
Abstract
Introduction:
Detailed Emergency Department attendance data for migraine are needed for service redesign.
Methods:
A service evaluation was undertaken, classifying adult emergency department headache attendances using the International Classification of Headache Disorders migraine C-E criteria, evaluating attendance characteristics.
Results:
Migraine/Probable migraine diagnosis was documented in 58% but coded in 24% attendances by ED clinicians. 29% of patients used no analgesia before attending, 43% attended ≥4 days after onset and 19% arrived by ambulance.
Conclusion:
This evaluation highlights sub-optimal acute management and discrepancy between migraine coding and diagnosis contributing to underreporting. We recommend further evaluation of identified cohorts and headache proforma use.
Introduction
The United Kingdom (UK) headache guidance for local service commissioners recommends that most migraine is managed in primary care. 1 However, 23% of respondents to a national migraine survey reported visiting an emergency department (ED) for migraine in the prior 2 years. 2 This is in the context of continuing poor provision of community care reported by people living with migraine. 3 A recent audit using ED discharge data from patients attending for headache showed that 30% were diagnosed with migraine. 4 A better understanding of the characteristics of these emergency attendances for migraine is needed to direct further work on improving alternative access to headache care.
Methods
The service evaluation was a collaboration between the headache service and ED at St George’s Hospital, London– a large UK teaching hospital hosting a major trauma centre and regional neurosciences centre, serving around 1.2 million people. A retrospective cross-sectional analysis was performed of consecutive electronic attendance records of patients attending ED from 1 December 2016 to 30 April 2017. Inclusion criteria were all attendances coded on arrival as attending for headache. Attendances were excluded if clinical records were unavailable, further review of case notes indicated the primary reason for attendance was not headache, or the patient was under 16 years old.
Documented headache features were extracted directly from electronic case notes. Patients were classified for the purposes of the evaluation, if they met criteria C, D and E criteria of the International Classification of Headache Disorders (ICHD-3) criteria for migraine 5,6 independently of documented ED clinician diagnosis. Variables recorded for headache attendances were age, gender, timing, and arrival method. For those attendances meeting C-E criteria, documented diagnosis, discharge coding, treatment prior to and during attendance, as well as headache symptom duration prior to attendance were recorded. Descriptive statistical analysis was performed in Microsoft Excel.
Research ethical approval was not required according to the UK Health Regulatory Agency (HRA) decision tool. Local approval processes were followed for accessing data for service evaluation.
Results
During the 5-month review period, 63,159 patients attended the ED, of whom 889 (1.4%) attendances were coded at arrival as headache (Figure 1).
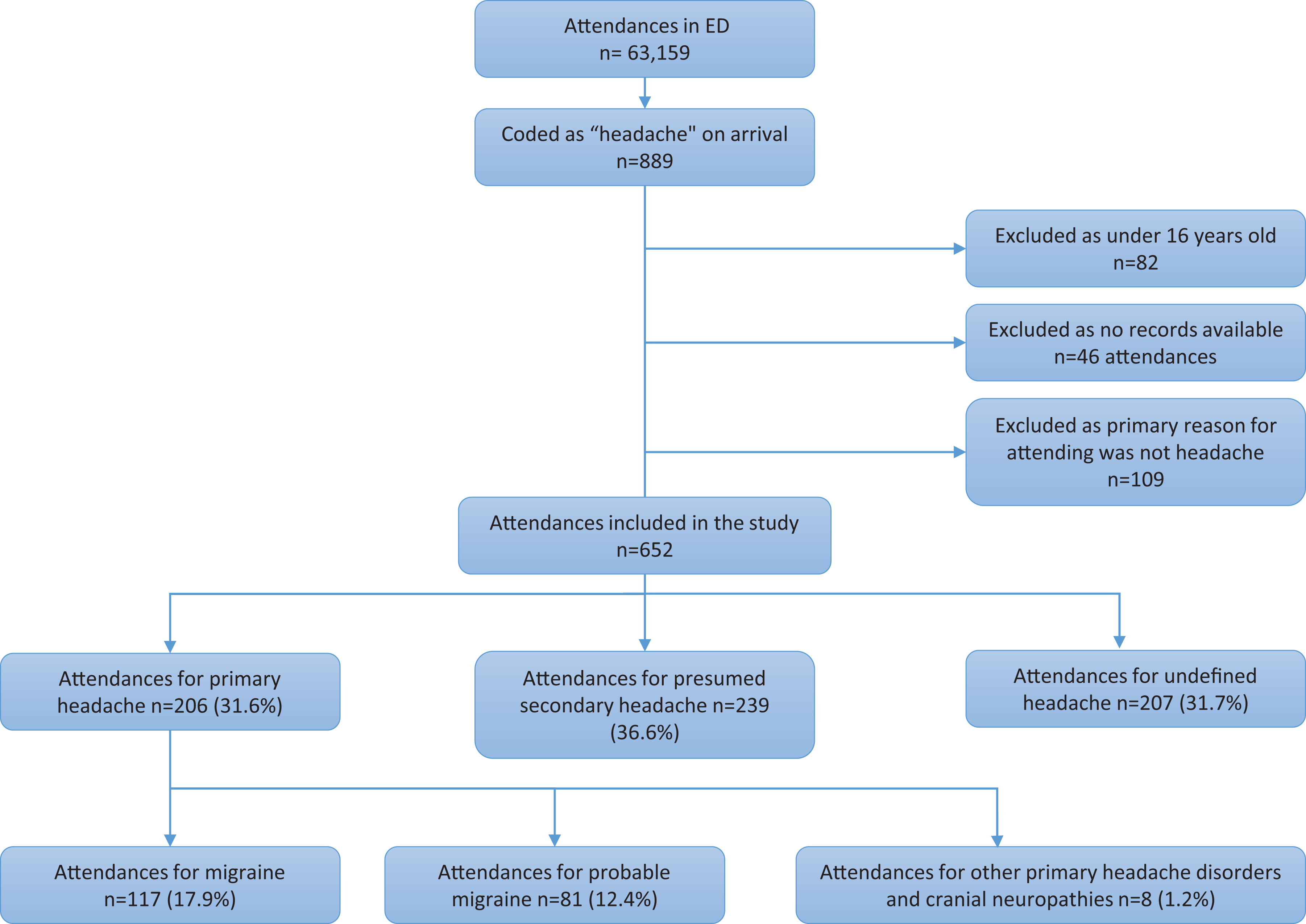
Flowchart of ED attendances during 5-month study period.
It was not possible to classify 207 (32%) of study attendances due to lack of documentation of headache features. Migraine/probable migraine as defined by meeting ICHD-3 criteria C-E was fulfilled in 198 (30%) attendances of the 652 included study attendances. Only 48 (24%) of these were given a migraine discharge coding by ED clinicians although a migraine diagnosis was written in the clinical documentation in 115 (58%) of attendances. Scans occurred in 59 (29.5%) attendances.
Of the 198 attendances fulfilling the migraine/ probable migraine ICHD-3 C-E criteria, 101 (51%) were given a generic discharge coding of headache by ED clinicians.
Descriptive statistics of the attendances are shown in Table 1.
Demographic, investigation and attendance characteristics.

Migraine/probable migraine attendances attendances
The majority of attendances, 137 (69%), had longer symptom duration than 24 hours at arrival, with 85 attendances (43%) occurring ≥4 days post-headache onset. This may reflect patients attending with preexisting chronic symptoms or status migrainosus.
Migraine/probable migraine treatment
No treatment was taken prior to 58 (29.3%) attendances. Triptan containing treatment was used prior to 20 (10.1%) attendances or during 3 (1.5%) attendances (Table 1).
Arrival method
Patients arrived by ambulance in 37 (18.6%) attendances, 13 (6.6%) of which had a migraine onset of ≥4 days. One of 37 attendances were referred by a health care professional.
Discussion
This service evaluation identified three important cohorts of patients with documented features fulfilling the ICHD-3 criteria C-E for migraine/probable migraine using the ED. It highlighted a discrepancy between attendances coded as migraine and those with clinical documentation of migraine diagnosis by ED clinicians, with likely underreporting.
The majority presenting to ED for migraine do not attend acutely, with 43% attending ≥4 days post-onset. These delayed attendances may highlight primary or specialist care access issues and warrant further investigation. Strikingly, a third of patients did not use analgesia prior to attendance despite recommendations to do so early 7 highlighting the need for patient and clinician education. Lastly, significant numbers of migraine patients accessed ED by ambulance but only one was referred by a health care provider. This may reflect the self-perceived urgency and severity of their needs. 8 Health economic evaluations have not included ambulance use, 9 increasing the known direct costs of migraine. Further study is needed into these cohorts.
A recent study has shown that one-third of patients attending ED for headache were coded as migraine. 4 However, in our evaluation we identified attendances with reported migraine features fulfilling the ICHD-3 criteria C-E for migraine/probable migraine through documented symptoms and in these compared ED clinician recorded diagnosis and coding data. The results showed that 34% of attendances were not coded as migraine by the ED clinicians despite having a documented migraine diagnosis in narrative records, with a preference instead for generic discharge coding as ‘headache’. Reasons for this are unclear but coding is known to underreport other conditions in ED, 10 and is limited by inconsistency. Retrospective notes reviews using documented features have been used previously 11 but are limited by inadequate documentation. While the ED documentation provided reliable medication use and symptom onset records, headache features were reported less consistently. This work has implications for the evaluation of the migraine attendances purely using ED coding data. We suggest that a standardised proforma-based approach would improve diagnosis and management in ED. Coding support for ED clinicians would improve data quality, assisting accurate evaluation of the extent of migraine presentation to acute services.
We limited the ICHD criteria to C-E on the basis of previous work 6,12 raising concerns over using the full ICHD A-E criteria in ED which limited diagnosis in one-third of patients with headache. Although not fulfilling the full diagnostic criteria it was a pragmatic approach for this ED study, enabling us to identify an important patient cohort for further study and raise awareness of these attendances.
Clinical implications
Priority groups were identified for further study; patients with non-acute presentation, those not using analgesia prior to attendance, patients arriving by emergency transport.
Greater focus on alternative support, education for migraine management and self-management advice in the community is needed.
A proforma-based approach to ED headache evaluation could assist junior medical colleagues expediting accurate diagnosis.
Coding support for ED clinicians will improve the accuracy of reporting of headache conditions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.