
Abstract
Background:
The aim of this work is to analyze reports of migraine attacks collected online in the citizen science project CLUE with respect to gender- and migraine type-specific differences in drug effectiveness and pain perception. Citizen science project data collection opens the possibility to examine these differences based on a large number of individual attacks instead of a simple survey of patients.
Methods:
One thousand three hundred and ninety four participants reported 47,274 migraine attacks via an online platform and smartphone apps. The reports contained information on the acute medications taken, the evaluation of their effect, and information on pain parameters such as pain intensity, origin, and localization. Chi-square tests were used to investigate whether the effect of acute medications and pain parameters differed when collated by gender and migraine type (migraine with and without aura).
Results:
Our participants rated the effectiveness of triptans as significantly better than that of ibuprofen. For triptans, significant differences in effectiveness were found when migraine types were distinguished, but no difference was found between genders. For ibuprofen, there were no differences between migraine types but significant differences between gender groups. Examination of pain parameters reveals differences between groups in pain intensity, pain origin, and pain location. The differences are statistically significant, but the effects are small.
Conclusions:
Despite some methodological limitations, web-based data collection is able to support findings from clinical trials in a real-world setting. Due to the high numbers of participants included and attacks reported, even small differences in medication efficacy and pain parameters between the groups considered can be demonstrated to be statistically significant.
Introduction
Collecting health data as part of citizen science projects using modern technologies such as smartphone or web apps makes it possible to conduct studies with a larger number of participants over a longer period of time and on a more transregional basis than is possible in the context of conventional medical studies. In research of headache disorders, for example, it is thus possible to record and evaluate a large number of headache attacks in a large number of participants. Data collection in a real-world scenario offers a number of advantages over data collection via questionnaires, as data can be collected immediately during or after the attacks. In addition, many clinical studies are limited to patients of headache clinics, which may lead to a bias toward severely affected headache patients.
Results from the citizen science project CLUE (CLUsterkopfschmerz Erforschen) are presented in this article. Migraine attacks are investigated with regard to differences in the assessment of drug effectiveness as well as differences in reported pain parameters in different participant groups. Distinction is made with regard to the migraine disease—migraine with aura (MA) and migraine without aura (MO)—and with regard to the gender of the participants.
Some studies report data on clinical characteristics of migraine attacks 1,2,3 in terms of pain intensity, accompanying symptoms, and duration of attacks between MA and MO, others on the effects of placebos in both groups, 4 and two focused on the effect of sumatriptan for attack treatment 5,6 and obtained conflicting results. Another study investigated the effect of different triptans in women and men. 7
However, there are only few studies that consider not only the intensity but also the origin, type and location of pain for both groups. With the help of the CLUE research project and the associated “Migraine Radar” app, numerous migraine attacks have been recorded, thus creating a suitable database for those evaluations. However, it must be considered that the recording of migraine attacks with the help of the citizen science approach has some limitations that will be discussed in detail in the context of this work.
Methods
The CLUE project
The CLUE project is a citizen science project to study cluster headaches and migraines. Smartphone and web apps have been used to collect data on headache attacks. Different apps were developed for the diseases and adapted to the signs and symptoms of the specific condition. The migraine attacks relevant for the study have been collected since 2015. 8 Participants could register and take part in the project at any time and then start reporting their migraine attacks. During the registration process, participants were informed about privacy issues and gave their consent to participate. All data are anonymized for analysis.
The study was approved by the Ethics Committee of the Medical Faculty of the University of Rostock (reference number A 2017-0091).
Study design
The aim of the prospective study was to investigate different pain parameters such as intensity, type, origin and location as well as the effect of the medication taken during the migraine attack. Analyses focused on identifying differences in and between two main groups of participants: the gender (male/female) and the migraine type (MA/MO) group.
Participants
Between January 1, 2015 and December 31, 2020, 84,501 migraine attacks were reported by 4,681 participants from Germany, Austria and Switzerland. A standard headache questionnaire using the diagnostic criteria of the International Classification of Headache Disorders (ICHD-3 beta) was used to diagnose migraine. 9,10 Additionally, participants were asked if they experienced typical aura symptoms related to their headache attacks. The translation of the wording in the query is: “At the onset of migraine attacks, often before the headache, an aura may occur. Aura symptoms are characterized by increasing and spreading over minutes and then typically lasting 20–60 minutes. Typical aura symptoms include an increasing flicker before the eyes or an increasing restriction of the visual field, a rising tingling sensation or numbness, for example, in the arm. Do you suffer from such symptoms occasionally or regularly in connection with your headaches?” The answer to this question was used to classify the participant’s diagnosis as a migraine with aura or a migraine without aura. The duration of a migraineur’s participation in the project was calculated by the difference between the first and last reported attack. Participants were included in our study if they met the criteria to participate for at least 30 days and to report not less than five migraine attacks. In addition, we also ensured that the attacks considered were actually migraine attacks. For this purpose, only those attacks that met at least one of the typical accompanying symptoms were considered. According to ICHD-3 beta, these are nausea, vomiting, sensitivity to light and noise. 10 For comparison of the effectiveness of individual drugs, only attacks in which exactly one single drug was taken were observed. Participants with chronic migraine were excluded. Participants who did not want to reveal the year of birth and therefore chose the current year were also excluded from the study.
Data collection
During the registration process, basic characteristics such as gender, year of birth, place of residence, occupational group (employed (full-time, part-time), not employed (pupil or student, retired, unemployed)) and information on shift work (shift work: yes or no) were collected. During the study, the participants entered information for each migraine attack on the onset and end of the attack, pain characteristics (pulsing/throbbing, dull, sharp and others), pain location and intensity (on a numerical pain scale between 0 and 10 according to Hawker et al. 11 ). The participants also provided information on accompanying symptoms (nausea, vomiting, sensitivity to light/sound/odor, need for rest or movement, dizziness, etc.), medications taken and an assessment of their effectiveness, other measures (resting and lying down, cooling down, caffeine intake, etc.) and absence from work and cancellation of planned activities.
The drugs taken were divided into eight classes (triptans, ibuprofen, acetylsalicylic acid (ASA), paracetamol, combination preparation, metamizole, tramadol or tilidine and peppermint oil). Also “others” could be selected. A differentiation of the individual drugs in the classes, for example in the case of triptans, did not take place. The effectiveness of acute medication was asked with the question “improvement due to medication” and participants could choose between “yes,” “no” and “little.”
Statistics
The data were analyzed using the R language and the R-studio environment. 12 Chi-square tests were used to compare the distribution of the participants to different groups like gender or the different migraine headaches (MA, MO). Welch’s t-test was used to compare the age distributions of the several groups. Chi-square tests were used to compare the effectiveness of drugs in different groups. The groups could represent different drugs (e.g. triptans, ibuprofen) or the gender of the participants (female or male). The effectiveness of the drugs was divided into two classes (“yes” and “little/no”) in accordance with Pearson et al. 13 The duration of participation and the number of reported attacks varied greatly among the participants. To ensure that individual participants with a large number of reported attacks do not dominate any result, the density distribution for each participant was included in the calculation of the Chi-square. The different number of attacks was then taken into account when calculating the statistical error of the components.
Results
Considering only those participants who met the requirements of at least 5 attacks within at least 30 participant days, 47,274 migraine attacks of 1,394 participants remain.
These data include 36,366 attacks in females (18,264 migraine attacks with aura (MA)/18,102 attacks without aura (MO)) and 10,908 attacks in males (5,697 MA/5,211 MO).
For the study of pain parameters, we excluded the typical aura without headache by considering only attacks with pain intensity greater than zero; 47,233 attacks fulfilled this requirement. All these attack reports include—beside the pain intensity—information about the pain type, origin and location.
At least one drug was reported in 41,173 attacks.
Table 1 summarizes the key figures of the participants. Table 2 divides the participants into migraine with aura and migraine without aura.
Participant characteristics.

SD: standard deviation.
* Except for age.
Division of participants into with aura and without aura.

SD: standard deviation.
* Except for age.
Effectiveness of acute medication
In the examinations of the medications taken, only those attacks are taken into account in which the participants reported taking exactly one acute medication for pain control. This means that the stated effect could only be attributed to the one medication. After this restriction, 27,171 attacks remained. The drugs the participants could choose from are shown in Figure 1. In addition, the figure contains information on the number of participants who used the respective drug. Since each participant can report attacks with different drugs, the total number of participants in Figure 1 is higher than the total number of participants shown above. Attacks are only included in the further analysis if a participant reported at least five attacks with the corresponding drug.
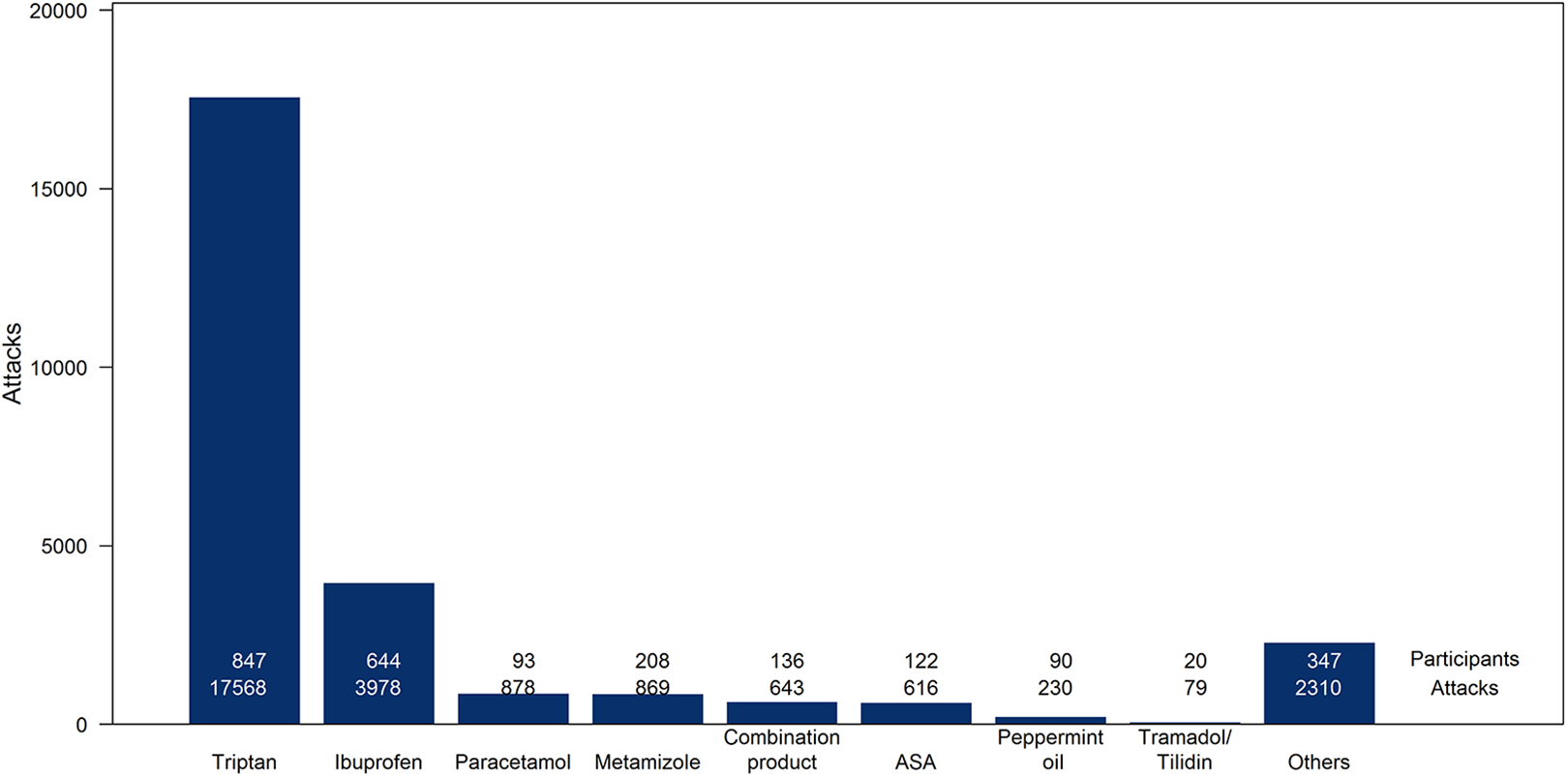
Distribution of the medications for attacks with only one medication reported.
In the following, the analysis was limited to attacks with triptans and ibuprofen because these two drugs are the most commonly used and because only for these two there is a sufficient number of reported attacks to analyze the data in the groups considered.
First, the assessment of the effectiveness of the two drug groups was examined. Figure 2 shows the assessment of the effectiveness of the drug triptan with its classification into “yes,” “little” and “no” in the different groups.

Assessment of the effectiveness of the drug triptan.
Table 3 shows the results of the analysis. As mentioned above, the effectiveness classes “little” and “no” were merged into one class for the evaluation of the effects.
Results of the assessment of the drug triptan in terms of effectiveness as an acute medication.

* p < 0.05, ** p < 0.01, *** p < 0.001
Looking at the effect of triptans and differentiating by migraine type, statistically significant differences can be found. In particular, it can be seen that MO migraineurs perceive a better effect than MA patients. However, when looking at the effect of triptans in relation to gender, there is no difference.
These studies were carried out in the same way for the drug ibuprofen. In this case, Figure 3 shows the effectiveness of the drug ibuprofen and Table 4 shows the results of the corresponding chi-square test.
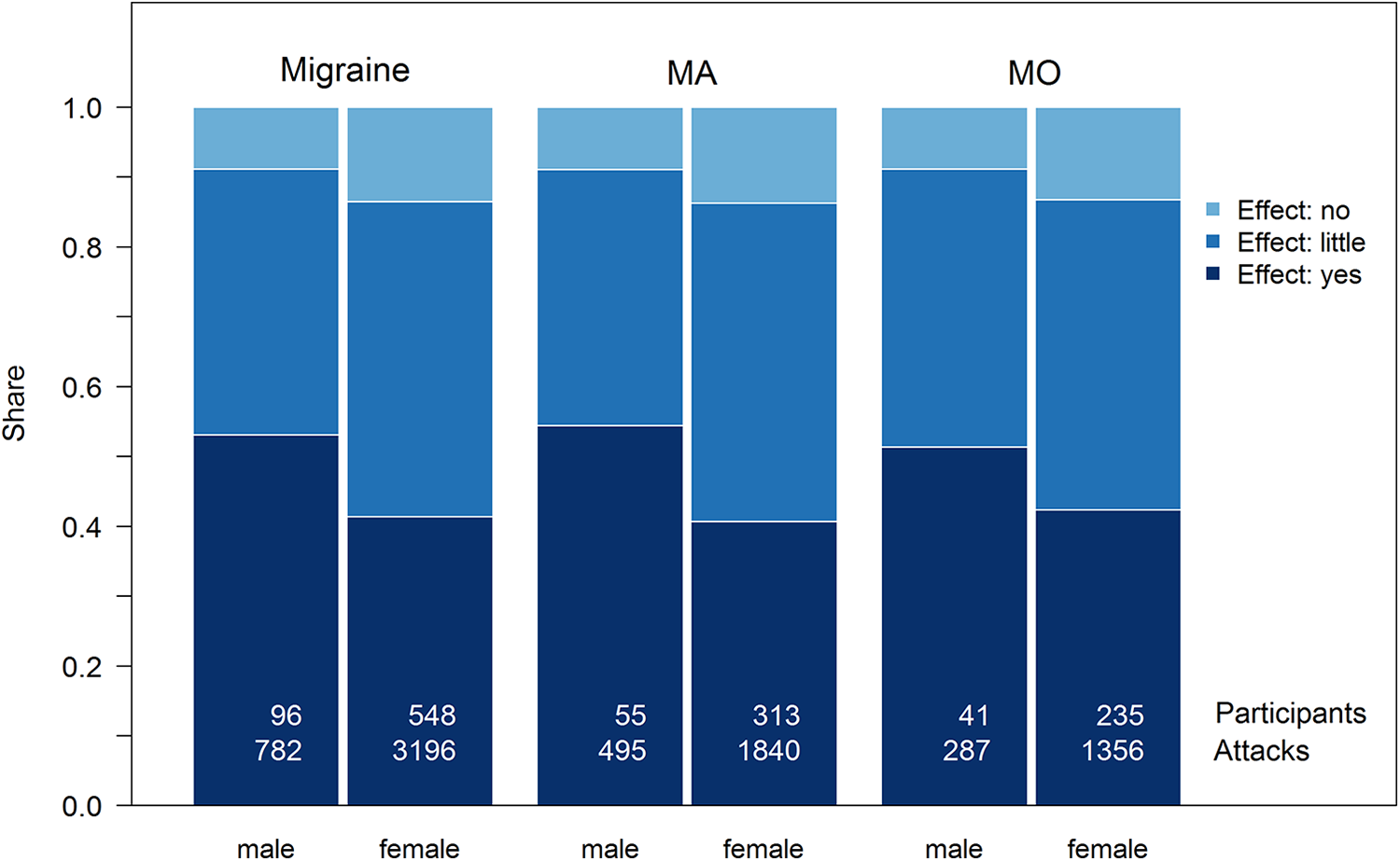
Assessment of the effectiveness of the drug ibuprofen.
Results of the assessment of the drug ibuprofen in terms of effectiveness as an acute medication.

* p < 0.05, ** p < 0.01, *** p < 0.001.
If a distinction is made between the groups of MA and MO migraineurs, no statistically significant differences in the effect of ibuprofen are found. However, there are gender-specific differences in the drug ibuprofen, especially in the group of MA migraineurs. Among this group, the effect is significantly better in men than in women.
Subsequently, the two drugs were compared to each other. As can already be seen from Figure 2 compared to Figure 3, participants rated the effect of triptan much better than the effect of ibuprofen, regardless of which group was considered. The corresponding p values and odds ratios are summarized in Table 5.
Comparison of the assessment of the effectiveness of triptans and ibuprofen using the latter as a reference when calculating the odds ratio.
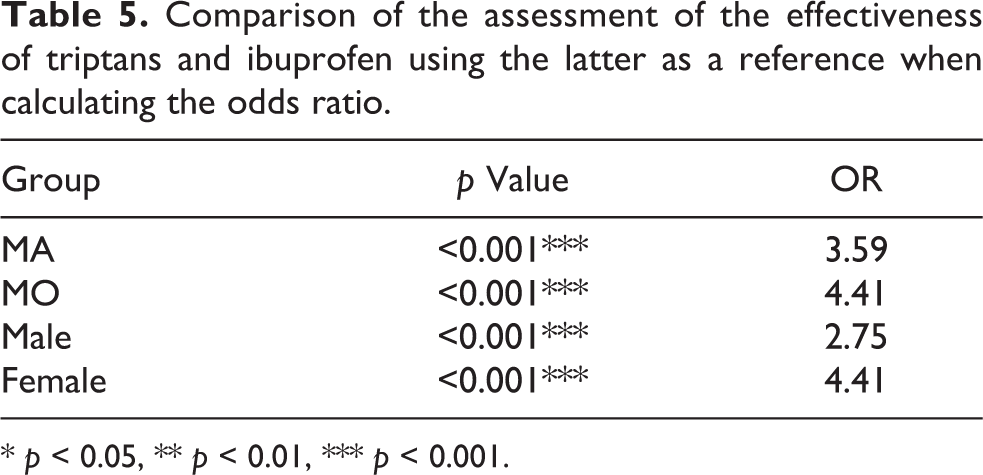
* p < 0.05, ** p < 0.01, *** p < 0.001.
Pain perception
First, the intensity of pain was examined. Attacks with an intensity of 0 were excluded because they can only occur in the MA group (attacks with an aura but without pain phase). The different values cover the different levels between freedom from pain and maximum pain. Figure 4 shows the distribution of the pain intensities in the groups of participants. Different levels of pain are illustrated in the same color to classify the intensities as mild (intensities 1 to 3), moderate (4 to 6), severe (7 and 8) and very severe (9 and 10).

Pain intensity of the attacks in the subgroups under investigation.
Slight differences can be observed between the groups. For example, migraine attacks with aura seem to lead to a trend to higher pain intensities. On average, migraine attacks are perceived as slightly more severe by women than by men. However, while most of the differences are statistically not significant, trends can be seen. The results are summarized in Table 6.
Results from the analysis of pain intensities.

SD: standard deviation.
* p < 0.05, ** p < 0.01, *** p < 0.001.
In addition, the indicated pain side was examined. The participants had three different possibilities—only left-sided, only right-sided and bilateral pain—to specify the pain location. Figure 5 shows the distribution of the specified pain locations in the selected groups.

Pain location in the subgroups under investigation.
Again, there were statistically significant differences in the groups considered. Table 7 shows the corresponding results. With regard to the migraine types, there is a difference in the distributions, which is due to a significant difference in women, whereas no significant difference is found in men related to pain side. Additionally, men suffer from bilateral pain more often than women.
Results of the analysis of the pain location (only right, only left, bilateral) reported by the participants.a

a The p values indicate the results for the comparison (chi-square tests) of the distribution in the groups considered (see also Figure 5).
* p < 0.05, ** p < 0.01, *** p < 0.001.
We additionally examined the origin of the migraine pain. The origin of the pain may be in the area of the head, eyes or neck. Figure 6 shows the distributions, Table 8 the results of the analysis.
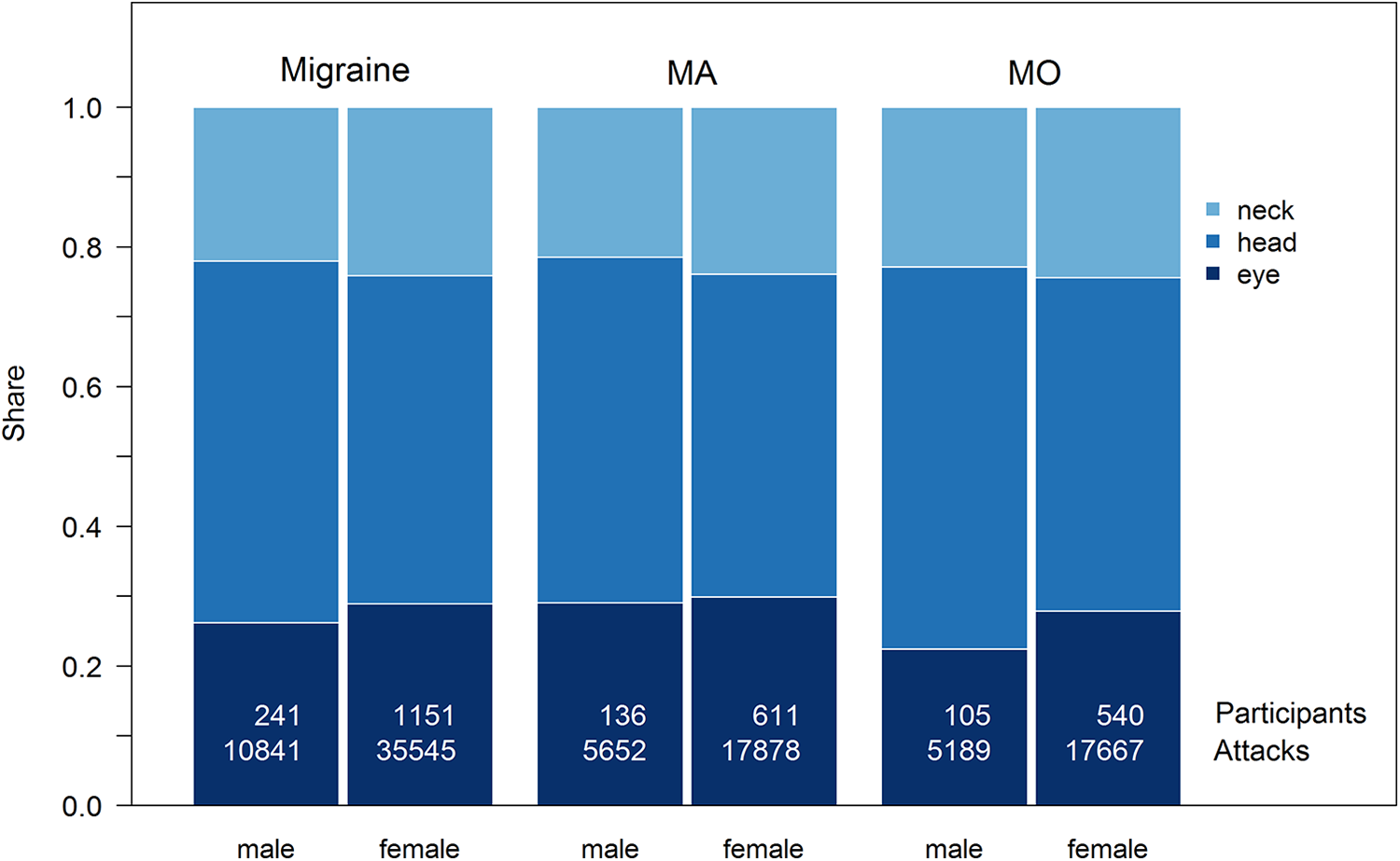
Pain origin in the subgroups under investigation.
Results of the analysis of the reported pain origins (neck, head, eye).a
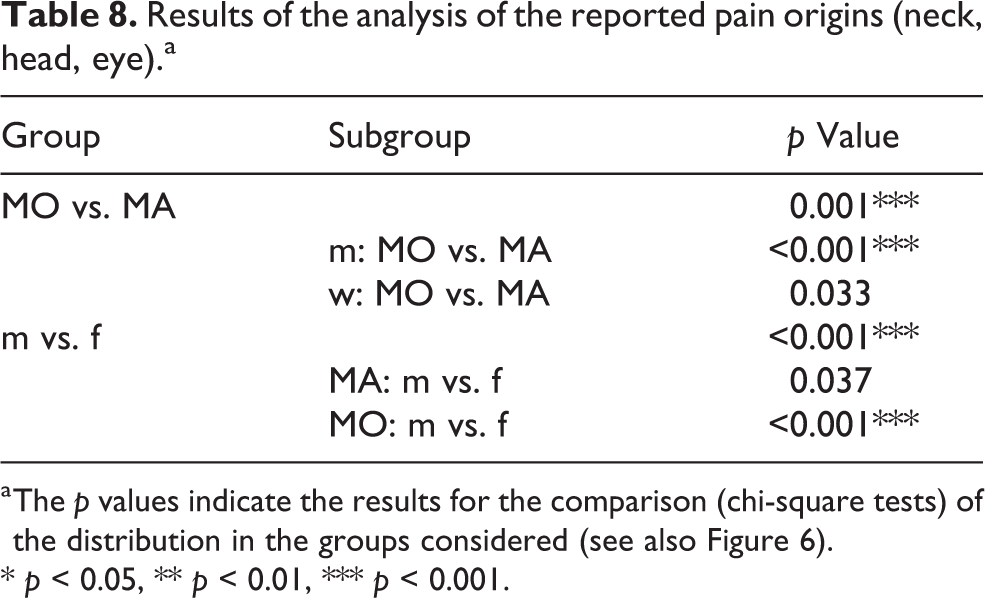
a The p values indicate the results for the comparison (chi-square tests) of the distribution in the groups considered (see also Figure 6).
* p < 0.05, ** p < 0.01, *** p < 0.001.
The figure shows that the onset of pain around the eye is less frequent in male MO migraineurs than in the other groups. This results in statistically significant differences in the comparison of the groups.
In addition, the type of pain was considered. Figure 7 shows the distributions in the investigated groups, Table 9 the results of the quantitative distinctions.

Pain type in the subgroups under investigation.
Results of the analysis of the reported pain types (pulsating, dull, stabbing).a

a The p values indicate the results for the comparison (chi-square tests) of the distribution in the groups considered (see also Figure 7).
* p < 0.05, ** p < 0.01, *** p < 0.001.
There is a significant difference in the proportions of pain types in the group of male MO migraineurs—especially between the pain types dull and pulsating.
Discussion
We analyzed 47,274 migraine attacks in 1,394 participants in terms of acute medication use and effectiveness. The focus of all the analyses was to detect differences between the genders and between the groups migraine with aura (MA) and migraine without aura (MO).
In terms of medications, we found that triptans and ibuprofen were by far the most commonly used acute medications among the participants in our sample.
Looking at the drugs individually and comparing the participants’ assessment of their effectiveness in the subgroups considered, there are no differences in the effectiveness of triptans between genders, which is in agreement with the study of Franconi et al. 7 where 1,978 attacks in 346 participants were analyzed. The effect of triptans in migraine without aura is estimated to be significantly better than the effect in migraine with aura. This is in accordance with the study of Hansen et al. 6
Ibuprofen is considered to be equally effective in migraine regardless of the presence of an aura, but there is a difference between the genders: the attacks reported by men suggest a better effect of ibuprofen compared to that reported by women. This is in agreement with the study of Walker and Carmody, 14 but there, the effect of ibuprofen was measured in electrically induced pain.
Comparing the effects of the drugs with each other, the effectiveness of triptans proved to be significantly better than that of ibuprofen in all groups considered.
It is noteworthy that although triptans are recommended for therapy of migraine attacks if they are severe and do not adequately respond to analgesics or NSAIDS, 15 a large proportion of attacks are treated with less effective drugs. This could be because as a study has shown, about half of those affected by headaches do not consult a doctor. 16 However, three non-prescription triptans are now on the market, which decouples the use of triptans from a doctor’s visit.
The following results were obtained for the pain parameters considered: Although the distribution of pain intensity of the reported attacks showed minor differences in the groups considered, the mean pain intensities were not statistically significantly different. This is consistent with Davies et al., 1 a questionnaire-based study in which 354 patients with MA and 397 patients with MO were included.
As far as the location of pain is concerned, significant differences were found between the groups. It is noticeable that women report bilateral pain much less frequently than men. In addition, MO seems to lead to bilateral pain less frequently than MA. The study by Rasmussen and Olesen 2 found evidence of this, but the difference was not statistically significant in their study, which was based on 38 MA and 58 MO patients.
Examination of the origin of pain shows differences between the genders, especially in the MO group. The groups also differ significantly in the type of pain. It is noticeable that quite a large proportion of participants report dull pain.
Some limitations of this work have to be discussed. The main weakness of this study is the way in which the data were collected. Participants could join or leave the study at any time. Even though a minimum participation period of 30 days was required, it cannot be guaranteed that participants actually reported all their attacks during this period. Selective reporting by the participants could also not be ruled out.
In addition, the diagnosis of migraine was not confirmed by a physician, but was merely based on a standard questionnaire. Although, as a precaution, only attacks with at least one of the typical accompanying symptoms were included, it cannot be ruled out that migraineurs who do not suffer from migraine at all also participated.
Another critical point is the fact that the presence of aura was only self-reported by the participants and not confirmed by a medical diagnosis. This can lead to individual participants mistaking perceptions for an aura that are not.
Of course, the results on the effectiveness of acute treatments are not absolute because participants take the medications they expect will help them. We do not have information on which acute treatments a participant had previously tried and may have found less helpful.
In addition, we examined the medications taken only in groups; for example, we did not distinguish between different types of triptans or between different dosage forms. Studies have shown that the dosage form can have a great impact on the effectiveness of triptans, see e.g. Eiland and Hunt 17 and Hou et al. 18
This publication addressed two questions: (1) Are there gender-specific differences in the use and effect of acute medication and pain parameters in migraine with and without aura? (2) Can valid results be achieved with web-based data collection, in which a large number of volunteers report their migraine attacks nationwide and over a long period of time?
The first question can be answered with yes. Various differences were found in the groups considered.
Regarding the second question, it can be said that the web-based collection of health data can be at least a good complement to classical health studies. Due to the large number of participants and attacks, many explorative studies are possible, but the weaknesses of the data collection must always be taken into account. Results that seem interesting should always be verified in conventional studies that do not have the weakness of web-based data collection.
Key findings
The effect of triptans in migraine without aura is estimated to be significantly better than the effect in migraine with aura.
The effectiveness of triptans proved to be significantly better than that of ibuprofen in all groups considered.
Web-based collection of health data can be at least a good complement to classical health studies.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Gaul has received honoraria for consulting and lectures within the past 3 years from Allergan Pharma, Lilly Germany, Novartis Pharma, Hormosan Pharma, Grünenthal, Sanofi-Aventis, Weber & Weber, Lundbeck, Perfood and TEVA. He does not hold any stocks of pharmaceutical companies. He is honorary secretary of the German Migraine and Headache Society. Dr Kropp has received honoraria for consulting and lectures within the past 3 years from Allergan Pharma, Lilly Germany, Novartis Pharma, and TEVA. All other authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Medical Faculty of the University of Rostock (reference number A 2017-0091). We confirm that all methods were performed in accordance with the relevant guidelines and regulations.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the German Federal Ministry of Education and Research (BMBF—Project 01BF1701).