
Abstract
Objective:
To define a new type of head pain syndrome termed “cranial suture headache” which is a localized headache originating along the cranial suture lines of the skull.
Background:
Well localized headaches maybe extracranial in origin. As trigeminal nociceptors are localized within the cranial sutures of the skull, these fibrous joints maybe the source of head pain for some patients.
Methods:
Case series. To diagnose cranial suture headache, the patient’s pain had to be localized to the skull and elicited/mimicked by mild to moderate palpation over one or more distinct cranial suture lines.
Results:
Ten cases are presented. Most of the patients were women (9/10). The headache started daily from onset in all cases. Range of age of headache onset was 32–64 years. Headache was one sided, unless confined to the midline and typically lacked any migrainous and/or cranial autonomic symptoms. Most cranial suture headaches localized to either the sagittal, coronal or squamosal suture lines. Headache duration prior to diagnosis was on average 8.5 years. Triggering events: three began immediately after head trauma, two had very remote head trauma, one was post infectious, one was post craniotomy, while three patients had no known triggering event. All patients were treatment refractory failing at least three preventive medications. All improved with localized anesthetic injection to the suture line(s) and/or onabotulinum toxin A injection only to the cranial sutures.
Discussion:
Without the recognition of cranial suture-based pain, patients may have unremitting headaches that can last years to decades. The observation that “cranial suture” headache improves with localized treatment only to the cranial sutures would seem to suggest the extracranial origin of the pain.
Keywords
Some headache patients do not fit into an ICHD defined subtype. 1 They have failed multiple classes of preventive medication, have no response to abortive agents and have intractable head pain. They can tell you where it hurts on their head, even point to where they feel is the region of pain origination, but the area of pain may not fall under the well circumscribed location of nummular headache. 1 The object of this manuscript is too define a new type of headache deemed “cranial suture headache” which as the name suggests is a localized headache originating along the cranial suture lines in the skull.
Methods: Case series
Reporting on a series of patients that were evaluated in an academic headache clinic over the last 3 years and deemed to have cranial suture headache. Patients were evaluated by a neurologist specializing in headache medicine. To diagnose cranial suture headache, the patient’s pain had to be localized to the skull and elicited/mimicked by mild to moderate palpation over one or more distinct cranial suture lines. The length of palpated pain had to extend beyond what would be expected for nummular headache, unless it involved a cranial suture line of short length (e.g., frontal suture). The exam would entail palpation of the primary cranial sutures (sagittal, coronal, squamosal, lambdoid), but smaller suture lines were also palpated based on patients perceived head pain location. The author utilized skull anatomy diagrams (Figure 1(A) to (D)) to help pinpoint the exact suture lines involved if smaller or connecting sutures seemed to be irritated (e.g. sphenofrontal, sphenoparietal, frontozygomatic). No distinct sensory examination of the scalp was completed. This is a descriptive study only.
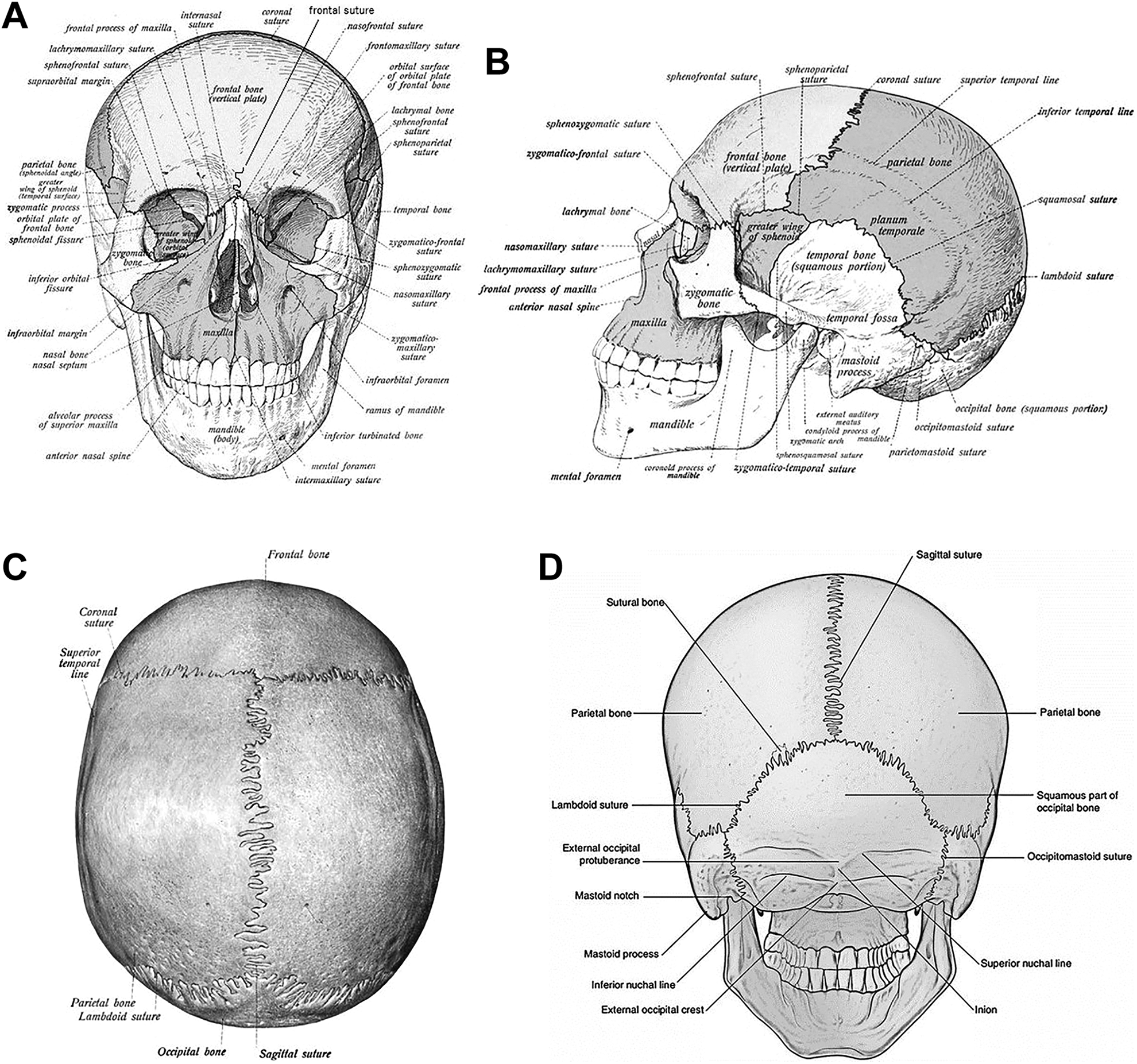
(A) Skull cranial suture lines frontal view. (B) Skull cranial suture lines lateral view. (C) Skull cranial suture lines vertex view. (D) Skull cranial suture lines posterior view. Skull cranial figures are free to use per author’s institution Mayo Clinic.
Results
There have been 10 cases of cranial suture headache diagnosed by the author (Table 1). All patients presented with a complaint of chronic daily headache. In all cases the pain started as a daily persistent headache from onset, thus meeting ICDH-3 criteria for new daily persistent headache (NDPH). 1 All patients could define the location of where their head pain was originating. Headache was typically one sided unless midline in respect to sagittal suture-based pain. Most lacked any migrainous symptoms (7/10) and none had cranial autonomic symptoms. Most of the patients were women (9/10). A history of migraine was noted in 4 of the 10 patients. Range of age of headache onset was 32–64 years, with a mean age of 42 years. Headache duration prior to diagnosis was on average 8.5 years of persistent pain (range 3 months to 21 years). On examination, the palpated pain typically ran the entire length of the suture line, but at least 75% of the suture length was involved in all patients. Two patients presented as nummular pain by description but when the calvarium was palpated, the area of perceived pain extended beyond the subjective circumscribed site to along a suture line. It appeared that the nummular location was at the connection point of two suture lines-coronal/sagittal in both cases.
Cranial suture headache: Patient demographics.

In regard to triggering events: three cases began immediately after head trauma (one of these was a physical abuse case where the patient’s hair was pulled from the scalp along the sagittal suture line), three had very remote indirect or direct head trauma (one hit her head 20 years prior, one banged her head 12 years prior, and another fell against a door 5 years prior but on the side contralateral to her headache and without direct head trauma), one was post infectious with heavy coughing/sneezing, one was post a craniotomy surgery, but her pain was not localized to the craniotomy site but in a remote location, while three patients had no known triggering events. All patients were deemed treatment refractory failing at least three headache preventive medications, although most failed five plus prophylactic medications. Most of the substances that were prescribed were for a diagnosis of migraine and thus included antidepressant and anti-epileptic/neuropathic medications. After consultation, imaging studies (MRI brain w/wo, MRA head, MRV head and skull x-ray) were completed, if they had not been done prior, and which presumably ruled out secondary causes of headache. All studies were normal. All patients failed indomethacin (dosing up to 75 mg tid) to rule out hemicrania continua. Patients over the age 50 years had a negative sedimentation rate and CRP to rule out giant cell arteritis, while one patient had a negative temporal artery biopsy prior to her headache consultation. See Table 1 for full patient demographics.
Four representative cases of “cranial suture headache” are presented (Table 1: Patients 1–4):
Patient 1
A 62-year-old woman with a very remote history of migraine presented with a 3-month history of right sided head pain, localized to the temporal region. She awoke one day with the headache and it had been present since and of a very severe intensity. She could not think of a triggering event for headache onset. She remembered a remote trauma to that side of her head 20 years prior, falling against a door but outside of several days of pain after the trauma she had no residual pain in that region. Currently, her head was so tender she could not touch it. She was seen by rheumatology for possible giant cell arteritis and even though her sedimentation rate was in the normal range a temporal artery biopsy was completed as her exam was suggestive of arteritis. The biopsy came back negative, so she was sent for Headache consultation. High dose prednisone did help with her pain but did not provide pain freedom and was thus tapered off after the negative biopsy results. Associated symptoms with the headache included some migrainous features (photophobia and phonophobia) but no cranial autonomic symptoms. On exam the patient had significant palpable tenderness over the right coronal, squamosal, sphenoparietal and sphenofrontal cranial suture lines. Mild palpation made her almost cry. Remainder of the examination was non focal. Neuroimaging for secondary causes was completed and were normal. An oral indomethacin trial up to 75 mg tid provided no benefit. On return visit, localized injections over the cranial suture lines with 1% lidocaine and triamcinolone 40 mg/ml provided 3 weeks of pain freedom. Serial anesthetic injections every 6 weeks continued to provide relief but never lasting longer than 3 weeks. Thus, onabotulinum toxin A therapy was initiated focusing injections over the irritated cranial suture lines. With each successive round of onabotulinum toxin A, her time of pain freedom lengthened, and she just returned for repeat treatment after having 1 year of complete headache freedom.
Patient 2
A 35-year-old woman presented with a 3-year history of pain around her left eye. The pain just started one day out of the blue without a precipitating event. The pain was continuous and of moderate to severe intensity. It would wax and wane in severity but never had any associated migrainous or cranial autonomic symptoms. On exam there was no tenderness over the supraorbital/supratrochlear notches and or the trochlear region. Eye movement did not exacerbate the pain. Neuroimaging was normal including looking at the intra and extracranial vessels. An oral indomethacin trial up to 75 mg tid failed. In office supraorbital and supratrochlear anesthetic injections with 1% lidocaine provided no benefit. Trochlear injections under ultrasound guidance also gave no pain relief. Various preventive medications including gabapentin and topiramate were ineffective. On seeing the patient back in follow-up, she made the remark that her area of discomfort was more to the lateral part of her eyebrow/orbital bone and not in the region we had been focusing on. Re-examination found a trigger zone which matched up to the fronto-zygomatic suture line. Anesthetic injection (2 cc of 1% lidocaine) along the suture line provided immediate benefit and her pain has not returned through a 1-year follow-up.
Patient 3
A 65-year-old woman presented with a 21-year history of daily persistent headache. She had experienced very infrequent migraine without aura since her teens, however the day after she had a retro-sigmoid craniectomy for removal of a left acoustic neuroma tumor she developed a new headache which was more right sided in location and which never dissipated. She sensed the pain was temporal in location, but the top of her head was very sensitive to the touch. The site of the craniotomy did not hurt. The pain was moderate to severe in intensity with no migrainous or cranial autonomic associated symptoms. She thought a divot had developed at the vertex, possibly where a skull fixation device was placed at the time of her surgery. She had failed 8 plus “migraine” preventives and also onabotulinum toxin A injections using the “migraine protocol”. Nothing improved her pain including opiates. On examination the patient’s headache could be mimicked by palpation over the sagittal cranial suture line, worse to the right of midline. Anesthetic injections with lidocaine and triamcinolone along the suture line provided short term benefit of several days to 1 week. Thus, onabotulinum toxin A injection therapy was retried but this time only focusing on the sagittal suture line which was not injected with previous treatments. After three rounds of treatment her suture-based headache was almost 100% improved with no more pain to palpation on examination. The thought was that skull movement during the surgery and or suture displacement by a skull fixation device caused the suture-based headache.
Patient 4
A 61-year-old woman presented with a 19-year history of daily persistent headache. Her headache began along with a flu-like illness with excessive coughing and sneezing. The pain was localized to the mid-forehead. Everyday pain was mild to moderate in intensity. For the first 17 years she had minimal to no migrainous features but for some reason these began to occur with pain exacerbations over the past 2 years. There were no cranial autonomic symptoms. She did not have a history of migraine but was prone to motion sickness as a child. She had a remote head trauma 12 years prior to headache onset where a car door hit her in the forehead region. For her headaches she had tried 10 plus migraine preventives including GCRP monoclonal antibodies, as well as onabotulinum toxin A injection therapy with minimal to no relief. She was put in an inpatient headache unit for intravenous medications without benefit and even had bilateral supraorbital/supratrochlear nerve decompression surgery which provided some relief, but she still had a constant daily headache. Neuroimaging studies for secondary etiologies were normal. On examination the patient’s pain was mimicked by palpation over the frontal cranial suture. Anesthetic injection to the suture line (2 cc of 1% lidocaine) provided 70% relief which lasted only 2–3 days. Repeat injection again was of short duration. Thus, onabotulinum toxin A injection treatment only to the frontal suture line was completed (20 units). The frontal suture was not injected during her previous trials of this treatment. She is now status post five rounds onabotulinum toxin A with almost 90% plus improvement and with some pain free time. A novocaine/prilocaine cream combined with a topical ketamine cream is also being used 2× per day over the suture line which seems to have enhanced the preventive effect. The patient was hypermobile, and the hypothesis is that her prior head trauma caused movement of the frontal suture with compression and irritation of the trigeminal sensory afferents within the suture. Then the heaving coughing and sneezing during her presumed viral illness, moved or irritated the frontal suture further with secondary stimulation of the trigeminal nociceptors resulting in a persistent localized daily headache.
Discussion
A possible new type of chronic daily headache is presented. Cranial suture headache can originate from a single cranial suture or several interconnected cranial suture lines on one side of the skull in most instances. Patients develop a de-novo daily headache localized to a certain region of the head. The majority also appear to have had head trauma in the region of their cranial suture headache. The trauma may have been very remote or in close temporal profile to headache onset. All present as a new daily persistent headache with some also fulfilling ICHD-3 criteria for chronic post traumatic headache. 1
Anatomy
Cranial sutures are the fibrous joints that connect the bones of the skull. They are in place to prevent bone separation with external force/injury and to allow skull movement during cranial growth. 2 Cranial sutures close with age, typically beginning to fuse in a person’s mid-twenties, but they can remain open until the fifth to eighth decade of life. 2 –4 Recent post mortem data as well as older studies suggest that the sagittal suture does not completely close until a person is 60 plus years of age, the coronal suture in the mid-50's, while the lambdoid and squamosal sutures do not typically fully fuse until an individuals mid 60’s to early 70’s. 2 –4 The frontal suture, which separates the two halves of the frontal bone, will typically fuse between 3 and 9 months of age. However, the frontal suture can remain open into adulthood in about 4% of women and 2% of men. 5 Estrogen has been shown to have an influence on cranial suture formation and closure, and females appear to close cranial sutures slower than males. 6
There are multiple cranial sutures (see images Figure 1(A) to (D)) and thus numerous possible distributions for cranial suture headache. It appears that most cranial suture headache cases involve the sagittal, coronal and squamosal suture lines, but the author has also noted head pain isolating to the frontal and fronto-zygomatic cranial sutures. The pain is typically linear in property or in essence follows the pattern of the cranial suture line. The key is the examination of the patient to denote the exact location of the pain by palpating the skull and region of pain and to see what cranial suture is involved. Even in nummular distribution pain, it is important to establish if the pain felt by the patient extends beyond the well circumscribed perceived region to other parts of the cranial suture line.
Etiology
Burstein and colleagues have noted a network of sensory (peripherin-stained) and pain (CGRP- and TRPV1-positive) fibers that remain intact within the cranial sutures into adulthood in mouse models. 7 Similar findings are noted in humans. 7 –9 Many of the pain fibers that navigate through the cranial sutures originate from dural nociceptor axons. 7 Thus, cranial suture head pain is hypothesized to result from progressive irritation of these tiny trigeminal nociceptors within the cranial suture lines until they reach a threshold point to generate pain. The initial trigeminal pain fiber irritation is possibly set up by a remote trauma (direct or indirect) and then continued irritation with skull plate movement over time, along with subsequent traumas, even microtraumas (a hard cough, laying on a pillow the wrong way) eventually elicits the headache. The delayed closer of the cranial sutures for almost a complete human lifetime would potentially leave them vulnerable to recurrent injury. 3 In addition, over-calcification of the suture lines could also end up pinching cranial suture line nerves and that calvarial bone pathophysiology, especially calvarial bone marrow may be at the origin of cranial suture-based pain. It is also feasible that some non-trigeminal nociceptors are involved in cranial suture headache, at least in the posterior skull region. It has recently been demonstrated in rat models that the posterior dura overlying the posterior fossa and cerebellum is innervated by the axons of sensory neurons deriving from the C2-3 dorsal root ganglia. These axons appear to enter the cranium (outside to inside) by several modalities of which one is crossing the cranial suture lines. 10
The majority of the patients (9/10) that developed de-novo cranial suture headache were hypermobile (verified by physical therapist), thus one could hypothesize that these patients have more excessive movement of their cranial sutures/skull plates than non-hypermobile individuals and thus are more at risk to develop head pain from cranial suture/trigeminal nociceptor irritation. This with any additional arthritic/inflammatory changes that occur within the cranial sutures could lead to a localized head pain syndrome. Burstein and colleagues have also noted in chronic migraine patients with imploding type pain that the calvarial environment is marked by an activation of pro-inflammatory genes and a suppression of genes that encode immune suppression systems. 8,11 Thus, the cranial suture environment at baseline maybe more prone to inflammation from injury and thus more likely to promote activation of the trigeminal nociceptors that run through the suture lines. As of yet, the calvarial inflammatory environment in cranial suture headache patients is unknown.
The observation that the “cranial suture” headache patients improve with localized anesthetic injection to the suture line(s) and/or onabotulinum toxin injection only to the cranial sutures would seem to suggest the extracranial origin of the pain, while also providing an effective treatment paradigm. The fact that most of the presented case patients did not have central symptoms seems to fully align with an extracranial etiology. However, as 30% of the patients had some central symptoms including migrainous features such as nausea and photophobia, this suggests a possible spectrum of headache extending from extracranial to central etiologies.
Treatment
Each cranial suture headache patient responded to localized injection of anesthetic (1–10 cc of 1% lidocaine depending on length of suture-based pain and number of sutures involved) and in most cases 0.1–1 cc of triamcinolone 40 mg/ml, except for the frontal region sutures in which injectable steroid was not utilized to avoid fat atrophy and skin divots. Depending on duration of headache response either a single or series of anesthetic injections were carried out to see if the headaches could be alleviated. If after one to three rounds of serial injections the duration of headache response did not lengthen, then localized onabotulinum toxin A injection was carried out. All patients have responded to this therapy so far with at least 75% improvement (Table 1) noted, although many have become pain free or nearly pain free. It is imperative the onabotulinum toxin A is injected into the suture line and the entire length of the palpated suture tenderness. This altered injection paradigm of injecting cranial suture lines could even be considered for chronic migraine patients who are not achieving good results with the FDA-approved paradigm for onabotulinum toxin A and who have pain localized to the cranial suture lines on examination.
Limitations
The major limitation in the description of cranial suture headache is the ability of the practitioner to define what cranial suture lines are involved when examining a painful patient. This is especially difficult with the smaller cranial sutures. The major cranial suture lines should be easier to palpate. Thus, the presented case patients with multiple contiguous sutures involved may indeed not have all the cranial sutures affected as listed in Table 1. The lack of a comprehensive sensory examination of the scalp may also make the clinical description of cranial suture headache incomplete. As only 10 patients have been defined, any discussion on gender predominance, unilaterality, lack of a prior migraine history and treatment response is premature. There also needs to be a consideration that cranial suture headache is not a unique syndrome but an offshoot of other epicranial headaches such as linear headache and /or there is at least shared pathophysiology with headaches of presumed extracranial origin. 12,13 Further study is needed.
Conclusion
A well localized headache may indeed be a “cranial suture” headache. Examination is essential to palpate over the cranial suture lines to see if pain can be elicited and if so, does the perceived pain mimic the patient’s daily headache. Cranial suture headache, while being treatment resistant to most medications, appears to readily improve with localized anesthetic injections to the cranial suture lines, while many patients require serial localized onabotulinum toxin injections to get persistent pain relief. Without the recognition of cranial suture-based pain, these patients have unremitting headaches that can last years to decades.
Clinical implications
Cranial suture headache is defined by head pain localized to one of the cranial sutures of the skull. The key is the examination of the patient to denote the exact location of the pain by palpating the skull and region of pain and to see what cranial suture is involved.
Cranial suture headache can present as a daily headache from onset and is typically unilateral. The most common cranial sutures to be affected include the sagittal, coronal and squamosal suture lines.
Cranial suture headache is typically medicine resistant, but readily improves with localized anesthetic injections to the cranial suture lines and/or serial localized onabotulinum toxin A injections
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics or institutional review board approval
Approval by Mayo Clinic Florida IRB.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.