
Abstract
We aimed to evaluate the clinical characteristics and outcome, hospital stay, and intracranial hemorrhage (ICH) development of patients with cerebral venous sinus thrombosis (CVST) who presented with isolated headache. In a retrospective study, consecutive patients with a definite diagnosis of CVST referred to Namazi hospital (Shiraz University of Medical Sciences) from 2012 to 2016 were included. Clinical, radiological, and prognostic characteristics and outcome on discharge (using modified Rankin Scale (mRS)) were compared between the CVST patients who presented with isolated headache and other CVST patients through univariate analyses. The associations of isolated headache with poor outcome (mRS > 2), presence or development of ICH, and duration of hospital stay were assessed through multivariable analyses. Of the 174 patients, 45 (26.0%) presented with isolated headache. Presence of isolated headache was more frequent in men (p value = 0.048) and patients with thrombophilia (p value = 0.040). Lateral sinus involvement was more common in patients with isolated headache (p value = 0.005). After adjustment for other variables, the isolated headache was significantly associated with shorter hospital stay (odds ratio (OR): 0.85, confidence interval (CI): 0.73–0.99) and lower risk of early ICH (OR: 0.314, CI: 0.132–0.749). Although poor outcome was significantly less frequent in patients with isolated headache on univariate analysis (p value < 0.001), this association was not significant in multivariable analysis (OR: 0.324, CI: 0.035–2.985). CVST patients with isolated headache had lower ICH events and shorter hospital stay. CVST should be considered as a possible differential diagnosis in certain patients who present only with headache, particularly those with diffuse progressive headache, or underlying provocative conditions.
Keywords
Introduction
Although the mortality of cerebral venous sinus thrombosis (CVST) has decreased in recent years, 1 it is still one of the most important causes of mortality and morbidity among young adult stroke patients. 2 Accordingly, early diagnosis and initiation of management are crucial. 3,4
Headache is one of the main presenting symptoms of CVST. 5 However, it has been reported as the sole presenting symptom in only 15–32% of the patients. 6,7 The prognosis of CVST patients with isolated headache is better than other patients. 7 Nevertheless, the presence of isolated headache in the absence of more severe neurologic presentations may lead to a delay in medical attention and diagnosis. 3
In this study, we aimed to compare the clinical characteristics and outcome of CVST patients with an isolated headache with patients with additional neurological symptoms.
Methods and patients
In a retrospective study, consecutive patients with a definite diagnosis of CVST based on the established clinical and radiological criteria, 8,9 who referred to Namazi hospital (Shiraz University of Medical Sciences) from 2012 to 2016, were included. This center has a high volume of referrals from the southern provinces of Iran. The study protocol was approved by the institutional review board (IRB) and ethics committee of Shiraz University of Medical Sciences (Approval Code: 13024). The review board waived the need for patient consent.
Patients were identified through the International Classification of Diseases, Tenth Revision (ICD-10) coding system with diagnostic codes of G08 for “Intracranial and intraspinal phlebitis and thrombophlebitis,” O87.3 for “Cerebral venous thrombosis in the puerperium,” and I67.6 for “Non-pyogenic thrombosis of the intracranial venous system.” We included all patients aged more than 18 with a definite diagnosis of CVST made by expert neurologists/radiologists according to the American Heart Association/American Stroke Association statement. 9 We excluded all CVST patients with incomplete medical records and those patients with other neurological disorders rather than CVST such as arterial infarcts, hypertensive intracranial hemorrhage (ICH), brain aneurysms, brain arteriovenous malformation, toxic and metabolic encephalopathies, reversible vasoconstriction syndrome, cerebral vasculitis without venous sinus thrombosis, idiopathic intracranial hypertension without evident venous sinus thrombosis, or any other condition that explained presentations of the patient better than CVST. We included patients in the group who presented with isolated headache if headache was the only major symptom at the time of admission. We used a clinical definition for isolated headache which can be easily applied by a general physician: “Any new headache or headache that could have causal relationship with CVST and led to the diagnosis of CVST was included.” 10 All other neurological symptoms and signs including altered mental status, all types of seizures, decreased level of consciousness, and focal neurological deficit were excluded. Those patients with nausea, vomiting, and papilledema were not excluded from this group. Radiological findings were not included in our categorization of patients into the group with isolated headache and the group with other symptoms and signs with or without headache.
All the included patients had computed tomography (CT), magnetic resonance imaging and venography (MRI/MRV), and/or CT venogram (CTV). Only a few patients had CTV. The diagnosis of CVST in our center was made mainly by MRI/MRV, since MRV is preferable to CTV because of the concerns regarding the radiation and renal toxicity of the contrast. 11 We recorded all demographic data, radiological and clinical findings, risk factors, treatment options, duration of hospital stay, and discharge outcome according to the modified Rankin scale (mRS) by reviewing medical records and picture archiving and communication system. Variables have been previously described 12 and listed in Appendix 1. Laboratory assessments were done in hospital course. Also, malignancy evaluation was performed in case of any clinical finding in history or physical examination which raised the suspicion to the presence of an underlying malignancy. For all the patients except two (who expired before initiation of anticoagulants), anticoagulation with therapeutic doses of unfractionated heparin or low-molecular-weight heparin was initiated as soon as CVST was confirmed.
The primary endpoint of this study was to compare the clinical outcome of patients with CVST who presented with isolated headache, measured by mRS, and to compare it to the clinical outcome of patients with other symptoms. The secondary endpoints were to compare early ICH (E-ICH) and delayed ICH (D-ICH) and duration of hospital stay in patients with isolated headache to those with other symptoms.
Since we evaluated all the patients referring during a certain period of time, we did not calculate the sample size.
For data analysis, we applied IBM SPSS, version 22.0 package (SPSS Inc Released 2009. Version 22, Armonk, New York, USA). Data were cleaned and prepared using appropriate techniques. 13 Considering the low rate and the pattern of missing data, we decided to use complete case-analysis approach. Mean ± standard deviation and absolute and relative frequencies were reported for quantitative and qualitative variables, respectively. We compared the patients with an isolated headache with others through the χ 2, Fisher’s exact, and independent sample t-tests. The associations of isolated headache with the poor outcome (mRS > 2) on discharge, duration of hospitalization, and presence of E-ICH and D-ICH were adjusted with other variables through logistic and linear regression models and unadjusted and adjusted odds ratios (OR), risk difference and 95% confidence interval (CI) were reported. Backward elimination technique was applied for multivariable modeling. We adjusted the multivariable models for duration of hospital stay and other covariates with a univariate p value of less than 0.3. As the frequency of patients with isolated headache and D-ICH was zero, the calculation of OR was not possible. Therefore, we corrected this frequency and replaced the frequency of 0 with 1 in crosstab used for unadjusted OR calculation. Standard errors and 95% CIs were estimated applying bootstrap technique. Conservatively, we applied Bonferroni correction for multiple comparisons (25 tests), and a p value of less than 0.002 was considered statistically significant.
Results
We excluded six patients from our cases due to missing data (missing rate = 3.4%). Among the total of 174 eligible patients, mean age was 37.8 ± 11.2 and 128 patients (73.6%) were women. One hundred and sixty-three patients (94.7%) presented with headache. Headache was the only neurological symptom in 45 patients (26.0%). Table 1 compares the characteristics of patients with isolated headache and other patients. Among men, 17 patients (37.0%) presented with isolated headache, while 28 women (22.0%) had isolated headache (p value = 0.048).
Univariate comparison of clinical and radiological characteristics among CVST patients with isolated headache and those with other symptoms ± headache.
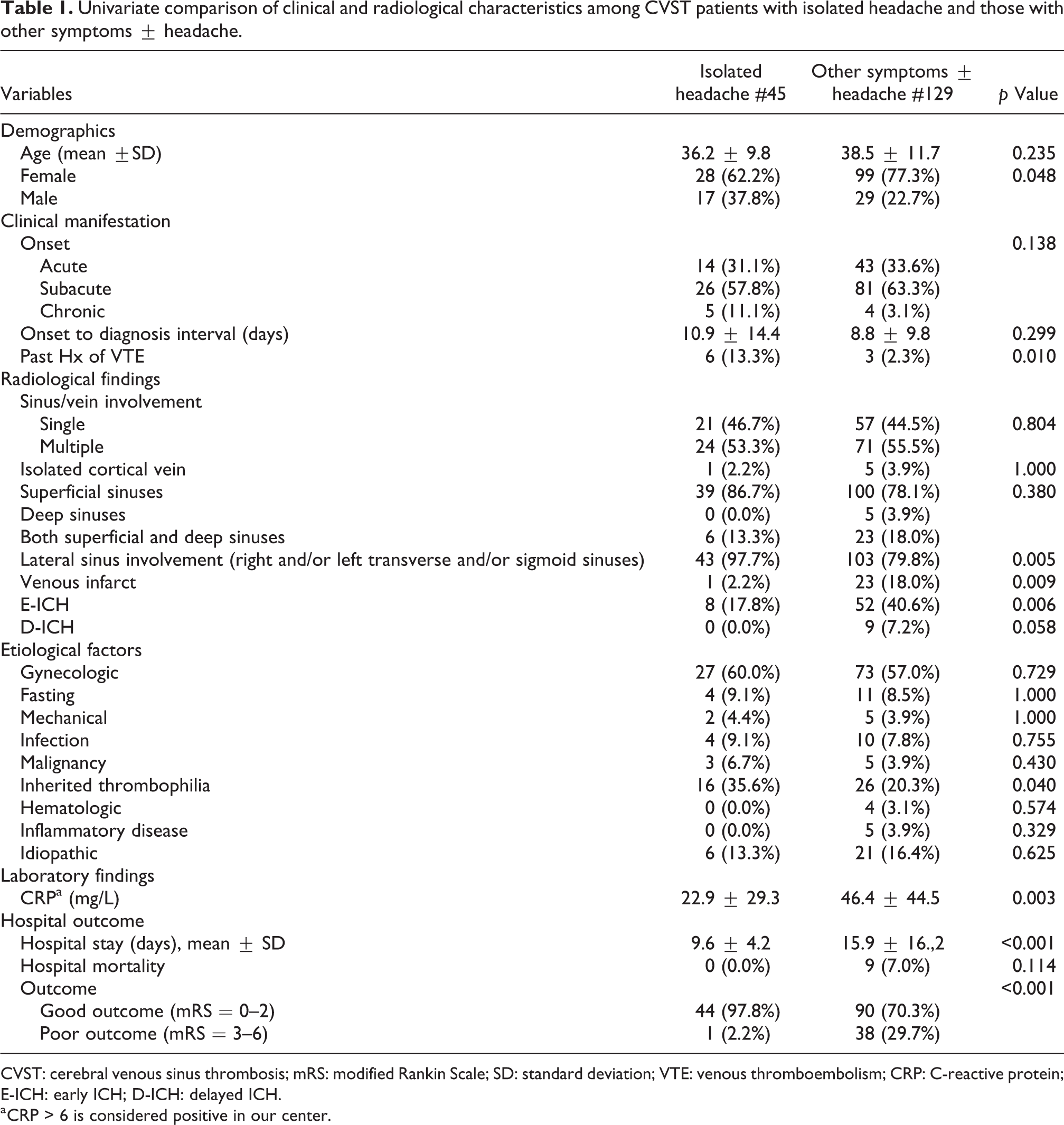
CVST: cerebral venous sinus thrombosis; mRS: modified Rankin Scale; SD: standard deviation; VTE: venous thromboembolism; CRP: C-reactive protein; E-ICH: early ICH; D-ICH: delayed ICH.
a CRP > 6 is considered positive in our center.
The interval between symptom onset and diagnosis of CVST was longer in patients with isolated headache in comparison to other patients, but this difference did not reach statistical significance (p value = 0.299). A positive history of venous thromboembolism (VTE), including previous CVST events, was reported in patients with isolated headache more than others (p value = 0.01). Among the risk factors, inherited thrombophilia was more frequent in patients with isolated headache than others (p value = 0.040). There were no associations between gynecologic causes, malignancies, mechanical precipitants, fasting, hematologic, and inflammatory diseases with the isolated headache manifestation (all p values > 0.002).
Lateral sinus involvement was more common in patients with isolated headache (p value = 0.005). In addition, E-ICH (p value = 0.006), venous infarct (p value = 0.009), and D-ICH (p value = 0.059) occurred less frequently in these patients.
No patient with isolated headache died in hospital, and overall, they had a better outcome (mRS < 2) on discharge than the others (p value < 0.001).
Table 2 indicates the association of isolated headache with poor outcome, ICH, and duration of hospital stay according to multivariable analyses.
Association of isolated headache and poor outcome, E-ICH and D-ICH, and hospital stay in patients with CVST.
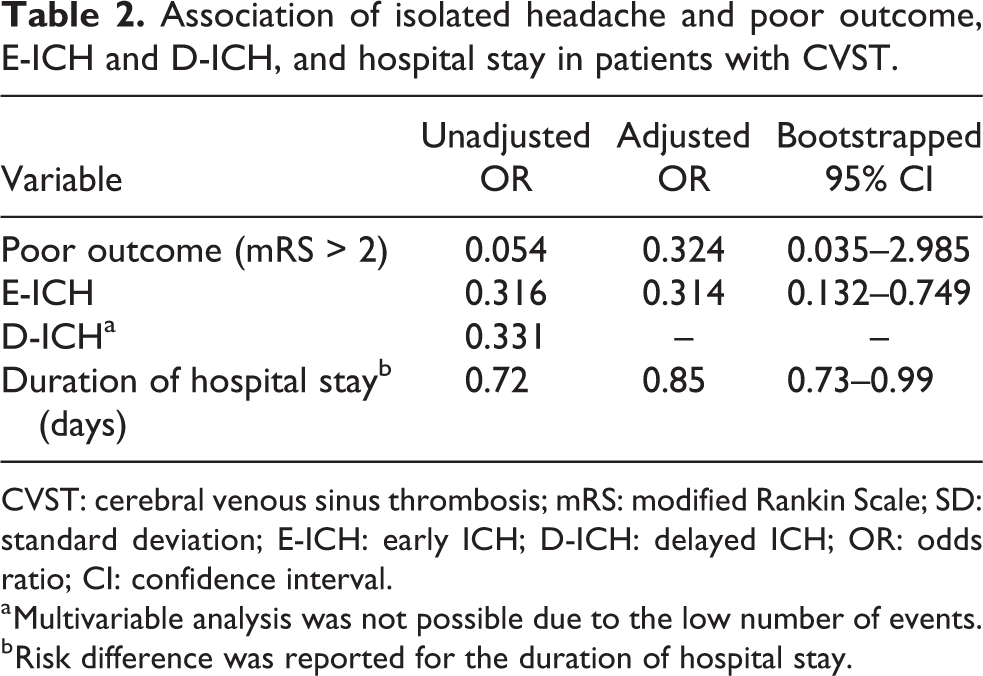
CVST: cerebral venous sinus thrombosis; mRS: modified Rankin Scale; SD: standard deviation; E-ICH: early ICH; D-ICH: delayed ICH; OR: odds ratio; CI: confidence interval.
a Multivariable analysis was not possible due to the low number of events.
b Risk difference was reported for the duration of hospital stay.
Discussion
The present study suggests that almost one-fourth of CVST patients presented with isolated headache, and they had lower odds of hemorrhagic intracranial lesions and shorter hospital stay. Significant better clinical outcome (mRS < 2) in the isolated headache group seen in univariate analysis was not shown in multivariable analysis. In our sample, isolated headache is more frequent in men, patients with thrombophilia, patients with a history of previous VTE, and those with lateral sinus involvement.
Previous studies of headache in CVST are few and mostly from Western countries. 6,14,15 To the best of our knowledge, this is the first study that specifically focuses on isolated headache and investigates the association of isolated headache with poor outcome, hospital duration, and intracranial hemorrhagic events in CVST patients in our region. Our study confirmed the results of previous studies which showed a frequency of 15–32% of isolated headache in CVST patients. 6,7
As a point of strength, we defined the isolated headache based on initial symptoms of patients on admission. Therefore, we did not exclude those with papilledema or any brain lesions on the further imaging workup. This definition leads to a more clinically applicable approach to the patients referring with a chief complaint of headache.
Our results revealed three groups of patients in whom isolated headache has a clinical prominence as a symptom of CVST. First, the frequency of isolated headache was higher in men compared to women (37% vs. 22%). Lower frequency of primary headaches such as migraine and tension-type headaches in men 16,17 may contribute to a higher rate of diagnostic work-ups to evaluate secondary causes of headaches such as CVST in men. This can explain the observed difference in sex distribution in our study. However, because CVST is more common in women, 5 physicians may not consider CVST as an important differential diagnosis in men who refer only with headache. This may lead to a delayed or missed diagnosis of CVST in men.
Also, in our study population, having a previous history of VTE was more frequently seen in CVST patients with isolated headache compared to those who had other symptoms. One explanation could be that physicians tend to be more cautious in diagnosing CVST and perform diagnostic tests and imagings earlier and more frequently in those with the previous history of thrombotic events. Therefore, CVST was diagnosed more frequently in this group compared to the patients without a history of VTE. This necessitates the importance of taking a thorough history from patients referring to the health-care services with a headache and having CVST in mind as a possible diagnosis. Furthermore, in CVST patients with isolated headache, inherited thrombophilia was observed more frequently. In most of the cases, hereditary thrombophilia was diagnosed in the hospital work-ups performed to find out the cause of CVST.
Lateral sinuses thrombosis was more common in the group with an isolated headache. Thrombosis in lateral sinuses less likely leads to ischemic or hemorrhagic brain lesions. 18 Therefore, severe neurological symptoms present less frequently in such patients.
The mean duration between the onset of symptoms and confirmation of the diagnosis (with imaging) was 10.9 ± 14.4 days for patients with isolated headache. Although not significant, the interval between onset of symptoms and confirmation of diagnosis was slightly longer in patients with isolated headache. This delay did not contribute to a poorer outcome in the present and other studies. 7
We assessed the association of isolated headache with undesirable events such as E-ICH, D-ICH, poor outcome, and duration of hospitalization. Although the association between presence of isolated headache and better mRS score was significant in univariate analysis, it was not significant after adjustment for other variables in multivariable analysis. This could be attributed to the small sample size in our study. In a previous study, no association between presence of ICH and headache was detected. 19 After correction for other variables, the isolated headache was associated with a lower odds of E-ICH and shorter hospital stay. Patients with intracranial hemorrhagic lesions typically present with more severe neurological symptoms rather than isolated headache. However, according to our univariate analysis, patients with isolated headache on admission are also at lower risk of developing delayed hemorrhagic lesions in course of hospital. In the dynamic course of CVST, if the patients with isolated headache had later developed ICH, they would have presented with other neurological manifestations. Nevertheless, our results show that the odds of developing D-ICH are lower in this group; therefore, we assume that these patients are in nature less probable to develop ICH and suffer from a less severe thrombosis. This can explain that the lower mRS scores, better outcome at the time of discharge, and shorter hospital stay could be the result of the overall milder disease course and the lower odds of clinical deterioration including D-ICH in such patients. This contributes to a decline in the hospitalization expenses.
Patients with isolated headache are considered to be in the benign spectrum of CVST. Nevertheless, if they had stayed undiagnosed, these patients might have progressed into more severe conditions leading to dramatic symptoms. As a result, early diagnosis of CVST in patients with headache leads to early initiation of treatment and may prevent progression of the disease; therefore, improve the outcome, 3 shorten the duration of admission, and reduce the burden of the disease on health systems. To achieve this goal, education of both clinicians and people at risk of CVST, about the significance of headache as an initial symptom of CVST, seems to be necessary.
One of the limitations of this study was the limited number of patients, therefore a few numbers of events such as D-ICH were detected which limited the multivariable analysis. Furthermore, we could not include those CVST patients with isolated headache who did not refer to our center and their outcome is undetermined. This could be a source of bias in the present study. Also, the retrospective nature of our study limited a systematic, complete laboratory assessment of thrombophilia. Therefore, we probably underdiagnosed thrombophilia as a cause of CVST in our patients. This may influence the generalizability of our results regarding the association of thrombophilia and isolated headache. However, since the missing data occurred randomly in both groups of patients with isolated headache and others, we believe that the direction of this association is not affected.
In conclusion, CVST patients can present with isolated headache. Hence, CVST should be considered as a possible differential diagnosis in patients presenting with headache. Presenting with isolated headache is associated with fewer complications of CVST and better clinical outcome; however, prompt diagnosis and initiation of therapy are recommended to prevent deterioration and poor outcome.
Clinical implications
Isolated headache is significantly associated with shorter hospital stay and lower odds of CVST complications such as ICH.
Diagnosed CVST patients with isolated headache are considered to be in the benign spectrum of the disease.
Early diagnosis of CVST patients with headache can prevent progression of the disease to more severe stages.
CVST should be considered as an important differential diagnosis in patients with isolated new-onset headache who seek medical care.
It is necessary to educate both clinicians and people at risk of CVST, about the significance of headache as an initial and only symptom of CVST.
Footnotes
Acknowledgements
The authors would like to thank the Clinical Neurology Research Center of Shiraz University of Medical Sciences for assistance in this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office of the Vice Chancellor for Research at Shiraz University of Medical Sciences [Grant Number 13024].