
Abstract
Objectives:
This study aimed to report the clinical profiles of patients with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT)/short-lasting unilateral neuralgiform headache attacks with cranial autonomic (SUNA) in a Japanese population by surveying those enrolled at a regional headache center in Japan.
Methods:
In this consecutive case series study, the clinical characteristics of patients with SUNCT (eight men, three women; mean age: 59.5 ± 20.5 years) and SUNA (five men, four women; mean age: 51.3 ± 18.4 years) who visited Tominaga Hospital from February 2011 to January 2017 were examined. Headaches were diagnosed according to the International Classification of Headache Disorders, Third edition (ICHD-3) guidelines.
Results:
Brief clusters of separate attacks were reported by all patients. The mean duration of attacks was 91.9 ± 87.9 s. Ipsilateral rhinorrhea was observed in 9 of 20 (45.0%) cases and facial sweating was observed in 1 of 20 (5.0%) cases. An eminent response to lamotrigine was observed in 9 of 9 (100%) patients; however, adverse events were only reported in 2 of 9 (22.2%) cases. An intravenous infusion of lidocaine was demonstrated to be completely successful for short-term prevention in 5 of 6 (83.3%) SUNCT cases.
Conclusions:
Lamotrigine can successfully treat most patients, and intravenous lidocaine is useful for the short-term preventive therapy of severe recalcitrant attacks in Japanese patients with SUNCT/SUNA.
Introduction
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) is classified as trigeminal autonomic cephalalgias (TACs) in the International Classification of Headache Disorders, Third edition (ICHD-3). 1 SUNCT is defined as the occurrence of at least 20 attacks of moderate or severe unilateral pain with an orbital, supraorbital, temporal, or trigeminal distribution, lasting 1–600 s. 1 When autonomic symptoms include only one or neither of these ocular symptoms, they are referred to as short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA). 1 Previously, it was unknown whether SUNCT or SUNA are clinical phenotypes of the same syndrome or whether SUNCT is a subset of SUNA. 1 –3 This is primarily because magnetic resonance imaging (MRI) revealed an incidence of neurovascular compression in patients with SUNCT/SUNA, which was also identified in classical trigeminal neuralgia. 2,3 However, recent studies have confirmed that SUNCT and SUNA should be considered as clinical phenotypes of the same syndrome with MRI as the diagnostic technique for identifying SUNCT/SUNA. 4 Both SUNCT and SUNA are recognized within the TACs grouping based on the clinical profiles and the associated symptoms.
Trigeminal neuralgia (TN) is a disorder that is classified based on painful cranial neuropathies and other facial pains. 5 TN, SUNCT, and SUNA are categorized as different disorders, and hence they have been grouped into discrete components of the ICHD-3. 1 However, the relationship among TN, SUNCT, and SUNA continues to be debatable because studies have indicated the presence of therapeutic, radiological, and clinical overlap among these disorders. 6 The present findings indicate a broader association among TN, SUNCT, and SUNA. 5 Further research is required to determine the relationship among TN, SUNCT, and SUNA considering their effects on clinical practice and existing therapies.
Most of the previous reports on SUNCT and SUNA involved Caucasian populations, and the studies reporting the characterization of SUNCT/SUNA in Asian patients are limited. Thus, this study aimed to identify the clinical profiles of patients with SUNCT/SUNA in a Japanese population by surveying those enrolled at a regional headache center in Japan.
Methods
Subjects
This was a consecutive case series that studied the clinical characteristics of 20 patients diagnosed with SUNCT or SUNA. The study assessed 11 patients with SUNCT (eight men and three women; mean age: 59.5 ± 20.5 years) and nine patients with SUNA (five men and four women; mean age: 51.3 ± 18.4 years) who visited Tominga Hospital, a tertiary headache center in Japan, from February 2011 to January 2017. The diagnosis of headache was confirmed according to the ICHD-3 structured questionnaires, following complete neurological examinations and appropriate tests. The questionnaire used in this study has been added as Supplementary Material 1. To exclude the presence of symptomatic SUNCT/SUNA, MRI was performed in 19 patients, and computed tomography (CT) was performed in 1 patient because of cardiac pacemaker insertion. For evaluation of neurovascular compression (NVC), MRI constructive interference in steady state (CISS) was performed in 19 patients. Approval for the examination was provided by the institutional ethics committee of Tominaga Hospital (Approval number: 120064), and informed consent was obtained from all participants.
Clinical data collection
Data were collected for categories, such as age at onset, sex, laterality, duration and frequency, cranial autonomic features, presence or absence of migraine-like conditions (nausea, vomiting, photophobia, and phonophobia), previous diagnostic details including duration and frequency, prevalence of possible triggering factors, incidence of other TACs, presence or absence of a refractory period, smoking history, and alcohol consumption along with medication received. The response rate to medication was documented using a four-point scale by Williams and Broadley. 3
Ethical approval
The study obtained appropriate approval from Tominaga Hospital Ethics Committee, approval number: 120064. Informed consent was obtained from participants.
Results
Demographic characteristics
The demographic characteristics of the study participants are shown in Table 1, including the mean age of patients, age of onset, and the other categories for which data were collected.
Demographics of study patients with SUNCT/SUNA.
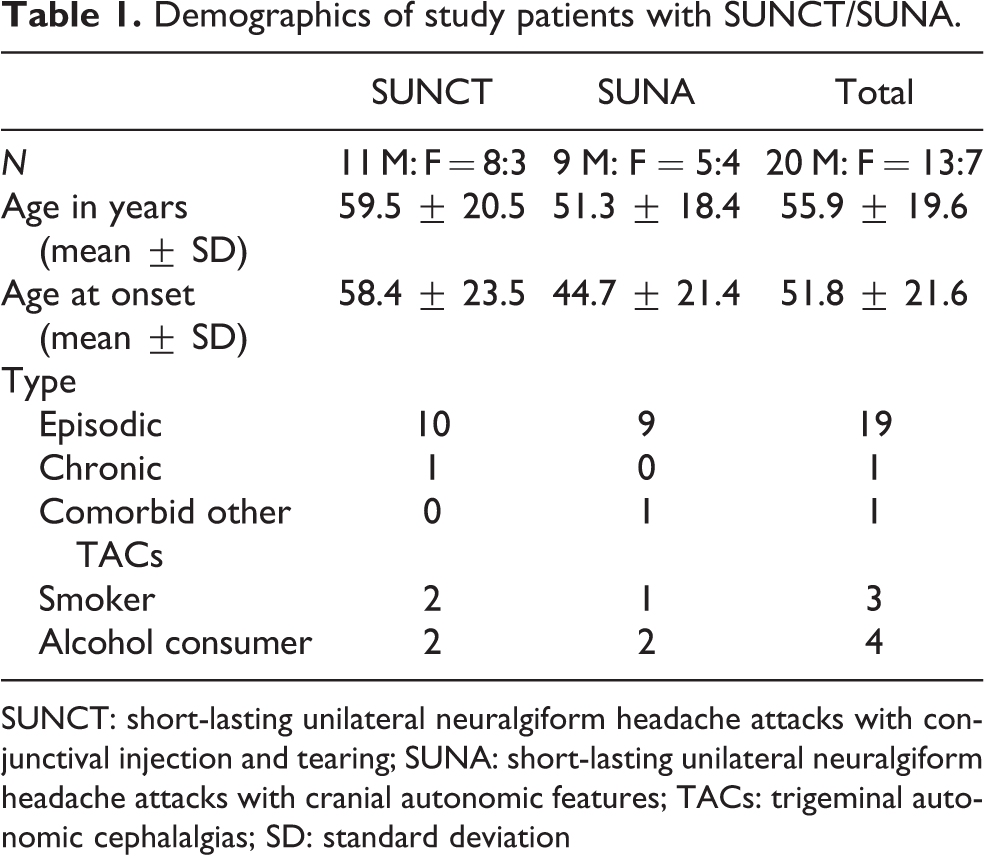
SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic features; TACs: trigeminal autonomic cephalalgias; SD: standard deviation
All the patients who participated in our study were diagnosed with SUNCT or SUNA previously at other clinics. Following the diagnosis, they were referred to our clinic for further treatment. The records from the previous clinics indicated that seven patients were diagnosed with TN: three of them had cluster headache, two were diagnosed with migraine during a previous visit at a hospital or clinic (Table 2), and two patients were previously diagnosed with SUNCT (Table 2).
Clinical data from previous diagnosis.

SUNCT: Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic features.
Clinical characteristics of patients with SUNCT and SUNA
The clinical characteristics of patients with SUNCT and SUNA are provided in Tables 3 and 4. The attacks were right sided in 13 patients and left sided in 7; a bilateral or side-shifting attack was not reported in any of the patients. Attacks were either brief clusters of separate attacks or a saw-tooth pattern in all patients. A chronic course was reported in 1 of 20 (5.0%) cases, whereas an episodic disease course was evident in 19 of 20 (95.0%) cases. The mean duration of attack was 91.9 ± 87.9 s: <30 s in 6 of 20 (30.0%) cases, approximately 60 s in 5 of 20 (25.0%), approximately 120 s in 3 of 20 (15.0%), and >120 s in 6 of 20 (30.0%; Tables 3 and 4). In SUNCT, ipsilateral conjunctival injection and lacrimation were observed in all cases (Table 3). In SUNA, conjunctival injection was observed in 1 of 9 (11.1%) cases, and lacrimation was observed in 8 of 9 (88.9%) cases (Table 4). Ipsilateral rhinorrhea was observed in 9 of 20 (45.0%) cases and facial sweating was observed in 1 of 20 (5.0%) cases (Tables 3 and 4). Photophobia was observed in 1 of 20 (5.0%) cases, and phonophobia was observed in 5 of 20 (25.0%) cases (Tables 3 and 4). All migrainous features were bilateral. In total, 3 of 20 (15.0%) patients were smokers and 4 of 20 (20.0%; Table 1) consumed alcohol. A refractory period was observed in two patients (cases 4 and 6) but not in 18 patients.
Clinical presentation of SUNCT cases.
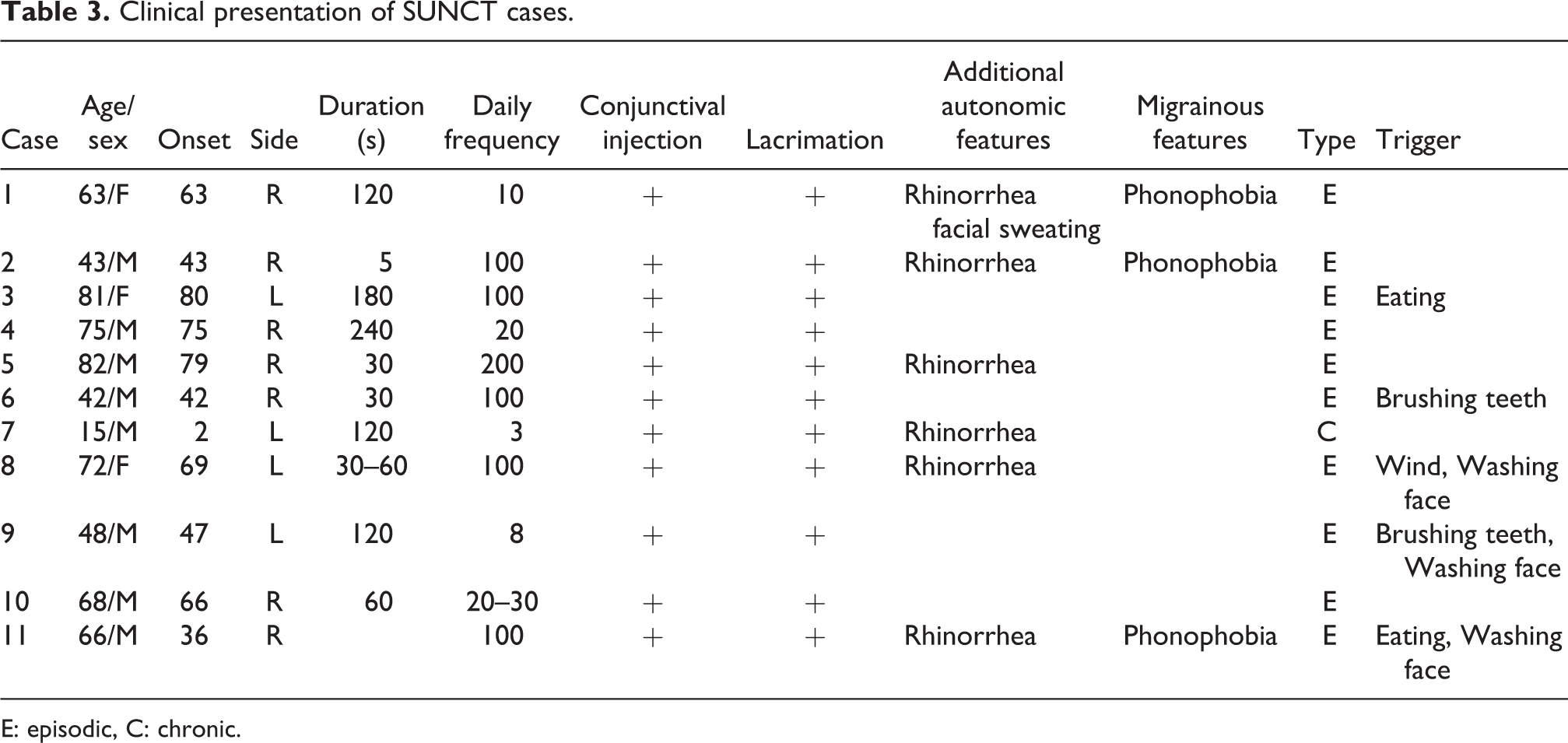
E: episodic, C: chronic.
Clinical presentation of SUNA cases.

E: episodic; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic.
Treatment of the patients with SUNCT and SUNA
An eminent response to lamotrigine was observed in 9 of 9 (100%) cases at doses of 100–250 mg/day; however, toxic eruption was also observed in 2 of 9 (22.2%) cases. One patient (case 18) improved following discontinuation of lamotrigine, but another patient (case 6) experienced complications of Stevens–Johnson syndrome and improved with steroid pulse therapy. Gabapentin was effective in 4 of 5 (80.0%) cases at doses of 600–1800 mg/day, pregabalin (150–450 mg/day) in 3 of 10 (30.0%), carbamazepine (200–400 mg/day) in 2 of 4 (50.0%), and topiramate (50–200 mg/day) in 2 of 3 (66.7%). An intravenous infusion of lidocaine (1–2 µg/kg/min) was proven to be completely efficacious for a short-term preventive therapy in 5 of 6 (83.3%) patients with SUNCT. However, poor response to lidocaine treatment was observed in chronic SUNCT cases. Indomethacin (75 mg/day) was not effective in 6 of 7 (85.7%) cases. Only one patient (case 17) showed a good response to indomethacin. She had two types of periorbital headaches with lacrimation. Type 1 headache lasted for approximately 10 minutes (20 times/day), and type 2 headache lasted for approximately 300 s (5–10 times/day). Type 1 headache considered to be paroxysmal hemicrania disappeared following indomethacin administration, and type 2 headache, considered to be SUNA, decreased. Type 2 headache disappeared following lamotrigine (100 mg/day) administration. Although the underlying mechanism is unknown, partial indomethacin reactivity could exist for SUNA in this case. In the Japanese insurance medical care system, since the maximum dose of indomethacin is 75 mg/day, we cannot administer the recommended dose (150 mg/day) for the initial treatment of paroxysmal hemicrania and hemicrania continua in ICHD-3. The detailed treatment results are provided in Tables 5 and 6.
Treatment performed in SUNCT cases.

LTG: lamotrigine; GBP: gabapentin; PGB: pregabalin; CBZ: carbamazepine; MPL: methyl-prednisolone; SC: subcutaneous injection; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic.
Treatment performed in SUNA cases.

LTG: lamotrigine, GBP: gabapentin, PGB: pregabalin, CBZ: carbamazepine, MPL: methyl-prednisolone, SC: subcutaneous injection; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic.
SUNCT/SUNA cases with trigeminal NVC
MRI or CT did not reveal structural abnormalities in any of the cases. In 11 cases (5/11 (45.4%) of SUNCT and 6/9 (66.7%) of SUNA), MRI revealed ipsilateral trigeminal NVC. Five cases with NVC (4 SUNCT and 1 SUNA) had TN before SUNCT/SUNA occurrence (Table 7). TN was not observed in cases without NVC. In some SUNCT/SUNA cases, the cause of the disease was NVC. The refractory period was observed in 2 SUNCT cases (cases 4 and 6) with NVC. In one SUNCT case (case 6) with ipsilateral trigeminal NVC, the treatment administered was microvascular decompression, and the pain was relieved postoperatively. The clinical course of this case is presented in Figure 1. The patient was diagnosed with SUNCT based on ICHD-3. The patient was successfully treated with continuous intravenous administration of lidocaine and oral lamotrigine. In this patient, the dose of lamotrigine was gradually increased from 50 mg/day to 200 mg/day. The patient experienced complications of Stevens–Johnson syndrome and improved with steroid pulse therapy. Lamotrigine was changed to topiramate (50 mg/day).
SUNCT/SUNA cases with trigeminal NVC.
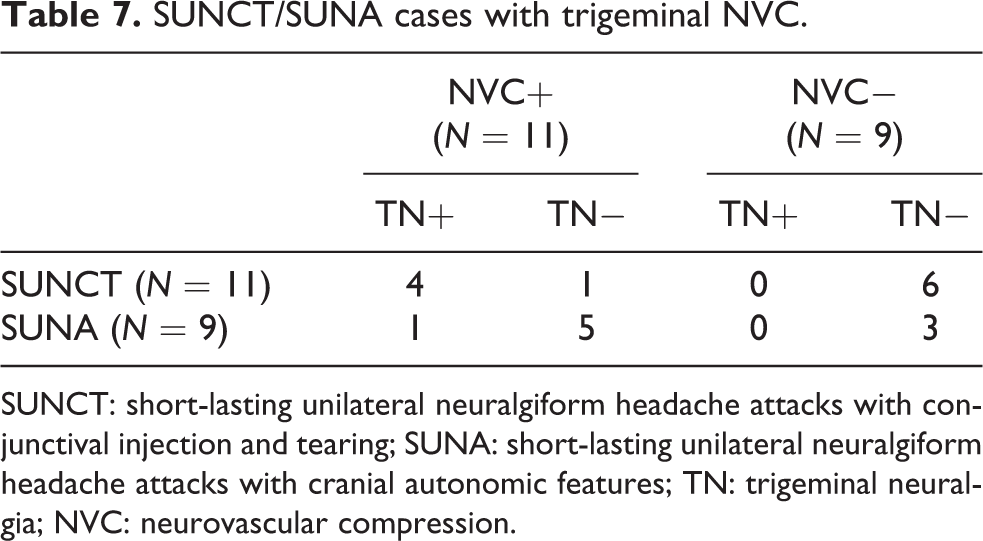
SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic features; TN: trigeminal neuralgia; NVC: neurovascular compression.

Clinical course of case 6 (SUNCT). SJS: Stevens–Johnson syndrome; SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing.
The headache recurred approximately half a year later. The patient then underwent an operation for microvascular decompression. The pain was relieved postoperatively and has not relapsed in the last 3 years since the operation.
Discussion
In this study, we have reported the clinical profiles of 20 Japanese patients with SUNCT/SUNA. Although previous studies on clinical profiles with SUNCT/SUNA have been reported, 7,8 to the best of our knowledge, this is the first study to report the clinical outcomes in patients with SUNCT/SUNA in a Japanese population. The findings from this study showed the presence of an eminent response to lamotrigine in the sample population, although adverse events were also observed. The results also indicated that an intravenous infusion of lidocaine was completely efficacious for a short-term preventive therapy in SUNCT cases and that Japanese patients show a low prevalence of chronic SUNCT/SUNA (5%). Low prevalence of chronic cluster headache has been previously reported in the Japanese and Taiwanese population. 9,10 The findings from our study are consistent with those from other previous studies that have shown lamotrigine and lidocaine as useful therapeutic agents for SUNCT/SUNA. 8,11 The results also indicated that similar to studies on the Caucasian population, lamotrigine can be used for treating patients with SUNCT/SUNA and an intravenous infusion of lidocaine is useful for treating severe recalcitrant attacks in Japanese patients with SUNCT/SUNA. Importantly, our study showed that microvascular decompression should be considered during the treatment of refractory SUNCT/SUNA as NVC might be prevalent is some cases.
One of the limitations of our study is the small sample size with only 20 patients included in the analysis. Nevertheless, our study indicated that some SUNCT/SUNA cases could be caused by NVC. Hence, the clinical outcomes from our findings support a broader classification of SUNCT/SUNA and TN disorders. Further research is required to gain more insights into this classification.
Clinical implications
Intravenous lidocaine is useful as a short-term preventive therapy for Japanese SUNCT/SUNA patients. Lamotrigine is effective in treatment for Japanese SUNCT/SUNA patients.
Supplemental material
Supplementary_file - Clinical profile of SUNCT/SUNA in Japan: A clinic-based study
Supplementary_file for Clinical profile of SUNCT/SUNA in Japan: A clinic-based study by Shoji Kikui, Junichi Miyahara, Hanako Sugiyama, Kentaro Yamakawa, Yoshihiro Kashiwaya, Kumiko Ishizaki, Daisuke Danno, and Takao Takeshima in Cephalalgia Reports
Footnotes
Acknowledgements
Editorial support, in the form of medical writing, assembling tables and creating high-resolution images based on authors’ detailed directions, collating author comments, copyediting, fact checking, and referencing, was provided by Editage, Cactus Communications.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.