With no current signs of secondary headaches, especially underlined by headache free intervals, we diagnosed the patient with probable primary stabbing headache according to the diagnostic criteria. An oral indomethacin trial was started with a sustained-release preparation of 75 mg once daily with concomitant proton pump inhibitor therapy. Furthermore, we prescribed biofeedback as well as cognitive behavioral therapy in line with a multimodal therapy concept. The diagnosis of probable PSH instead of certain PSH was made deliberately on our behalf, although the patient technically fulfilled the criteria according to the ICHD III. Rationale for this approach were the unusual long duration of the active episode of stabbing headaches.
At the 3-month follow-up the patient reported an almost immediate response to the indomethacin trial with reduced attack frequency from multiple stabs per hour to one or two stabs daily as well as decreased intensity (2/10 NRS). However, she experienced limiting side effects such as nausea, vertigo and fatigue leading to the discontinuation of indomethacin after 1 week. After the discontinuation the patient reported a rebound of symptoms with daily attacks with a frequency of one daily to up to several attacks per day, lasting less than 10 seconds. The distribution of the stabs still occurred randomly on the scalp and pain intensity was rated at 6–8 on the NRS. At this visit the patient reported troubles sleeping for the first time. The chronic dull-pressing headache that was reported on the first visit did not occur ever since, even before the indomethacin trial. Thus, a clear categorization could not be made and the additional diagnose “probable chronic tension-type headache” was discussed.
Since indomethacin was not tolerated and concomitant insomnia was reported a treatment with melatonin 5 mg (sustained release) daily, administered at night, was prescribed. We expected a positive effect on insomnia, but based on previous trials, possibly also on the PSH. Within the first 2 months of the therapy the patient reported a reduction in attack frequency from several attacks daily to attacks only every other day. However, after 2 months the patient experienced a slight recurrence with daily attacks, possibly in the sense of a wearing off effect. Melatonin did not affect the patients sleep, she continued to experience trouble sleeping with excessive daytime sleepiness. For further evaluation, an inpatient stay to undergo a polysomnographic testing was scheduled, where sleep-apnea could be excluded.
To maximize the therapeutic effect melatonin was increased to 10 mg (sustained release) daily. Hereafter the patient reported an almost 100% response with stabbing sensations only occurring every other month. Due to a missed prescription refill the patient reported to have had 1 week without melatonin therapy, with immediate rebound of attack frequency after 4 days but also swift therapeutic effect after reintroduction of melatonin therapy after few days. At the 1-year follow-up after increasing the dose, the patient remains almost pain-free with a single stab every other month. The treatment was well-tolerated without any side-effects without any wearing off effect. The treatment course and an overview of the patients’ follow-up is depicted in Figure 1.
Diagnostic criteria of primary stabbing headache.a
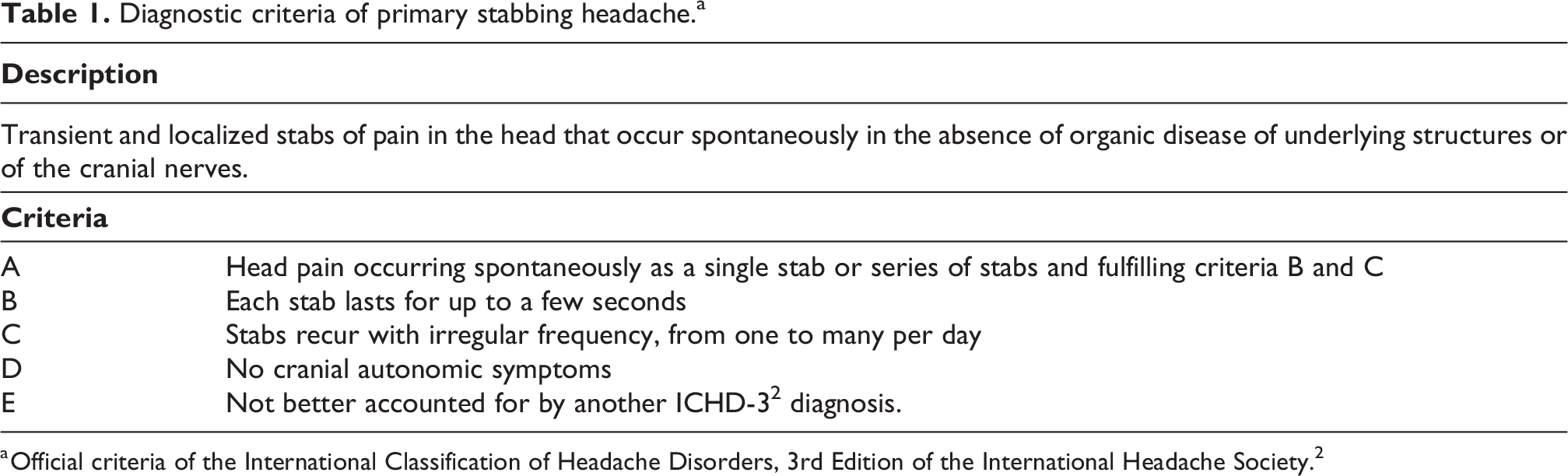
a Official criteria of the International Classification of Headache Disorders, 3rd Edition of the International Headache Society. 2
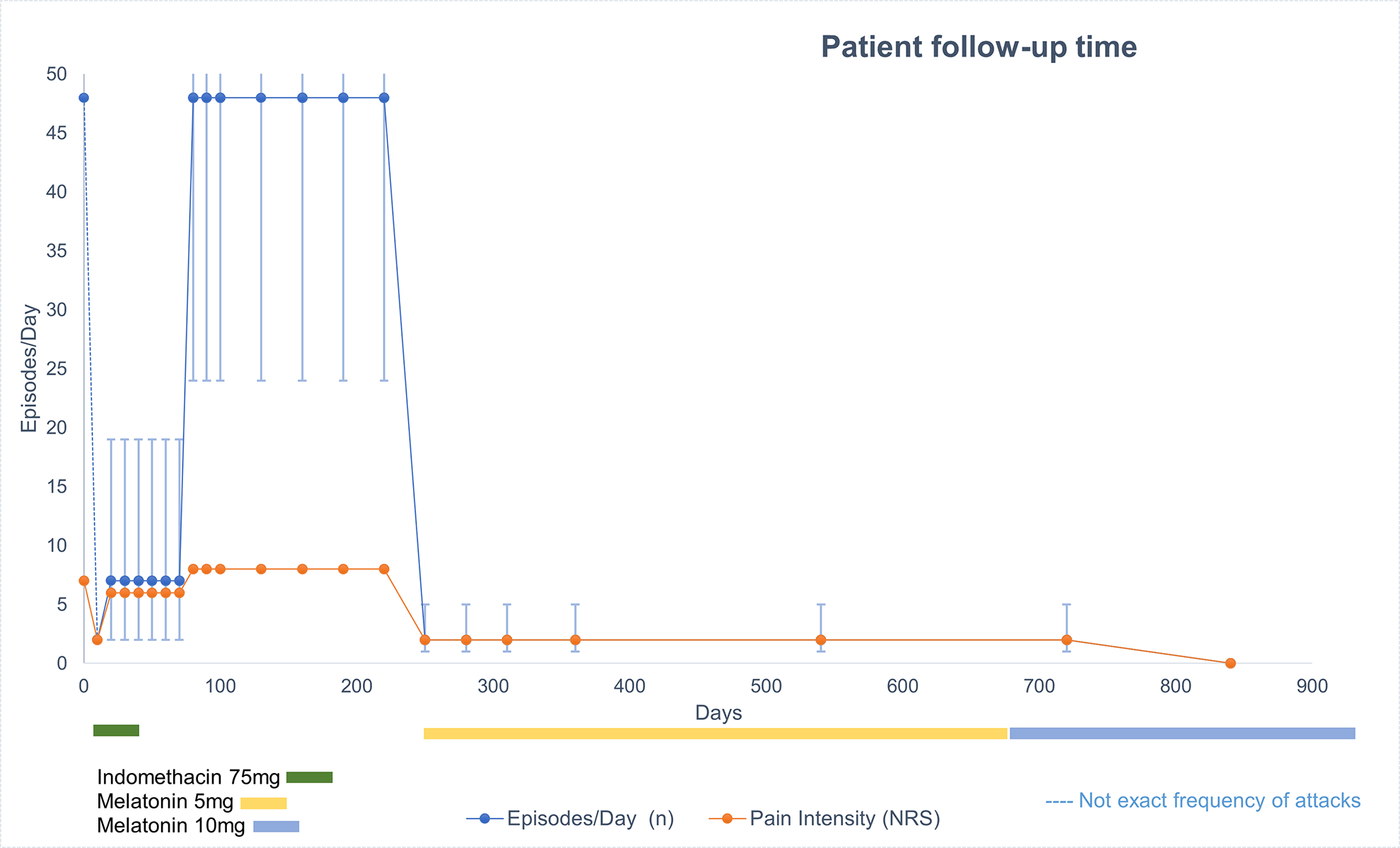
Graphical case description. The female adult patient initially received indomethacin 75 mg with in a sustained-release formulation to treat primary stabbing headache (PSH). Response regarding attack frequency as well as pain intensity was prompt, but due to lack of tolerability treatment had to be suspended after 7 days. A melatonin-trial with 5 mg per night was initiated which resulted in a promising initial response comparable to that of the indomethacin trial. However, in the following visits no complete cessation of the symptoms was achieved until melatonin dose was increased to 10 mg per night. No adverse effects to melatonin have been reported by the patient in the 1-year follow-up.
Informed consent/Ethical considerations
Written informed consent was obtained from the patient for the publication of this case report at the time she turned full age. Prior to execution, the case was presented to and approved by our independent ethics committee.
Discussion
Here we present a case of PSH treated with melatonin with outstanding therapeutic efficacy. Due to the low prevalence of PSH and subsequently limited awareness of the disease also among neurologists, only limited data exist on treatment options; randomized-controlled trials lacking entirely. The first line recommendation for pharmacological treatment constitutes indomethacin. Due to the unclear pathomechanism of PSH-development, it is also unknown which properties of indomethacin lead to the therapeutic effect. Besides the inhibition of cyclooxygenase, also an antagonism in nitric oxide pathways has been postulated. 5 However, a therapeutic failure with indomethacin can be expected in up to 40% of the cases, 1 demanding for alternatives. Due to the low adverse event rate and high tolerability as well as possible treatment of co-occurring insomnia, melatonin presents a suitable option. 9 This pineal hormone with anti-inflammatory, anxiolytic, antioxidant, and analgesic effects has been reported to be beneficial especially against pain itself in a number of primary headache disorders such as migraine, cluster headache, tension-type headache, hypnic headache and hemicrania continua. 10 For PSH limited data from case studies suggest a positive effect of melatonin, even in pediatric cases. 9,11 The mode of action is unclear, interestingly both indomethacin and melatonin share a common indole structure. Recommended starting dose of melatonin is 3 mg daily with possible titration of up to 24 mg. A noteworthy contraindication for the treatment with melatonin might be asthma, as increased nocturnal serum levels correlated with impaired FEV1. 12
Our patient additionally received a detailed work up to exclude secondary reasons for the headache, including but not limited to cranial MR imaging and exclusion of autoimmune disorders. The hereditary craniosynostosis in our patient was surgically treated at an early age and is therefore unlikely to be the reason for the new headache appearing 16 years later. Hereditary craniosynostosis usually is not associated with a higher incidence of headache according to the, admittedly scarce, literature. However, this applies only to patients that underwent corrective surgery with no further increased risk of intracranial hypertension. For example, Queiros et al. report on two cases of adults with Crouzon’s syndrome, a similar craniofacial dysmorphic syndrome. One female presenting with exorbitism, hypoplastic maxillary bone, obstructive sleep apnea, chronic headaches, and intracranial hypertension due to oxycephaly. The type or characteristics of the headaches were not reported. The headaches resolved after surgical correction of the dysmorphia by frontofacial monobloc advancement with internal distraction. The second case was a female patient suffering from intracranial hypertension, headaches, neck pain, exorbitism, and a hypoplastic maxillary. Furthermore, a Chiari malformation was discovered and surgically treated in advance. This patient has also received surgery, resulting in cessation of headaches. 13
In the management of patients with primary headaches, other important risk factors for headache chronification such as psychological factors or sleep disturbances must be addressed. In this case, both symptoms may have been present associated with the patient’s dysmorphia. As pointed out by Gelfand and Goadsby 10 for cluster headache and migraine, it would be interesting to examine the sleep–wake cycles of patients with PSH. In migraine and cluster headache, a dysregulated expression of circadian genes has been found, which, if present in PSH, may be an explanation for the marked treatment response to melatonin. It may also provide an insight in the mechanism of action of indomethacin in PSH due to the shared structural features. Thus, it could be beneficial to subject any patient with a potential melatonin responsive headache to a polysomnographic test or actigraphy, to further generate a better understanding of the disorder or to at least rule out secondary causes such as sleep apnea headache.
Conclusion and patient perspective
In conclusion, melatonin is an effective and safe option for patients with PSH with proven long-term efficacy. Melatonin could be used as a monotherapy or dose-saving agent for indomethacin. 14 The treatment is safe and well-tolerated, rendering it an important option to consider compared to other pharmacological agents used in PSH with more side effects (such as gabapentin or topiramate for example). Craniofacial dysmorphias require a more thorough exclusion of secondary causes, but apparently do not influence the therapeutic effect of melatonin or indomethacin. The underlying modes of action are yet to be discovered such as the pathomechanism of development of PSH. Randomized-controlled trials to further assess the effect of melatonin in PSH are necessary.
Upon interviewing the patient on her experience with the outcome of the treatment with melatonin so far, she reported ongoing subjective relief of limiting headaches. The stabbing sensations only occur rarely (once every other month) with a low intensity of 1/10 on the NRS. In hindsight, after reading up on her rare headache diagnosis, she told us to be very grateful to be diagnosed and treated so quickly. Compared to the first presentation in our tertiary headache outpatient clinic, as our patient was unable to attend school on a regular basis due to the headaches, she now finished studies and is able to work a demanding job full-time.
Clinical implications
This article highlights the efficacy and tolerability of melatonin in primary stabbing headache. As primary stabbing headache often requires long-term treatment, melatonin can considered as a dose-saving agent for indomethacin. Patients with craniofacial dysmorphias reporting headaches require a thorough exclusion of secondary causes of headaches, but can be treated as per suggested guidelines.
Footnotes
Acknowledgment
The authors extend our gratitude to our patient to be committed to our recurring follow-up!
Author contributions
FF was a treating physician of the patient and drafted the manuscript. VF has participated in drafting and reviewing the manuscript. KK has participated in reviewing the manuscript for intellectual content. GB was a treating physician and has participated in drafting the manuscript.
Declaration of conflicting interests
The authors declare the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FF has received travel grants from Novartis, TEVA, Lilly, and is a recipient of a grant from the Austrian academy of sciences (ÖAW). VF reports no conflict of interest. KK has received travel grants from Novartis, Lilly. GB has received unrestricted grants, honoraria, personal fees, travel grants from: Allergan, AMGEN, Menarini, Pfizer, Linde AG, Astra Zeneca, St Jude Medical, Reckitt Benkiser, Novartis, TEVA, Fresenius, Janssen Cilag, Lilly, Österreichische Gesellschaft für Neurologie (ÖGN), European Headache Federation (EHF), Österreichische Kopfschmerzgesellschaft (ÖKSG), Österreichische Akademie der Wissenschaften (ÖAW), European FP7 framework programme.
Ethical approval
This study was reviewed and approved by the local ethics committee of the Medical University of Innsbruck (EK Nr.: 1289/2022).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.