
Abstract
Introduction
The evaluation of red flags is crucial for the accurate the diagnosis of headache disorders, especially for thunderclap headache. We analysed if secondary headache disorders were adequately ruled out in patients that presented to the emergency room with thunderclap headache.
Methods
In this retrospective cohort study, we screened all patients that visited the emergency room for headache, including those that described thunderclap headache. We measured the frequency with which secondary causes were not adequately ruled out. We analysed the order of the exams, the final diagnosis, and the time elapsed between arrival, initial request for imaging, and the completion of the imaging.
Results
We screened 2132 patients, and 42 (1.9%) fulfilled eligibility criteria. Mean age was 43.1 ± 17.1 years, and 57% of patients were female. For 22 (52.4%) patients, the work-up was incomplete. Vascular study was missing in 16 (38.1%) patients, cerebrospinal fluid evaluation in nine (21.4%), and magnetic resonance imaging in seven (16.7%), with multiple assessments missing in six (14.3%). There were ten different combinations in which the exams were performed, with the most frequent being the second exam’s cerebral spinal fluid evaluation in 18 (52.9%) and the computed tomography angiogram in 10 (29.4%). A secondary cause of thunderclap headache was found in 16 (38.1%) patients, and four (9.5%) had a primary headache diagnosis after an adequate and complete study.
Conclusions
Thunderclap onset was described in one of every 50 patients that visited the emergency room for headache. More than half of these patients were not adequately managed. More than a third of thunderclap headache patients had a secondary cause.
Keywords
Introduction
Headache is one of the most common medical conditions, reportedly having a 1-year prevalence that ranges from 24% to 85% worldwide (1). The International Classification of Headache Disorders (ICHD) differentiates between primary and secondary headaches based on the cause (2), but the severity and potential consequences of secondary causes are highly variable, ranging from completely benign to life-threatening (3).
Biomarkers for diagnosing headaches are insufficiently validated (4). Hence, diagnosis of headache is still based on anamnesis and physical examinations (5). Some signs and symptoms are associated with a higher odds of life-threatening headache disorders, the so-called red flags (6). Several authors have collected and summarised different lists of red flags (6,7), but validation studies for their use in diagnosis are still scarce (8–11). Some individual red flags have been specifically studied, and probably the best investigated and most widely accepted is the thunderclap onset (8–13).
Thunderclap headache (TCH) is defined by the presence of severe head pain with an abrupt onset, reaching the maximum intensity within 1 min and lasting for at least 5 min (2,14,15). Traditionally, TCH has been associated with subarachnoid hemorrhage (SAH), so most of the guidelines for TCH focus on ruling out SAH (12,13,16–18). Indeed, some authors, suggest that current Computed Tomography (CT) technology is highly sensitive for SAH when performed within 6 h of headache onset, eliminating the need for lumbar puncture (LP) (19,20). However, further research has shown that many other conditions might manifest as TCH (21). This complicates the work-up and implicates that non-enhanced cranial tomography and lumbar puncture may not be sufficient to exclude all secondary causes (4,7,14,15). The ICHD states that a primary TCH can be diagnosed only after all organic/secondary causes are adequately rejected, implicating normal brain parenchyma, intracranial vessels, cerebrospinal fluid (CSF) opening pressure, and CSF composition (2). Given that vasoconstriction may not be observed in the early stage of reversible cerebral vasoconstriction syndrome (RCVS), primary TCH diagnosis should not even be made temporarily (2,22).
In the present study, we aimed to evaluate how often a secondary headache disorder was adequately ruled out in patients that presented to the emergency room (ER) with TCH. We analysed whether the management of patients with TCH was adequate and whether it was in line with the ICHD recommendations. We did not restrict the study to any specific secondary cause of TCH and accounted for all possible etiologies. We aim to detect possible areas of improvement and to raise the awareness of the importance of adequate TCH management.
Patients and methods
This is an observational descriptive study with a retrospective cohort design. The study population included patients that visited the ER for headache. The eligibility criteria were based on the ICHD definition (2). Patients were included if it was explicitly stated that i) headache was the main reason for the consult, ii) headache intensity was described as severe (i.e. as a score of seven or more on a 0–10 numeric rating scale [NRS]), iii) headache onset reached the maximal intensity within the first minute, and iv) the headache lasted at least 5 min. Patients were excluded if a) they were unable to precisely describe the headache characteristics, b) the information about the episode was not complete, or c) traumatic injury to the head or neck occurred in the preceding 7 days.
The study was done in the ER of the San Carlos University, a tertiary hospital with a reference population of 600,000 patients located in the centre of Madrid, Spain. The hospital has 24/7 neurology ward availability. The study period was between 1 January 2012 and 31 July 2014. We used a probability sampling method. We screened the ER electronic health records of all consecutive patients that visited the ER for headache. Data was sourced from both the information provided at triage and the data gathered during the clinical evaluation.
Ethics approval
The local ethics review board approved the study (CP14/425-E) and we adhered to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines (24). The study was done according to the principles of the Declaration of Helsinki.
Study endpoints
For the primary endpoint, we analysed if a secondary headache disorder was adequately ruled out, defined by the exhaustive search for a secondary cause with a complete study in the case that the preceding tests were normal. According to the ICHD (2) this should include: i) parenchymal evaluation, usually by cranial CT; in case of no abnormal findings, the study should be completed with ii) an LP, including opening pressure determination and CSF composition analysis; and iii) a cranio-cervical vascular evaluation including an arterial and venous study, either with CT angiography (CTA), magnetic resonance angiography (MRA) or digital subtraction angiography (DSA). In the case that all the preceding tests were normal, iv) a complete parenchymal evaluation by using magnetic resonance imaging (MRI) should be done. Patients with normal CT results were considered to be fully evaluated regardless of whether they underwent LP or CTA first, as long as they completed the study afterwards, in the case of no abnormal findings being found.
The secondary endpoints were i) to describe the order in which the exams were requested; ii) to list the final diagnosis of patients; iii) to describe the time elapsed between a) the arrival of the patients to the ER and the request of the first cranial imaging and b) the first cranial imaging to the completion of the study, iv) to describe the time elapsed between a) the arrival of the patient to the ER and the LP and b) the first cranial imaging and the LP. We also reported the percentage of patients that were evaluated by a neurologist, the percentage of patients that were admitted, and the percentage of patients that were discharged without further examination. As an exploratory endpoint, we assessed if the CT was requested within 6 h of arrival to the ER, if it was completed within 6 h of arrival (19), and whether or not CT detected the presence of SAH in patients with SAH as a final diagnosis (20).
Assessment
Two neurologists who primarily see patients in headache units (NGG and DGA) reviewed electronic health records of all the patients that visited the ER during the study period, assessing eligibility criteria and extracting the data accordingly. We analysed demographic variables, including sex, age, and prior history of headache. The clinical variables were i) time between arrival and the request for CT and ii) time between that request and the performance of the first imaging. We also describe the examinations that each patient underwent and the accompanying results. We describe the final diagnosis according to the ICHD 3rd version as it was published at the time of the analysis. For RCVS diagnosis, we analysed whether patients also fulfilled radiologic and CSF criteria and if any radiologic findings normalised in follow-up studies (23). We analysed whether patients had been evaluated by a neurologist and if they were discharged directly from the ER.
Statistical analysis
We present qualitative data as frequencies and percentages. Quantitative variables are presented as means and standard deviations (SD) or medians and interquartile ranges (IQR) depending on the type of distribution. For hypothesis testing of both qualitative and quantitative variables, we used Student’s t-tests for variables that had a normal distribution or Mann-Whitney U tests otherwise. We analysed the timing of the exams by using Kaplan-Meier curves and presented these data in 1-survival plots. We considered p-values to be significant if the value was lower than 0.05. Missing data were managed by using complete case analysis. Sample size was not calculated in advance, and the analysis was based on the available data. We used SPSS v.26.0 (IBM Corp. Armonk, NY) for the statistical analysis, and the figures were created using BioRender.
Results
During the study period, 2132 patients visited the ER for headache and were screened; 71 patients fulfilled the inclusion criteria and 29 patients were excluded, leaving 42 (1.9%) patients to be included in the analysis. Figure 1 shows the flow diagram.
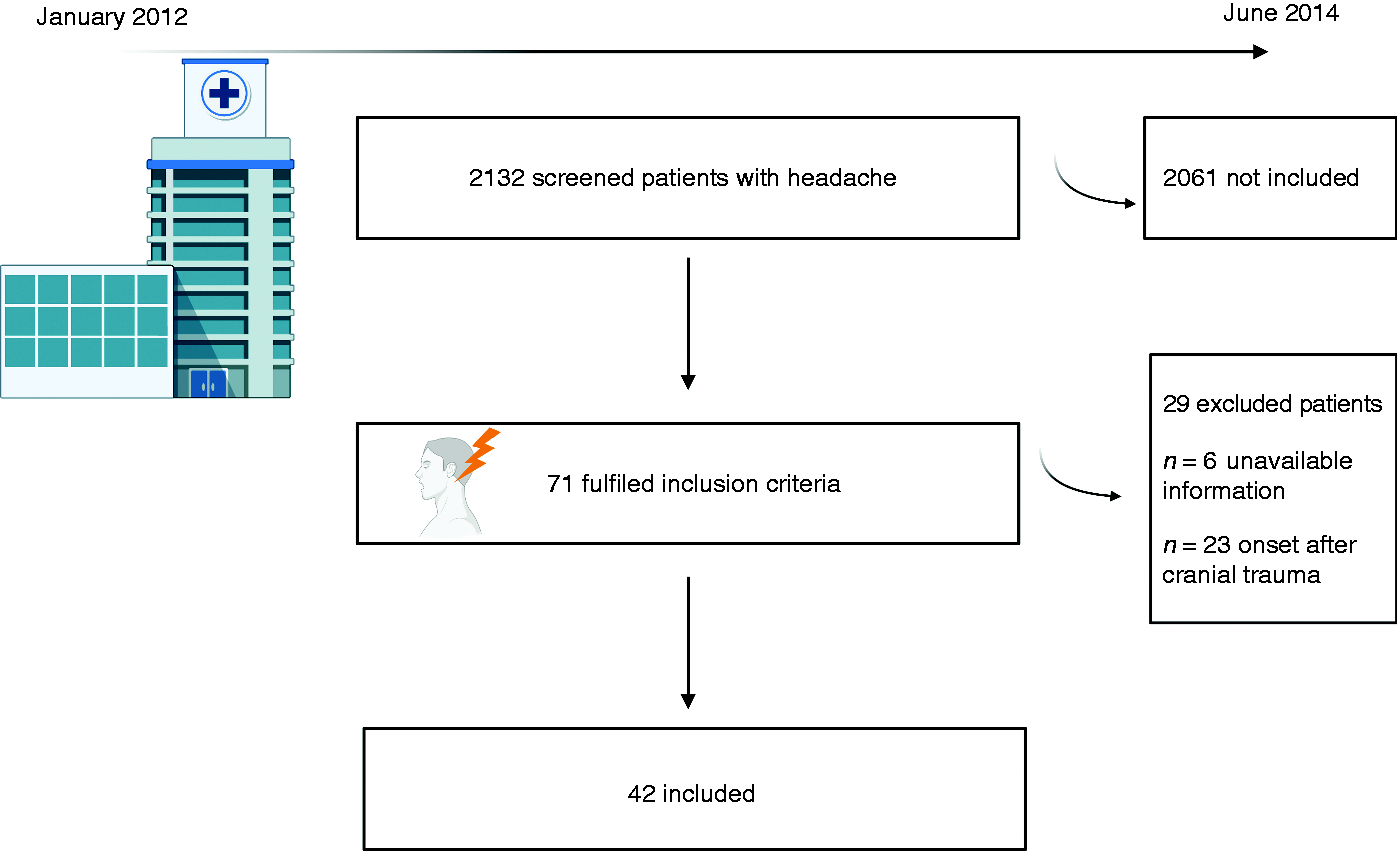
Flow diagram of the study.
Table 1 summarises the demographic variables and the global frequency of each exam. The first complementary exam was CT in all patients. Of the 34 patients with a “normal” CT, the second exam was an LP in 18 (52.9%), a CTA in 10 (29.4%), and an MRI in two (5.8%); four (11.7%) patients did not undergo further exams.
Demographic variables and frequency of exams.

CT: cranial tomography; CTA: cranial tomography angiography; MRI: magnetic resonance imaging.
Primary endpoint: Adequate exclusion of secondary headache disorders
In 22 out of 42 (52.4%) patients, the work-up was incomplete and secondary causes were not sufficiently ruled out. Vascular evaluation was absent in 16 (38.1% of the entire sample, 72.7% of patients with incomplete work-up) cases, CSF evaluation in nine (21.4% of the entire sample, 40.9% of patients with incomplete work-up) cases, and MRI in seven (16.7% of the entire sample, 31.8% of patients with incomplete work-up) cases. In 6/22 (27.3%) patients, multiple exams were absent. Eight (19.0%) patients received a primary headache diagnosis during their stay in the ER, despite the exam being incomplete; of these, five were diagnosed with migraine, two with primary headache associated with sexual activity, and one with tension-type headache.
The order of the exams
The first complementary exam was cranial CT in all cases with positive findings in 8/42 cases (19.0%). The second exam was an LP in 18 (52.9%) patients, a CTA in 10 (29.4%), absent in four (11.7%), and an MRI in two (5.8%). The order in which the exams were done showed 10 different combinations, presented in Table 2. Figure 2 depicts the order of the exams in the whole sample and the results. Neurologists evaluated 28 (66.7%) of the patients.
The different combinations in which the studies were requested and completed.

CT: cranial tomography; LP: lumbar puncture; CTA: cranial tomography angiography; MRI: magnetic resonance imaging.

The number and type of exams done per patient, accounting for all included cases, with final diagnosis. In red, patients with a primary headache diagnosis in which a secondary headache disorder was not adequately ruled out.
Final diagnosis
In those patients who were properly studied, a secondary cause of the TCH was found in 16 patients (38.1% of the entire sample, 75% of the adequately studied patients). Eight patients had SAH, caused by aneurysm rupture in five. Two patients fulfilled criteria for RCVS (23) and two for intracerebral hemorrhage secondary to arteriovenous malformation rupture. One patient had amyloid angiopathy-associated intracerebral hemorrhage, one patient had CSF low-pressure headache, one patient had an unruptured intracranial aneurysm, and finally, one patient had a pituitary space occupying lesion with bleeding signs in the MRI. Two out of the eight patients with a final SAH diagnosis had a negative CT initially, and one even had a negative CTA initially (Figure 2). In four (9.5%) patients in which a secondary cause was adequately ruled out after complete work-up and follow-up, the final diagnosis was a primary headache, including primary headache associated with sexual activity in two patients, primary TCH in one patient, and primary cough headache in one patient (Figure 2).
Timing of the exams
Median time from arrival to the CT request was 68.0 min (IQR: 47.7–188.7, range 3–805 min; Figure 3). Median time from CT request to its performance was 66.0 min (IQR: 30.0–98.0, range 4–279 min; Figure 4); imaging was completed within 1 h after its request in 20/42 patients (47.6%) and within 1 h of patient arrival in 18/42 subjects (42.8%). CT was requested within 6 h of patient arrival in 37/42 (88.1%) of patients and completed within 6 h of arrival in 32/42 (76.2%) patients, including seven out of eight patients with a final diagnosis of SAH.
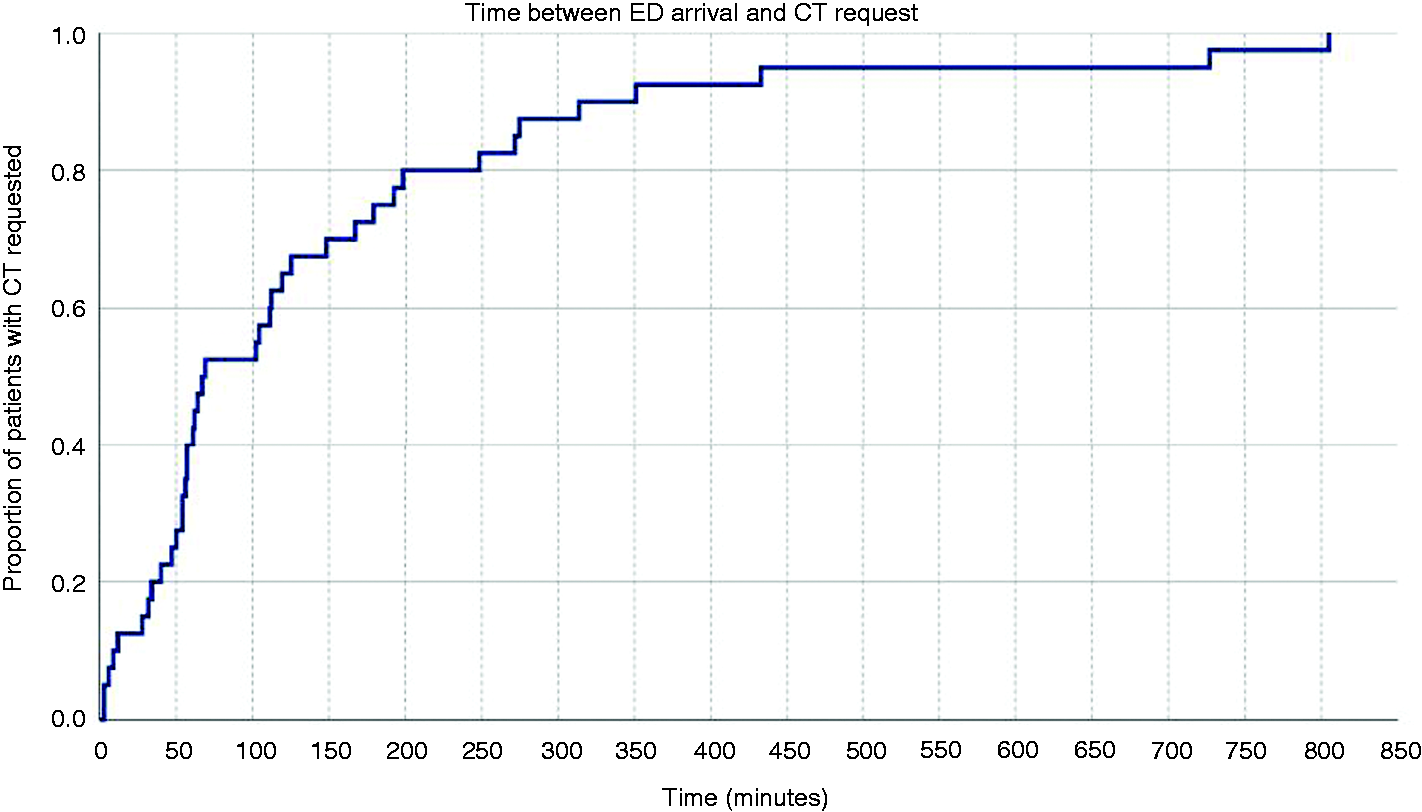
1-survival plot of time between emergency room (ER) arrival and the cranial tomography (CT) request, in minutes.
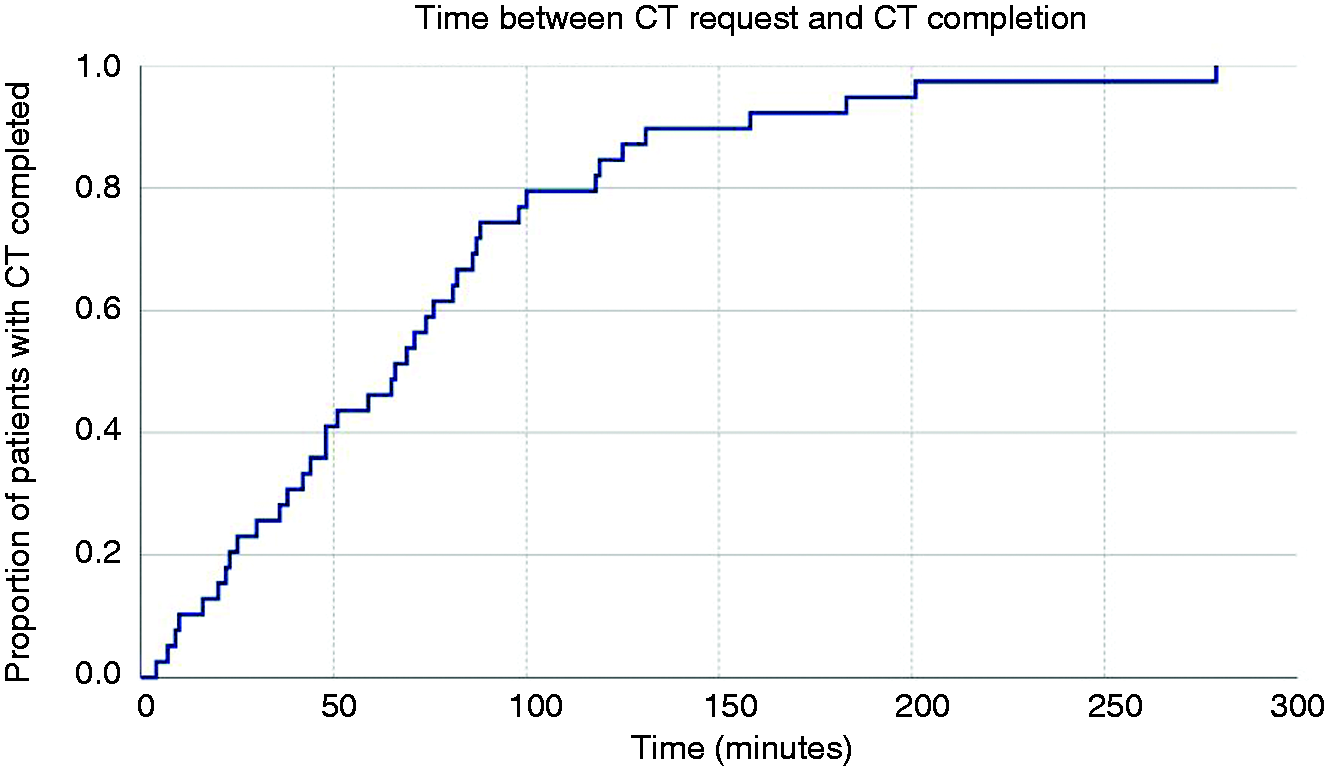
1-survival plot of time between cranial tomography (CT) request and exam completion, in minutes.
In patients in which the neurologist on call was consulted, the CT was completed 158.7 min (sd: 190.3) after the patient’s arrival compared with 86.6 min (sd: 72.6) for patients not evaluated by a neurologist; however, the difference was not statistically significant (p = 0.10). Time between CT request and completion did not differ in patients with or without neurological evaluation (76.1 min vs. 65.0 min respectively, p = 0.65). The time between patient arrival and the LP was 262.2 (SD: 146.4) min, and the time between the first imaging and the LP was 83.5 (SD: 60.5) min.
Discussion
In the present study, we analysed the management of patients who visited the ER for headache and described thunderclap onset of pain. We did not restrict our study to any specific etiology, as TCH might be caused by several disorders (22). We adhered to the ICHD criteria, both for the definition of TCH onset and for the classification of patients as adequately managed (2). The main finding of our study was that management of patients was not adequate in more than half of the cases. There was no clear order to the diagnostic exams. TCH was a rare but not exceptional presentation form of headache in the ER, accounting for almost 2% of all headache visits. At least one third of the patients with TCH had a secondary cause. Seven secondary causes of TCH were found, and three additional primary causes were found with complete work-up.
Inadequate management of TCH patients might reflect that headache education is still insufficient. Other authors have previously shown that up to 38% of patients visiting the ER with their “first or worst” headache were discharged without any complementary exam (9). A survey of 160 Scottish physicians (25), 137 of them consultants or specialists, showed that 3% of the participants would discharge a potential TCH patient without a CT scan and 6% after a basal CT scan.
In our series, headache had a thunderclap onset in 1.9% of all patients visiting the ER for headache, which is similar to that of other previously reported series of around 1.5% (15). The frequency in our population could be underestimated as we only accounted for those patients in which the headache fulfilled the TCH definition in the electronic health records. Despite a systematic review of all reported causes depicting 119 potential different causes (22), most of the studies focus on SAH (11,12). For that reason, some guidelines consider that the diagnostic study is complete after a normal CT and LP. However, other series have shown a total number of six different causes within 137 cases (12), or 14 different causes within 433 cases (11). In our study, seven different secondary causes were observed, highlighting the importance of a complete and extensive diagnostic study.
Incidence of SAH was estimated to be 9.9 per 100,000 person-years in a large population-based study in Queensland (26); one of every four patients admitted to the hospital with SAH expired, one in 50 ER patients with headache as the chief complaint had SAH, and one in 5000 ER patients with any chief complaint had SAH. In that study, there were nine other causes of secondary headache, accounting for 4.2% of all headache visits (26). Frequency of SAH in the reported series of patients with TCH varies between 6.2 and 17% (8,12,16–18,26), with a pooled frequency of SAH in TCH patients of 334/4659 (7.2%) when including patients of those studies and the present study.
There is no doubt of the need for an immediate CT in patients with TCH (10,27). Thunderclap onset of the headache must be evaluated during triage of headache patients and incorporated within the different triage systems. In our series, median time between arrival and CT request surpassed 1 h. This time should be minimised as much as possible, considering that some etiologies are time dependent (14,15,19,25). In the case of a negative CT, an LP should be considered, including xanthochromia determination and opening pressure measurement (28,29). If both CT and LP are negative, agreement concerning the next step is not clear, but most authors concur that MRI and vascular evaluation should be done. The vascular evaluation should include both arteries and veins and can be done by either MRA and magnetic resonance venography, CT angiography and CT venography, or even four-vessel DSA (4,14,30). In our study, two SAH diagnoses were made after LP, with one of these even after a false-negative CTA. Guidelines should clearly state that both LP and vessel evaluation are equally important to TCH management (30).
Work-up proposals made by radiologists describe all of the differential radiological etiologies that can be found (31), including small dural arteriovenous fistulas, arteriovenous malformations, arterial dissections, colloid cysts at the third ventricle, and cerebral venous sinus thromboses. Many of these cannot be completely ruled out without completing all aforementioned imaging modalities, and sometimes it is even necessary to repeat imaging after 3 months (31–33).
Some researchers argue that CT might be sufficient to rule out subarachnoid bleeding if the scan is normal and is done within 6 h of the TCH onset (19,20,27,34). However, other secondary headache disorders can be responsible for the TCH, and even in those studies, 4.0% (19) to 9.3% (27) of patients showed a cause of TCH different from SAH, half of them diagnosed only by LP (25). The 6-h CT rule showed a 95.5% sensitivity rate in a prospective multicenter study in the diagnosis of SAH, reporting 188 cases of SAH out of 3672 patients with TCH (20). False negatives were observed in two cases of unruptured aneurysm and presumed traumatic LP, one case of underreading by the radiologist, one case of dural vein fistula, and one case of sickle cell anemia (20). In our study, two out of eight patients with a final diagnosis of SAH had a normal CT, only being detected after a positive LP. This could be related to the use of less sensitive CT scans, given that the study was done between 2012–2014.
Besides the fact that the headache phenotype of SAH cannot be distinguished from other secondary headache disorders (8), only a complete work-up can rule out a severe condition (2,14,28). In addition, mathematical models have shown that LP is more cost-effective and has a higher utility compared with CTA (35).
Some clinicians criticise the attribution of unruptured cerebral aneurysms as the cause of TCH, considering that they might be an incidental finding (36). However, the first description of TCH by Day and Raskin in 1986 was made in a patient with unruptured cerebral aneurysm that also exhibited diffuse cerebral vasospasm in both anterior and posterior circulation of both hemispheres (37). Some studies show that TCH might be the sole preceding symptom of SAH (38). A meta-analysis of nine studies of patients with aneurysmal subarachnoid hemorrhage showed that the percentage of SAH patients with sentinel headache varies between 10 and 43% (39).
A rising cause of TCH is RCVS, even though its frequency within the available studies is highly variable or even nonexistent (11,16). This could be related to the fact that until Calabrese and collaborators coined the term RCVS (40), cases were diagnosed under many different names, such as isolated benign cerebral vasculitis (41), migrainous vasospasm (42), acute benign cerebral angiopathy (43), reversible segmental vasoconstriction syndrome (43), Call-Fleming Syndrome (44), and central nervous system pseudovasculitis (45). RCVS is probably the condition in which TCH is the most frequent onset (14,15,22). Its adequate diagnosis requires precise vessel evaluation by using CTA, MRA, transcranial doppler or even angiography (22). Follow-up of patients with TCH is essential, as the vascular abnormalities might be delayed (23) and therefore the complete work-up may be falsely negative if done immediately. A delayed MRI and/or MRA might be necessary to properly assess arterial vasoconstriction, hidden or concealed aneurysms, or venous sinus thrombosis, but it should never substitute for the CSF and vascular evaluation.
The main limitations of our study are the inclusion of only a single centre, the small sample size, the retrospective nature, and the lack of correlation of the findings with the rest of the clinical presentation. The frequency of TCH might be underrepresented because of the study design, as we only included those patients in which the headache had a clear thunderclap onset. The study analyses a sample from 2012–2014, but we do not expect that there has been a significant change in the management or the epidemiology of TCH causes from then to today. Among the strengths of the study, we described management of TCH in a real-world setting, describing for the first time the precise order in which the exams were accomplished. Future studies should consider that the high number of possible etiologies of TCH exceeds that of SAH (5,10), and the use of rules based on clinical scenarios might be helpful for the clinicians (3,13) but should not exclude the stepwise approach that should be done in every patient presenting with TCH.
Conclusions
More than half of the patients in this study were not adequately managed. Almost a fifth of patients received a primary headache diagnosis even though the diagnostic study was not completed. Thunderclap onset was described in one of every 50 patients who visited the ER for headache. More than a third of TCH patients had a secondary cause.
Clinical implications
Thunderclap headache should be always considered a red flag and included in the triage of every patient with headache in the emergency room. Many different secondary headache disorders might present as a thunderclap headache. Future work-up recommendations should explicitly recommend CSF opening pressure determination, CSF composition, adequate vascular examination, including intracranial arteries and veins and cervical arteries, and brain parenchyma evaluation with MRI.
List of abbreviations
ICHD: The International Classification of Headache Disorders
TCH: Thunderclap headache
SAH: Subarachnoid haemorrhage
CSF: Cerebrospinal fluid
ER: Emergency Room
NRS: Numeric Rating Scale
STROBE: Strengthening the Reporting of Observational studies in Epidemiology
CT: Computed tomography
LP: Lumbar puncture.
CTA: Cranial tomography angiography
MRA: Magnetic resonance angiography
DSA: Digital subtraction angiography
MRI: Magnetic resonance imaging
SD: Standard deviation
IQR: Interquartile range
RCVS: Reversible cerebral vasoconstriction syndrome
AVM: Arterio-venous malformation
Footnotes
Acknowledgements
We thank the department of emergency medicine for their support and collaboration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The Clinical Research Ethics Committee of Hospital Clinico San Carlos approved the study.
The present work has been partially presented at the LXVIII Spanish Society of Neurology Congress.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.