
Abstract
Background:
Surface imaging is a promising, noninvasive approach to assess regional perfusion in craniovascular disorders such as migraine.
Methods:
We used optical imaging to examine differences in facial blood volume at baseline and in response to ammonia inhalation (a noxious stimulus), as well as standardized measures of cardiovascular autonomic function, in healthy, non-headache controls (n = 43) and in interictal migraine subjects (n = 22).
Results:
Resting facial cutaneous oscillation (FCO) frequency was significantly different in migraine compared to healthy controls. Following ammonia inhalation, healthy controls showed a significant increase in resting FCO frequency, whereas this response was not significant in the migraine group. Standardized autonomic reflex parameters did not differ significantly between study groups, and facial cutaneous activity did not correlate with standardized cardiovascular autonomic reflex parameters, suggesting potentially different regulation.
Conclusions:
This approach to the assessment of craniofacial hemodynamic function appears to exhibit differing mechanisms from previously available techniques, and represents a promising new physiological biomarker for the study of craniofacial vascular function in migraine and potentially other craniovascular disorders.
Introduction
Altered trigeminovascular function is a key feature of migraine pathophysiology. 1 Prior studies suggest that ictal extracranial vascular dysfunction may link to trigeminovascular reflex activation. 2,3 Furthermore, craniofacial autonomic signs and symptoms are frequently evident in migraine, 4 –8 yet studies evaluating classic measures of systemic cardiovascular autonomic function have been inconclusive. 9,10 In contrast, studies of vascular reactivity, including those of the trigeminovascular response, 3,11,12 have shown promise in the study of migraine, with evidence to suggest altered vascular function both extra- and intracranially. 13 –15
In recent decades, several optical techniques have been developed for noninvasive and noncontact blood perfusion imaging, including laser Doppler flowmetry (LDF), laser speckle contrast techniques, optical imaging, and photoplethysmography; however, recent applications to facial structures have focused on pulsatility 16,17 and surrogate markers for systemic cardiovascular function (heart rate, blood pressure (BP)). 18 –20 In an effort to better examine intrinsic vascular function of the craniofacial region, we developed a technique adapted from our work in animal model systems, 21,22 utilizing surface imaging to register spontaneous oscillatory hemodynamic changes in the skin (facial cutaneous oscillations (FCOs)) to examine differences in facial blood volume in response to trigeminovascular reflex stimulation, as well as standardized measures of cardiovascular autonomic function (heart rate variability and baroreflex responses). Here we present validation of the technique in healthy controls, along with a comparison to migraine subjects.
Materials and methods
Subjects
In total, 65 subjects (38 female, 27 male) aged 15–75 years were recruited into migraine (n = 22) and age- and sex-matched healthy, non-headache control (n = 43) groups. Subjects were recruited between June 2013 and March 2017 from the local community, community clinics, and the University of Utah Headache and Outpatient Neurology Clinics, via word of mouth, Internet, and flyer advertisements. The study procedures were approved by the University of Utah Institutional Review Board (IRB_00064447), which is registered with the US Federal Office of Human Research Protections and subscribes to the principles set forth in The Belmont Report and the International Conference on Harmonization’s Good Clinical Practices in human research; informed consent was obtained for all study subjects.
Control subjects were identified based on the following characteristics: no history of recurrent or disabling headaches, nor of any neurological or medical disorder for which regular medications were taken. Headache diagnosis was based on International Classification of Headache Disorders IIIb criteria 23 via a structured clinical questionnaire modified from Samaan et al. 24 Migraine subjects were included who qualified for episodic or chronic migraine; headache not fitting migraine criteria and/or probable migraine were excluded from this group. Subjects were excluded if they had comorbid medical or neurological disorders known to directly affect cardiovascular or craniofacial autonomic function. Subjects were instructed not to exercise or consume alcohol, caffeine, or nicotine for at least 4 h prior to testing.
Episodic migraine participants were studied after being headache-free for at least 48 h, and subjects were excluded from analysis if a migraine occurred within 24 h of testing; chronic migraine subjects were assessed when migraine attack-free for at least 48 h, though testing during daily or non-migrainous headaches was permitted. Subjects had not used opiate medication or migraine-specific abortive medications during the 48 h prior to testing and did not take any medications that could affect autonomic function, including psychotropics, antihistamines, tricyclics, BP agents, and benzodiazepines or their derivatives. The group of healthy control subjects were studied in their usual state of health and met the same medication exclusion criteria.
Experimental setup for facial imaging
The experimental system, shown in Figure 1, consisted of a computer, camera, lens, and an LED light source. Subjects were instructed to lie on their back, facing the camera positioned directly above; electrocardiogram (ECG) leads and a respiratory monitor (strain-gauge) were placed in order to obtain heart and respiratory rates. The upper 2/3 of the face was illuminated with two 567 nm light-emitting diodes (Rebel SP-12-L1, Luxeon Star LEDS, Lethbridge, Alberta, Canada). Reflected light from the subject’s face was collected at a distance of 28 cm ± 1 cm between the subject’s face and camera, using a 12-bit charge coupled device (CCD) camera (Pixelfly QE, PCO-Tech Inc., Romulus, Michigan, USA) and lens (8–48 mm Pentax TV Zoom Lens, Field of View 200 × 140 mm2, 1392 × 1024 pixel2, 140 um/px). Images were acquired at 4 Hz with an exposure time of 200 ms. Each imaging session ranged from 3 min to 9 min, depending on the experimental manipulation used (see protocols below).
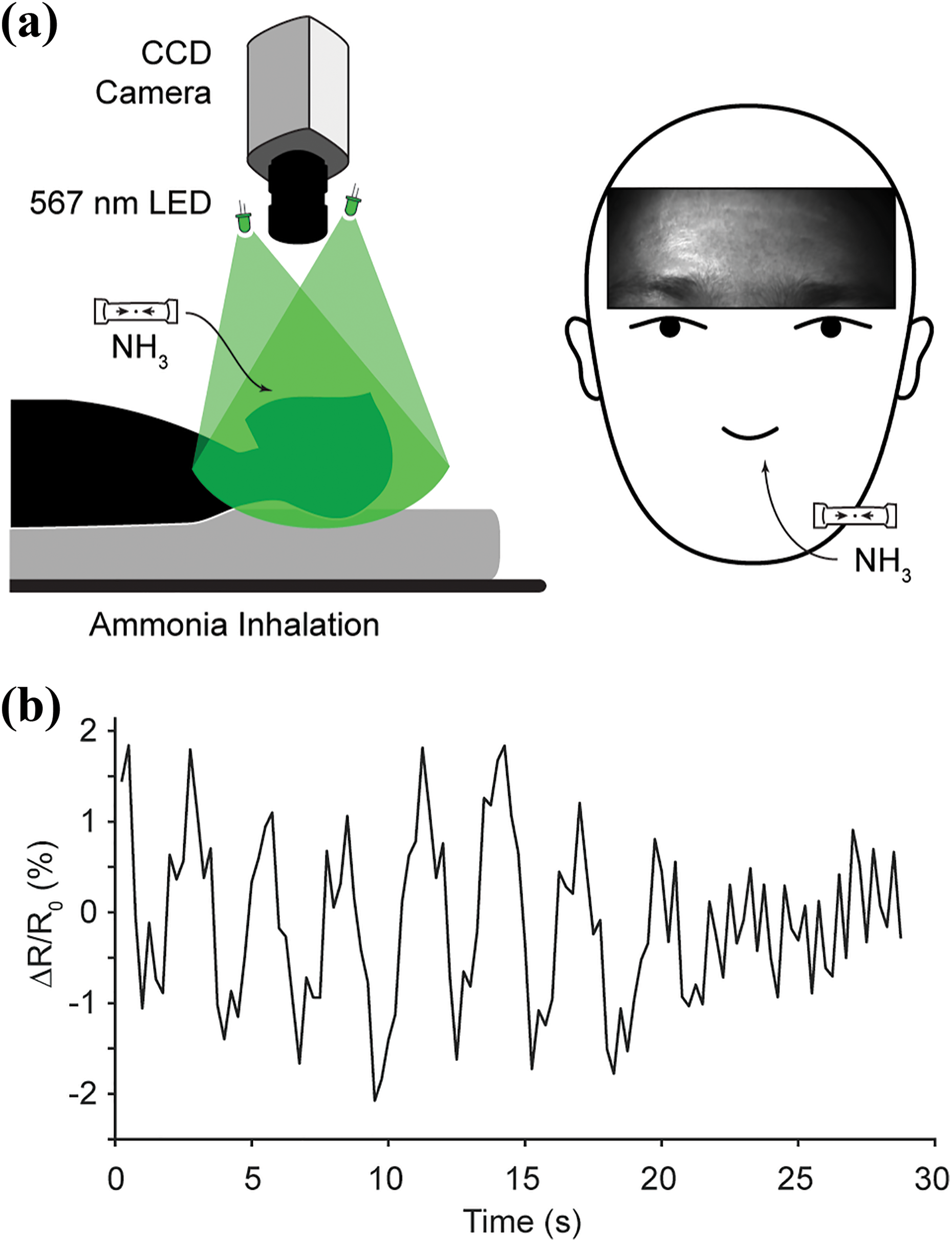
Experimental setup: (a) imaging setup and (b) a representative trace of the signal obtained via facial cutaneous imaging at rest.
In preliminary experiments, various LEDs emitting light at different wavelengths (488 nm, 567 nm, 617 nm, and white light) were tested for facial skin illumination. We found that the intensity of light reflected from the subject’s face was modulated in time at any of the tested wavelengths. However, the maximal amplitude in the frequency range of interest was achieved at a wavelength of 567 nm. Given this was also an isosbestic wavelength for hemoglobin absorption, 21,22 allowing interpretation of reflectance signal as representative of cutaneous blood volume, we proceeded with this wavelength. Illumination intensity (12,000 ± 2 K) was chosen so that the camera’s dynamic range was optimally used while avoiding pixel saturation.
Experiments were performed in a dark, quiet, temperature-controlled room (22–23°C). Each subject spent a minimum of 30 min in this environment prior to the experiment. All subjects underwent resting (supine) facial cutaneous imaging, after a minimum of 10 min of quiet supine rest. To minimize motion artifacts, a foam support for the subject’s head was used during imaging.
Ammonia inhalation testing
In addition to resting (baseline) facial imaging described above, a subset of subjects underwent facial imaging following ammonia inhalation (n = 42; age- and sex-matched groups of 17 migraine, 25 controls), see Figure 1(a). In this setting, participants were positioned under a CCD camera as outlined above with the right nostril occluded. After a 90-s baseline recording, ammonia vapor was inhaled until the subjective pain threshold was reached (1–2 s), and recording continued for an additional 90 s.
Autonomic reflex testing
Standardized cardiovagal and cardiovascular adrenergic function were tested using noninvasive continuous heart rate and beat-to-beat BP monitoring (BMEYE Nexfin, Amsterdam, the Netherlands) according to published methods. 25,26 Cardiovagal function was assessed using heart rate deep breathing (HRDB) and Valsalva ratio (VR). Cardiovascular adrenergic function was evaluated by measuring BP and heart rate (HR) responses to Valsalva. In brief, subjects were asked to perform deep breathing cycles and a Valsalva maneuver (VM) by way of forced exhalation using visual cues. For the HRDB, subjects were instructed to breathe at a rate of 6 breaths per minute (inspiratory and expiratory cycles of 5 s each; visual cue was an oscillating bar with a period of 10 s). Eight cycles are recorded. Following 2 min of rest, the procedure was repeated. The five largest consecutive responses were measured and averaged. For the VM, subjects were instructed to inhale deeply, subsequently exhaling through a bugle with an air leak (to ensure an open glottis) (WR Medical Electronics Co., Maplewood, Minnesota, USA) to maintain the manometer dial at an expiratory pressure of 40 mmHg for 15 s. Each test was followed by a rest period of 3 min, with testing repeated for two trials. For each test, the VR was calculated as the maximum HR generated during the maneuver, divided by the minimum HR occurring in the 30 s following the release of the maneuver. In the current study, the VR values were averaged for our analyses. Adrenergic score was calculated from BP measures produced during the VM according to published methods. 27 For resting vital sign testing, the subject’s BP and HR responses were measured via a continuous beat-to-beat BP device fixed to the right middle finger and three-lead EKG, respectively. Following a period of supine rest, no less than 20 min, baseline recordings were obtained for a minimum of 2 min (average of the measurements during these 2 min is reported). All recordings were collected using WR TestWorks™ software (WR Medical Electronics Co), exported as raw data and analyzed off-line.
Image acquisition and processing
All images were saved to a desktop computer in an uncompressed tiff-image format. Image processing was performed off-line using FIJI 28,29 and MATLAB (Version 2015b; Mathworks, Natick, Massachusetts, USA). Prior to analysis, respiratory-mediated and motion artifacts were further reduced by running all image series through a custom filter and the StackReg ImageJ plugin, 30 respectively. Once registered, regions of interest (ROI) over the right and left forehead were selected using the iris as an anatomical standard reference for size. All pixels within each ROI were averaged for each frame, resulting in a single time series for each ROI. Due to the lack of significant lateralization of signal, the two ROIs for each subject were averaged for further analyses. The fractional change from baseline, (R t − R o)/R o, of each image series was calculated using a custom ImageJ plugin, using the first nine frames as the baseline period. An example of these FCOs is shown in Figure 1(c). Time series data were then band-pass filtered between 0.02 Hz and 1 Hz, to isolate putatively autonomically driven low-frequency (LF) vascular oscillations. 31 –34
FCO frequency was determined by applying fast Fourier transform (FFT) to the signal to determine its power spectrum (method A) and identifying the dominant frequency component. Method A was confirmed manually by a single rater by visually determining the number of major oscillations during a set interval of time (method B). Method B frequencies were also confirmed by a second rater for a subset of 10 healthy control subjects (no significant difference between raters, p = 0.64).
Statistical methods
Data distributions were visually inspected and tested for normality using the Shapiro–Wilk test and found to be nonparametrically distributed, thus all measurement values are expressed as median and interquartile range (IQR). Pair-wise comparisons were made using the paired-sample Wilcoxon rank-sum test, while comparisons between study groups used the two-sample Wilcoxon rank-sum test; finally, Kruskal–Wallis rank-sum test was used to test for differences across >2 groups. Correlations were made using two-sided Spearman’s correlation. A Bland–Altman assessment for agreement was used to compare our two analysis techniques for FCO frequency calculation (methods A and B as described above). Results were considered significant for p-values<0.05, using two-tailed hypotheses. Statistical analyses were performed with R for Windows (Version 3.3.2; R Core Team, Vienna, Austria).
Results
Clinical characteristics
Subjects (65 total; 38 female, 27 male) aged 15–75 years were recruited into migraine (n = 22) and age- and sex-matched healthy controls (n = 43) groups. Initial recruitment included 80 subjects, though 3 were excluded due to early withdrawal from the study and the remaining 12 were excluded through the process of sex- and age-matching for migraine and control groups. Of the 22 migraine subjects (16 episodic migraine, 6 chronic migraine), there were 11 with aura and 11 without aura; headache predominated on the right side in 5, left side in 5, alternating right/left in 4, and nonlateralizing in 8. See Table 1 for a summary of basic clinical characteristics of the sample.
Clinical characteristics.a

F: female; IQR: interquartile range; M: male.
aTwo-sample Wilcoxon test, non-significant—years of age: p = 0.36. χ 2 test, non-significant—sex: p = 0.77.
Facial hemodynamic oscillations differ between healthy controls and migraineurs
The frequency of resting (supine) FCOs was significantly higher in migraine, compared to healthy controls (Figure 2; Table 2), where controls exhibited a median oscillation frequency of 0.137 (IQR 0.044) versus 0.162 (IQR 0.035) in migraineurs (two-sample Wilcoxon rank-sum test, p = 0.01). Resting facial oscillation amplitude did not differ between control and migraine groups (▵R/R 0 median 0.006, IQR 0.005 vs. 0.006, IQR 0.002; two-sample Wilcoxon rank-sum test, p = 0.50).

Resting (supine) facial cutaneous activity was significantly higher in migraine, compared to healthy controls (median 0.162, IQR 0.035 vs. 0.137, 0.044 respectively); two-sample Wilcoxon rank-sum test, p = 0.01. IQR: interquartile range.
Physiological data.
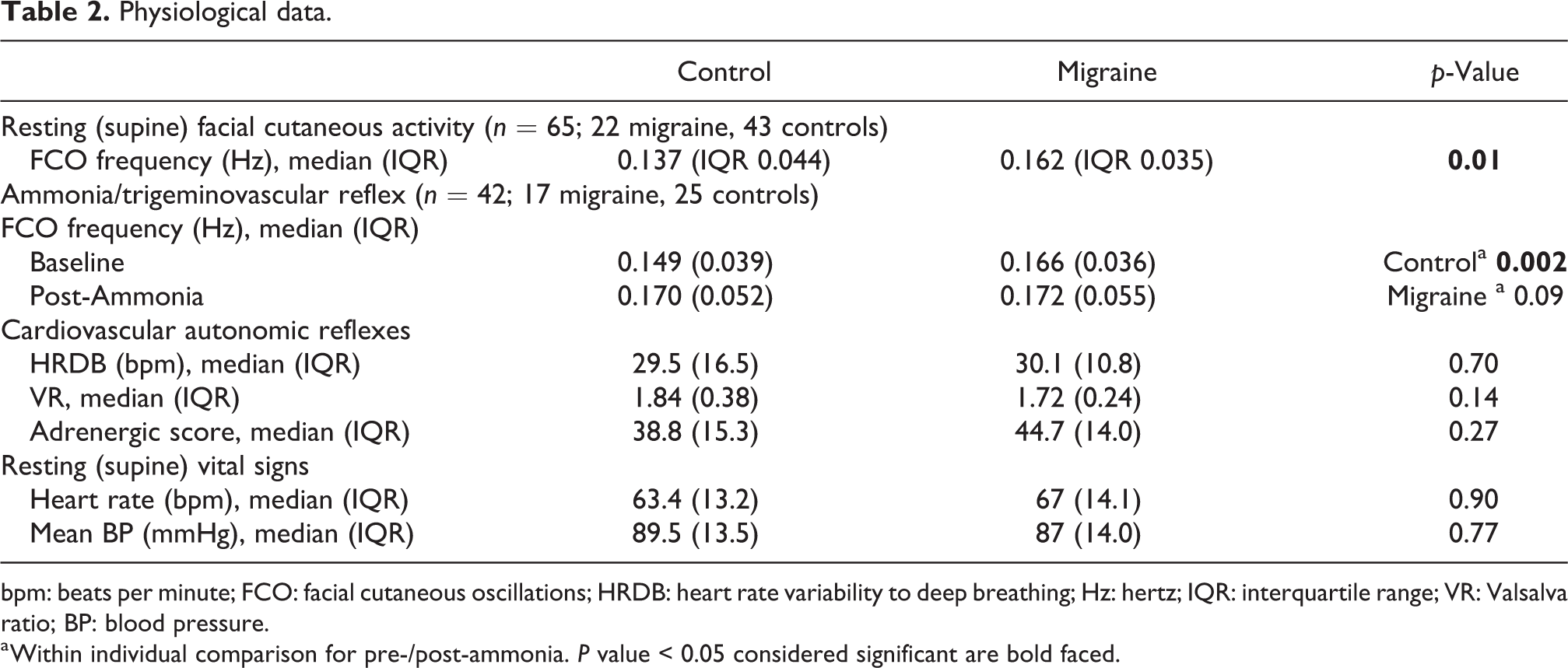
bpm: beats per minute; FCO: facial cutaneous oscillations; HRDB: heart rate variability to deep breathing; Hz: hertz; IQR: interquartile range; VR: Valsalva ratio; BP: blood pressure.
a Within individual comparison for pre-/post-ammonia. P value < 0.05 considered significant are bold faced.
Facial cutaneous activity after trigeminovascular reflex is altered in migraine
Of the subset of subjects (42 total; 26 female, 16 male) that completed the ammonia inhalation protocol, migraine (n = 17) and healthy control (n = 22) groups were again matched for age (18–75 years; p = 0.64) and sex (64% and 60% female, respectively; p = 0.61). Following ammonia inhalation, healthy controls showed a significant increase in facial cutaneous frequencies (median oscillation frequency 0.149 Hz, increased to 0.170 Hz; paired-sample Wilcoxon signed-rank test, p = 0.002), whereas the increase was not significant in the migraine group (median oscillation frequency 0.166–0.172 Hz; paired-sample Wilcoxon signed-rank test, p = 0.09) (Figure 3). There were no significant differences in the resting (pre-ammonia) or post-ammonia FCO frequencies among migraineurs with lateralizing (right or left), nonlateralizing, or alternating headaches (pre-ammonia, p = 0.65; post-ammonia, p = 0.69; Kruskal–Wallis rank-sum test across groups).
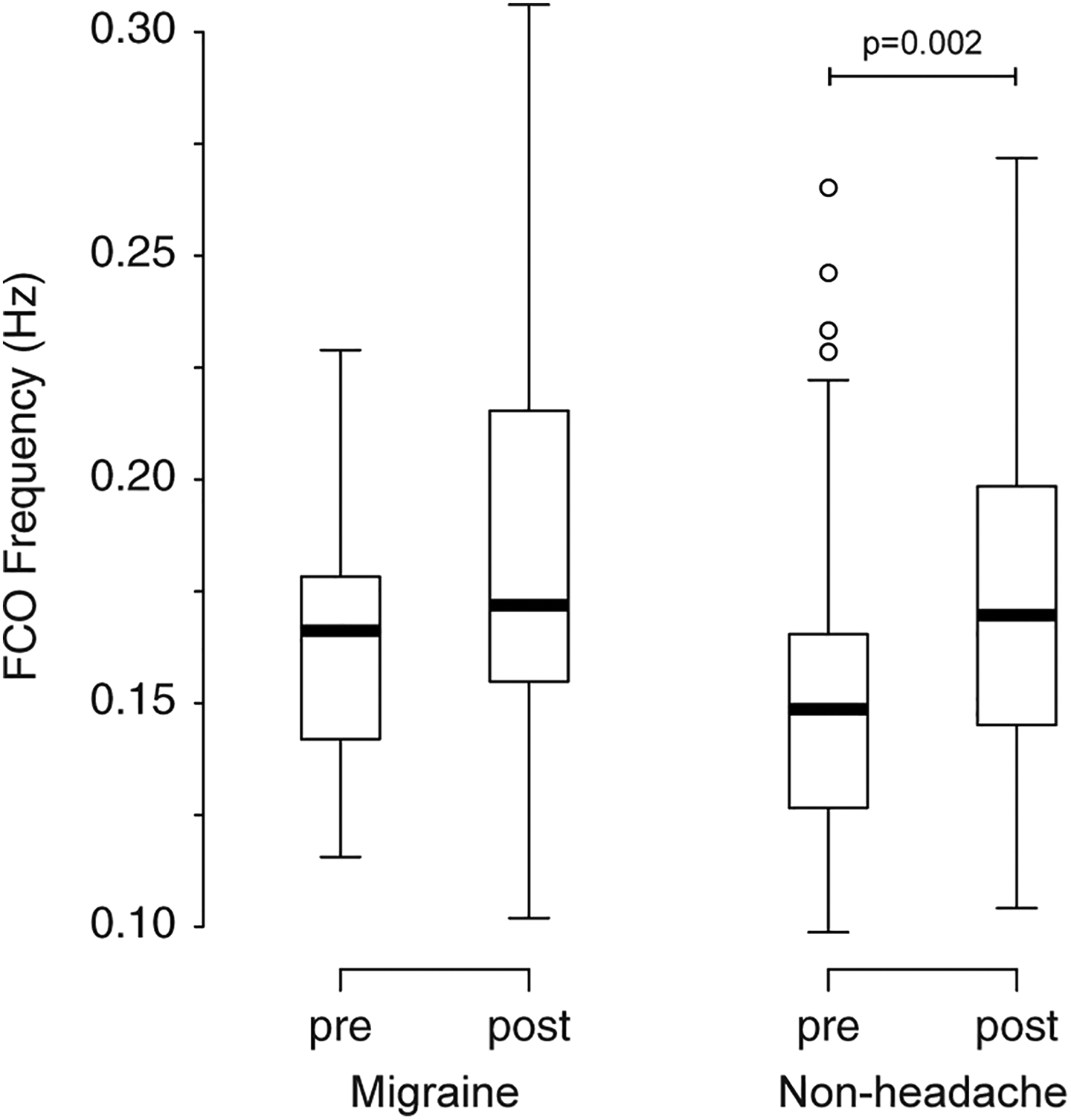
Control subjects showed a significant increase in facial cutaneous activity following ammonia inhalation (median oscillation frequency of 0.149–0.170; paired-sample Wilcoxon signed-rank test, p = 0.002), whereas this response was blunted in the migraine group (median oscillation frequency of 0.166–0.172; paired-sample Wilcoxon signed-rank test, p = 0.09).
Facial cutaneous activity appears to be independent of standardized cardiovascular autonomic or intracranial vascular measures
Standardized autonomic reflex parameters (HRDB and VM) and resting heart rate and BP did not differ significantly between the two study groups (Table 2). Resting FCO frequencies did not correlate with any of the standardized cardiovascular autonomic reflex parameters (HRDB, r = −0.30, p = 0.80; VR, r = −0.13, p = 0.64; adrenergic score, r = −0.30, p = 0.28), resting heart rate (r = −0.03, p = 0.90), or BP (r = 0.15, p = 0.58).
Reproducibility and repeatability
A Bland–Altman assessment for agreement was used to compare our two analysis techniques: method A (MATLAB FFT determined frequency) versus method B (manual frequency determination) (Figure 4); a range of agreement was defined as mean bias ±2 standard deviations. The Bland–Altman indicated that the 95% limits of agreement between the two methods ranged from −0.014 to 0.018, with a correlation coefficient of r = 0.95.

(a) Bland–Altman plot of method A (MATLAB FFT determined frequency) versus method B (manual frequency determination). The 95% limits of agreement between the two methods ranged from −0.014 to 0.018 (limits shown by upper and lower dotted lines; mean difference represented by the hashed line), with a correlation coefficient of r = 0.95 (b). FFT: fast Fourier transform.
Discussion
We present results of a novel assessment of craniofacial hemodynamic function, focusing on LF hemodynamic oscillations, 31 –34 which showed reproducibility between multiple assessments and consistency between manual and automated analysis techniques. Importantly, the frequency of resting facial cutaneous hemodynamic oscillations was different in migraineurs compared to healthy controls (Figures 2 and 3) providing proof of principle that this technique can be used in the investigation of craniovascular disorders. We also found that resting facial cutaneous activity can be significantly altered by ammonia inhalation, though this response was not significant in the migraine group (Figure 2). Additionally, there was no correlation between resting facial cutaneous activity and standardized cardiovascular autonomic reflex measures. Interestingly, these latter findings suggest a possible independent neural control for the local facial cutaneous hemodynamic activity studied here.
Approach to quantitative assessment and localization of hemodynamic oscillations
Autonomically driven spontaneous LF vasomotor oscillations have been observed with multiple single-point techniques, from transcranial Doppler to LDF and photoplethysmography. 31,35 –37 Power spectral frequency analysis of such oscillations in heart rate and BP is a widely used approach to the study of cardiovascular autonomic control. 32,38 –40 Such studies, paired with pharmacological and physiological perturbations, have led to the proposal of LF (0.04–0.15 Hz) and high-frequency (HF; 0.15–0.4 Hz) bands where the HF peak is accepted to reflect cardiovagal (parasympathetic) nerve activity and the LF peak is often assumed to represent sympathetically dominant nerve activity. 31 –34 In this paradigm, baroreflex-mediated BP and heart rate changes exhibit LF predominant control, whereas resting state and heart rate variability driven by deep breathing exhibit HF predominate control. 35,39 It is worth noting that interpretation of the LF frequency band is not straightforward and likely reflects a complex mix of distinct sources of sympathetic (e.g. baroreceptor, thermoregulatory vasomotor) activity, as well as parasympathetic and other unidentified factors. 41 –43 Interestingly, there was no correlation between standardized cardiovascular autonomic reflex measures and resting facial cutaneous activity. This preliminarily supports the possibility of differing neurogenic mechanisms for craniofacial- versus cardiovascular-based hemodynamic oscillations, though follow-up studies are needed to further examine the coherence of facial cutaneous activity and generalized cardiovascular signals, as well as cross-correlation of these signals during baroreflex and other evocative maneuvers.
Using the proposed LF and HF localizations to interpret our findings is tempting, as our results appear to agree with an increase in facial parasympathetic activity following ammonia inhalation (a shift toward higher frequencies with trigeminovascular reflex activation). Additionally, we find that the resting state FCOs in migraine subjects are significantly higher, in the HF range, compared to healthy controls. However, we did not detect significant relationships between facial cutaneous activity and systemically controlled cardiovagal parasympathetic (HRDB, VR) measures. Prior studies focusing on cutaneous vascular responses to heat (thermoregulatory vasomotor activity) have suggested that facial skin, but not forearm, can overcome sensory blockade through local axon reflex vasodilation. 44 This could explain in part, why our study does not find significant relationships between systemic cardiovascular and intracranial vascular responses. It is also quite possible that sympathetic and parasympathetic vasomotor responses are operant in craniofacial oscillations, but that their control is differentially localized from that of systemic vasculature.
Trigeminally mediated parasympathetic vasodilation of forehead vasculature is classically attributed to parasympathetic vasomotor fibers distributed by the facial nerve. 45 –47 Blood vessels in this region have been observed to have a distinctive 0.15 Hz rhythm, which has been localized to brainstem activity in an animal model and human work, and can be augmented by relaxation and paced breathing, suggesting a basal level contribution cardiorespiratory parasympathetic input. 48,49 Drummond examined seven patients with facial nerve lesions and evaluated their facial vascular activity in the 0.15 Hz range before and after noxious ocular stimuli (Schirmer’s test). 12,50 This work suggested an effective “masking” effect of facial nerve-mediated parasympathetic activity over resting state 0.15 Hz vascular activity, supporting the likelihood of multiple generators for this signal, apart from cardiovascular-respiratory phase coupling. In our study, the apparent blunting of ammonia response in the migraine group (Figure 2) could potentially be generated by a ceiling effect, mediated by facial nerve relayed parasympathetic activity, and leading to a higher resting (baseline) FCO frequency. Such a higher “set point” for resting activity could potentially inhibit reflex-mediated variance of facial cutaneous activity and lead to spurious conclusion for this study group. Follow-up studies utilizing coherence analysis with other previously validated tests of trigeminovascular and sympathetic/parasympathetic function could provide additional insight into this possibility.
In the present study, we found no significant differences in sympathetic (adrenergic score) or parasympathetically (HRDB, VR) mediated autonomic reflexes between migraine and healthy control subjects (Table 2). These findings are in agreement with prior reports, where standardized cardiovascular autonomic reflexes do not significantly differ between migraineurs and controls, 51 –53 though these groups have also reported varying differences in responses to sustained hand-grip and phase analysis of BP changes during Valsalva. 52,53 In our study, we intentionally elected to focus on the most sensitive, best standardized, and least effort-dependent sympathetic and parasympathetic cardiovascular autonomic measures 54 in order to reduce spurious group differences based on technique. Furthermore, we chose to minimize the number of parameters compared (focusing again on the best standardized measures) in order to reduce the potential pitfalls underlying studies using multiple comparisons (>10 variables tested in the studies cited). The consistent lack of a difference in systemic autonomic reflexes in multiple studies, and evidence of altered craniofacial autonomic response, underlines the possibility of separate autonomic regulation of this region.
Application to craniovascular diseases such as migraine
The trigeminovascular reflex is characterized by craniofacial vasodilatory and secretory responses evoked by a painful stimulation to facial structures, which is thought to be due to a combination of trigeminal-evoked changes and autonomic outflow. 45,47 In this study, we applied inhaled ammonia vapor to evoke a trigeminovascular response 55 and measured the facial cutaneous vascular response through changes in hemodynamic oscillation frequency. Prior studies examining normal and interictal migraine patients have shown an augmentation of bilateral forehead pulsatility in response to painful cutaneous or mucosal facial stimulation, 47,56 and still others have focused on migraine lateralization relative to facial blood flow pulsatility. 11,17 Such studies have focused on an alternate characteristic of craniofacial hemodynamic control, namely, blood flow via pulsatility at heart rate frequencies and spatial aspects of perfusion pulse waves. Our technique explicitly examines oscillations in blood volume, rather than pulsatile flow. Thus, we do not find such results necessarily contradictory to our findings, but simply reflective of differing aspects of facial perfusion. The answer to this difference may lie in the differing baseline (resting) facial cutaneous activity, where migraine subjects demonstrate a higher set point in FCOs compared to control subjects (Figure 2), possibly related to a relative interictal sympathetic deficit 2,57 or relative peri-ictal parasympathetic hyperfunction 58 (though our analysis does not account for time since the last attack, nor time till next attack). Following ammonia inhalation, we see a relatively blunted change in FCO frequency in the migraine group, compared to healthy control subjects (Figure 3). Here we hypothesize that our technique is measuring an element of facial cutaneous vascular control that is independent of blood flow pulsatility (otherwise shown to be increased in migraineurs 47,56 ) and perhaps reflective of local, extracranial neural control, as discussed above, that is statically altered in a relative state of increased parasympathetic (or decreased sympathetic) tone 2,57,58 in interictal migraineurs.
As noted in the prior section, previously published approaches to facial cutaneous pulsatility have suggested differences in unilateral migraineurs. 11,17 Avnon et al. showed that migraineurs with unilateral migraine tended to have the smallest amount of vasodilation with painful stimuli, whereas bilateral migraineurs had the largest amount of vasodilation. 11 While the present study was not powered to detect differences between right and left unilateral migraineurs, nor between those with lateralizing and nonlateralizing migraines, our results do not suggest a significant difference in FCO frequencies between these migraine subgroups.
Limitations
Although we made efforts to match age and sex between control and migraine groups, the severity of migraine and frequency of attacks varied widely across our migraine group, and aura was perhaps over-represented compared to the expected frequency in the migraine population (32% aura is expected in both males and females). 59 While migraine subjects were studied during a headache-free period, the timing between the previous and next attack was not analyzed. Since it is plausible that time since the last headache, and/or migraine with or without aura could influence a migraineur’s facial cutaneous activity, evaluation of our findings in a larger migraine sample, both during and outside a migraine attack, could be useful.
Conclusions
We present a novel, noninvasive assessment of craniofacial hemodynamic function and validate our approach as a reproducible and consistent technique for the assessment of facial cutaneous hemodynamic activity. We propose this approach as a promising, novel biomarker of craniofacial vascular function that may be independent of mechanisms studied by other techniques and which holds promise for providing additional understanding of craniofacial vascular processes in migraine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.