
Abstract
Background
Aromatase inhibitor–induced arthralgia (AIA) is a frequent adverse effect of endocrine therapy in breast cancer survivors, often leading to treatment modification or discontinuation. Non-pharmacological interventions have been proposed to manage AIA, but evidence remains fragmented.
Objective
To synthesize recent randomized controlled trials (RCTs) evaluating the efficacy of non-pharmacological interventions for AIA.
Methods
A systematic search of PubMed, Scopus, and Web of Science identified RCTs published between 2010 and 2025 assessing non-pharmacological strategies for AIA. Two reviewers independently performed study selection, data extraction, and quality appraisal using standardized criteria.
Results
Eight RCTs met inclusion criteria, encompassing interventions such as acupuncture, structured exercise (aerobic, resistance, and Pilates), progressive relaxation, and neuromuscular taping. Acupuncture produced clinically meaningful reductions in pain intensity (mean differences 0.9-1.1 points on the Brief Pain Inventory), while exercise programs yielded moderate improvements in pain, function, and quality of life. Relaxation and taping interventions demonstrated smaller or less consistent effects. No eligible trials evaluated occupational therapy-based interventions.
Conclusions
Acupuncture and structured exercise show the strongest evidence of benefit for managing AIA, though overall methodological quality remains moderate. Further well-designed trals with standardized outcomes and longer follow-up are needed to guide clinical implementation and to explore underrepresented approaches such as occupational therapy.
Introduction
Breast cancer (BC) is the most prevalent malignant neoplasm among women worldwide. 1 In 2022, approximately 2.3 million new cases were diagnosed globally, with a prevalence in Europe of 28%. 2 In Spain, the estimated incidence for 2025 is 37 682 new cases. Tumor cells in BC may express hormone receptors for estrogen (ER), progesterone (PR), and human epidermal growth factor receptor 2 (HER2), which de-termine molecular subtypes: luminal A (ER+, PR ≥ 20%, HER2−), luminal B (ER+, PR < 20%, HER2±), triple-negative (ER−, PR−, HER2−), and HER2-enriched (ER−, PR−, HER2+). Approximately 75%–80% of BCs are luminal subtypes that express ER. 3
Over recent decades, major advances in BC treatment have led to significant increases in survival rates. 4 Hormone therapy plays a central role in reducing recur-rence risk and improving prognosis for patients with hormone receptor-positive BC, as recommended by the St. Gallen International Breast Cancer Conference. 5 Commonly used hormone therapies include tamoxifen and aromatase inhibitors (AIs), such as letrozole, anastrozole, and exemestane.6,7 Tamoxifen blocks ERs on tumor cells, preventing hormone-driven growth, while AIs inhibit estrogen synthesis by blocking the aromatase enzyme. 8
Despite their efficacy, AIs are frequently associated with musculoskeletal side effects, particularly arthralgia, 9 which is defined as joint pain and is often localized in the hands. This condition leads to stiffness, reduced mobility, impaired physical function, and negatively affects quality of life, sometimes compromising adherence to oncologic treatment. Reported prevalence estimates range from approximately 20% to 74%, 10 with a substantial proportion of patients experiencing moderate-to-severe joint symptoms that interfere with daily activities.11–13 Hand and wrist joints are among the most commonly affected anatomical regions, contributing directly to functional limitations in grip strength, fine motor tasks, and activities of daily living. 14 Importantly, Aromatase inhibitor–induced arthralgia (AIA) is a leading cause of poor adherence, dose reduction, or early discontinuation of endocrine therapy, with estimates that around 11% of patients stop or modify treatment because of joint pain.15–17 These adherence problems are clinically relevant, as premature discontinuation of hormonal therapy has been associated with worse oncological outcomes. 18 Pharmacological management of hormone therapy–induced arthralgia usually includes analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), short treatment interruptions, or switching between different endocrine therapy agents (eg, from one aromatase inhibitor to another or from an aromatase inhibitor to tamoxifen). However, these strategies often provide only partial and transient symptom relief, and dose modification or treatment change may raise concerns about oncologic efficacy and long-term outcomes.19,20 In this context, non-pharmacological approaches have to be considered in the light of their favorable safety profile, the fact that they are are compatible with prolonged endocrine therapy, and can simultaneously target pain, physical function, and health-related quality of life. 21
Several non-pharmacological strategies have been proposed to address AI-induced arthralgia, including therapeutic exercise, manual therapy, hydrotherapy, yoga, splint-ing, and occupational therapy. 22 These interventions form part of a multimodal care approach aimed at improving patients’ physical function and overall well-being while promoting adherence to cancer therapy. 14
Given the clinical relevance of this adverse effect and the growing interest in supportive care strategies, this systematic review aims to synthesize the current evidence on the effectiveness of non-pharmacological interventions for managing hand arthralgia secondary to hormone therapy in BC patients.
Materials and Methods
Study Design
A qualitative systematic review was conducted in accordance with the PRISMA 2020 guidelines. 23 The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) CRD42025641398.
Search Strategy
A comprehensive literature search was performed in PubMed, the Cochrane Cen-tral Register of Controlled Trials (CENTRAL), and CINAHL databases. Two reviewers (N.M.-B. and V.A.-E.) independently conducted the search between January and Feb-ruary 2025. Discrepancies were resolved through discussion with a third reviewer (V.A.-P.).The search covered studies published between January 2010 and February 2025. This timeframe was selected because research on aromatase inhibitor–induced arthralgia and its supportive care strategies underwent major developments after 2010. Earlier literature frequently used heterogeneous terminology, non-standardized outcome measures, and older endocrine therapy regimens, reducing comparability with contemporary trials. In addition, current recommendations for managing AI-related musculoskeletal symptoms were largely established after the early 2010s, making recent studies more reflective of modern clinical practice.
Medical Subject Headings (MeSH) and free-text terms were used, including: “arthral-gia”, “breast neoplasms”, “aromatase inhibitors”, “tamoxifen”, “occupational therapy”, “rehabilitation”, “joint pain”, “hand arthralgia”, “breast cancer”, “hormonal therapy”, “hormonal treatment”, “endocrine therapy”, “hand therapy”, “physical therapy”, and “non-pharmacological interventions”. Boolean operators AND and OR were applied to construct the following search string:
(“arthralgia” OR “joint pain” OR “hand arthralgia”) AND (“breast neoplasms” OR “breast cancer”) AND (“hormonal therapy” OR “hormonal treatment” OR “endocrine therapy” OR “aromatase inhibitors” OR “tamoxifen”) AND (“occupational therapy” OR therapy OR “hand therapy” OR “physical therapy” OR “non pharmacological interventions” OR “rehabilitation”).
Eligibility Criteria
Inclusion criteria were defined using the PICOS framework: 24
Population: Adults (≥18 years) diagnosed with breast cancer and experiencing hormone therapy-induced hand arthralgia.
Intervention: Non-pharmacological rehabilitative interventions. Non-pharmacological interventions were defined according to the Cochrane Rehabilitation and Cochrane Complementary Medicine frameworks as structured therapeutic strategies delivered without pharmacological agents and intended to reduce symptoms, improve physical function, or enhance quality of life. 25 Eligible interventions included: acupuncture or related needle-based techniques, structured exercise programs (eg, aerobic exercise, resistance training, Pilates), relaxation or mind–body approaches (eg, progressive muscle relaxation), and neuromuscular taping. Interventions were excluded if they did not meet Cochrane Rehabilitation or Cochrane CAM criteria for structured, evidence-based non-pharmacological therapies. Specifically, we excluded modalities that (1) lacked a clear therapeutic rationale, (2) were not delivered using a standardized, reproducible protocol, or (3) corresponded to unvalidated alternative practices without empirical support (eg, energy healing, magnetic bracelets, crystal therapy).
Comparison: Eligible comparators included:usual oncologic care without additional rehabilitative intervention,sham or placebo procedures (eg, placebo taping, sham acupuncture), or standard pharmacological analgesic regimens used as part of routine clinical care.
Outcomes: Pain, physical function, and quality of life.
Study design: RCTs in English or Spanish.
Exclusion criteria were:
Participants with pain unrelated to arthralgia (eg, neuropathic pain), postopera-tive arthralgia, acute infections, severe trauma, or uncontrolled severe comorbidities (eg, metastatic cancer, systemic inflammatory disease).
Studies assessing only pharmacological or surgical treatments, or interventions not classified as rehabilitative (eg, unvalidated alternative therapies).
Studies using non-validated outcome measures or those focused solely on bio-chemical or inflammatory markers.
Pilot or feasibility studies, study protocols, or unfinished trials. Pilot and feasibility RCTs were excluded because they are primarily designed to assess feasibility, recruitment, acceptability, or procedural aspects rather than treatment efficacy. Their exploratory nature, frequent lack of statistical power, and heterogeneous methodological designs may introduce inconsistency and limit comparability across studies.
Methodological Quality Assessment
The methodological quality of the included RCTs was assessed using the PEDro scale, with the following interpretation: 0–3 poor, 4–5 fair, 6–8 good, and 9–10 excellent. 26 Risk of bias was evaluated with the Cochrane Risk of Bias Tool (RoB 2), considering sequence generation, allocation concealment, blinding, incomplete data, and selective reporting. 27
Results
Study Selection
A total of 826 records were initially identified through database searches. After removing duplicates and applying filters, 113 articles were screened based on their title and abstract. Of these, 13 met the inclusion criteria and were retrieved for full-text review. Ultimately, 8 articles were included in the review,28–35 as shown in Figure 1.
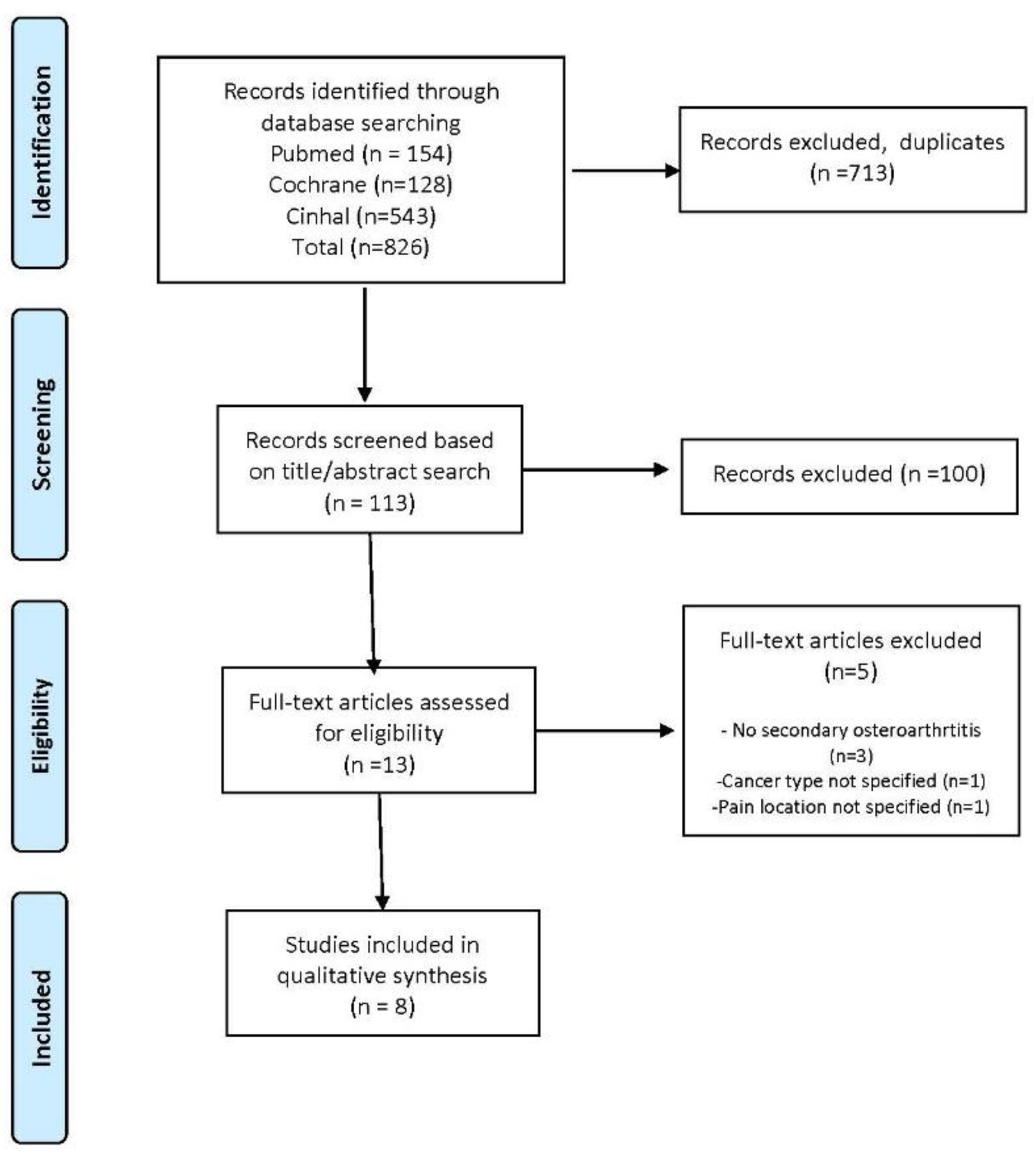
Flow diagram based on PRISMA statement (www.prisma-statement.org, accessed on: 30/01/2020).
The studies involved a total of 822 women, with mean ages ranging between 50 and 64 years. All participants had a diagnosis of BC and experienced hormone therapy-induced arthralgia. The interventions evaluated were non-pharmacological in nature and included rehabilitative strategies. A summary of the included studies is presented in Table 1.
Summary of the Articles Included in the Review.

Description of Interventions
Acupuncture was implemented in three studies,33–35 with protocols ranging from 6 weeks (12 sessions) to 12 weeks (18 sessions). Exercise-based interventions were also reported in three trials,28,30,31 including aerobic and resistance training, Pilates, and self-directed walking. Relaxation techniques 29 and kinesiology taping 32 were evaluated in one study each.
Pain Outcomes
All included RCTs reported pain as a primary outcome. Acupuncture significantly reduced pain at multiple time points, including weeks 6, 12, 16, 20, 24, and 52.32,33 Among the evaluated interventions, acupuncture and structured exercise programs demonstrated the greatest therapeutic potential for reducing aromatase inhibitor–induced pain. Three RCTs of acupuncture25,32,33 consistently showed significant improvements in pain intensity compared with sham or waitlist controls. One trial reported large treatment effects, with standardized mean differences ranging from 1.0 to 1.4 across Brief Pain Inventory (BPI) and WOMAC pain subscales. 25 In the multicenter studies,32,33 adjusted mean differences in BPI worst pain between true and sham acupuncture ranged from 0.92 to 1.08 points (95% CI 0.20-1.91), indicating clinically meaningful reductions sustained up to 52 weeks. Aerobic and resistance training, Pilates, progressive muscle relaxation, and neuromuscular taping also demonstrated statistically significant improvements in pain scores,27–30 as can be seen in Figure 2. Exercise-based interventions produced moderate effect sizes, with standardized mean differences of 0.39–0.46 for improvements in pain and endocrine-related quality of life 28 and a large effect (η2 = 0.83) for pain reduction with Pilates. 29 Progressive relaxation yielded moderate-to-large effects (r = 0.34-0.99) on pain severity and interference, 30 and neuromuscular taping resulted in significant reductions in VAS and EORTC QLQ-C30 pain scores (P = .009 and P = .040, respectively). 27 Overall, these findings suggest that acupuncture and structured exercise interventions provide the strongest evidence for pain reduction, while relaxation and taping strategies may offer complementary benefits supported by smaller studies.

Pain Outcomes. Abbreviations: BPI-SF, Brief Pain Inventory (Short Form); M-SACRAH, Modified-Specific Activity Scale for Rheumatoid Arthritis Health; NRS, Numeric Rating Scale; PROMIS PI-SF, Patient-Reported Outcomes Measurement Information System Pain Interference Short Form; VAS, Visual Analog Scale; WOMAC, Western Ontario and McMaster Universities Arthritis Index.
Figure 2. Pain assessment scales used in the included studies.
Physical Function
Physical function was evaluated in five of the included RCTs, using validated self-reported or performance-based measures. Structured exercise interventions produced the most consistent improvements. In a 12-month randomized trial, combined aerobic and resistance exercise significantly improved physical functioning and quality of life, with standardized mean differences ranging from 0.39 to 0.46 on the FACT-B and FACT-G scales. 28 An 8-week Pilates program achieved a medium-to-large effect on functional performance (η2 = 0.45), though between-group differences did not reach statistical significance. 29 A self-directed 6-week walking program also demonstrated significant improvements in WOMAC function and stiffness subscales (P = .024 and P = .043, respectively), 31 indicating moderate enhancement of mobility and daily activity tolerance. Acupuncture yielded significant gains in joint function and stiffness relief in one trial, with large standardized mean differences (d ≈ 1.0-1.4) across WOMAC and M-SACRAH subscales, 25 whereas in the follow-up multicenter study, no significant improvements were detected on the PROMIS physical function measure. 33 Neuromuscular taping showed nonsignificant trends toward improved upper limb function and mobility, as measured by ULFI and BADIX. 27 Collectively, these findings indicate that exercise-based interventions—particularly combined aerobic and resistance training—provide the most robust evidence for functional improvement, while acupuncture contributes additional benefit through stiffness reduction (Figure 3).

Physical function Scales. Abbreviations: BADIX, Assessment of Arthralgia Related to Aromatase Inhibitors; DASH, Disabilities of the Arm, Shoulder and Hand; FACT-ES, Functional Assessment of Cancer Therapy – Endocrine; FACT-G, Functional Assessment of Cancer Therapy – General; SF-36, 36-Item Short Form Health Survey; SFI, Spinal Function Index; TUG, Timed Up and Go; ULFI, Upper Limb Functional Index; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Quality of Life
Quality of life was evaluated in seven of the included RCTs using validated instruments such as the Functional Assessment of Cancer Therapy (FACT) scales, the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), and the Short Form-36 Health Survey (SF-36). Among these, exercise- and acupuncture-based interventions demonstrated the most consistent improvements. In a 12-month trial, combined aerobic and resistance training significantly enhanced endocrine-related and global quality of life, with standardized mean differences of 0.39–0.46 and mean increases of 6.8 to 8.2 points on the FACT scales, exceeding the minimal clinically important difference. 28 Acupuncture trials also showed favorable effects: Crew et al reported a significant increase in FACT-G physical well-being (P = .03, d ≈ 0.7), 25 while the multicenter studies observed smaller but statistically significant mean improvements on the FACT-ES and PROMIS-PI-SF scales sustained up to 52 weeks.32,33 Neuromuscular taping was associated with significant gains in EORTC QLQ-C30 global health status (+22.9 points, P = .005), 27 reflecting improved physical and emotional functioning. In contrast, progressive relaxation 30 and walking interventions 31 did not significantly affect overall quality of life, despite improvements in pain and mobility (Figure 4).

Quality of life Questionnaires. Abbreviations: EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer – Quality of Life Questionnaire – Core 30; FACT-B, Functional Assessment of Cancer Therapy – Breast; FACT-ES, Functional Assessment of Cancer Therapy – Endocrine; FACT-G, Functional Assessment of Cancer Therapy – General.
Methodological Quality
As detailed in Supplementary Table S2 and summarized in Figure 5, methodological quality was rated as “good” for all included studies (PEDro scores ranging from 6 to 8). Notably, 62.5% of trials received a score of 8/10.

Summary of the methodological quality of the reviewed studies.
Risk of Bias
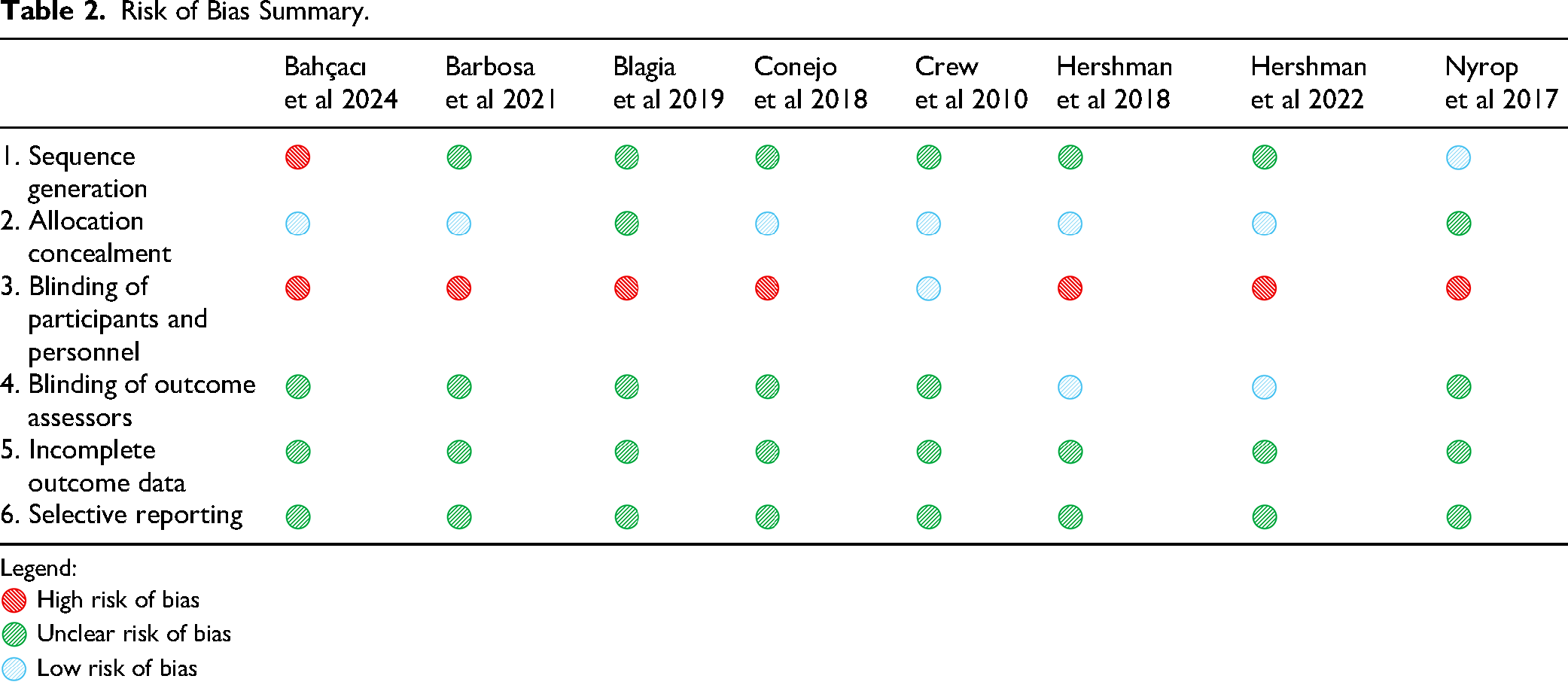
Risk of bias assessment using the Cochrane RoB 2 tool is summarized in Table 2. All studies showed low risk for attrition and reporting bias. Sequence generation methods were considered adequate in 62.5% of trials, while allocation concealment was often unclear. Due to the nature of the inter-ventions, blinding of participants and personnel was judged as high risk in all studies, and assessor blinding was unclear in 75% of cases.
Risk of Bias Summary.
Legend:
 High risk of bias
High risk of bias
 Unclear risk of bias
Unclear risk of bias
 Low risk of bias
Low risk of bias
Discussion
Main Findings
This systematic review provides updated evidence supporting the efficacy of non-pharmacological interventions, such as physical activity and acupuncture, in managing hand arthralgia induced by adjuvant endocrine therapy in BC survivors. Exercise interventions consistently reduced pain and improved hand function when applied over longer durations. Acupuncture also showed significant analgesic effects, though its impact on functional outcomes was more variable. While some studies reported improvements in HRQoL, these effects were less consistent. Moreover, no studies specifically examined the role of occupational therapy, indicating a significant gap in current research.
Interpretations and Comparison with Evidence
Conventional management of endocrine therapy–related arthralgia relies mainly on pharmacological analgesia, NSAIDs, and modifications of endocrine treatment, including temporary interruptions or switching drugs.19,20,36 While these options can be useful in selected cases, their effectiveness is often limited, and long-term use of analgesics or repeated changes in endocrine therapy may not be desirable due to safety considerations and the need to maintain optimal anti-tumor efficacy.20,21 Our findings reinforce the role of non-pharmacological interventions as complementary strategies that can reduce pain and improve function with minimal adverse effects, aligning with previous reviews that have highlighted the potential of exercise and acupuncture for managing aromatase inhibitor–induced musculoskeletal symptoms.21,37
When interpreting these findings in the context of existing evidence, acupuncture and structured exercise interventions appear to offer the greatest therapeutic potential for alleviating aromatase inhibitor–induced arthralgia.25,28,29,32,33 Acupuncture may exert its effects through modulation of endogenous opioid release, local anti-inflammatory mechanisms, and alterations in central pain processing, which together contribute to reductions in joint stiffness and discomfort. Exercise-based interventions, including aerobic, resistance, and Pilates programs, likely improve musculoskeletal flexibility, circulation, and neuromuscular control, thereby mitigating joint pain and enhancing function.28,29,31 Relaxation and neuromuscular taping strategies showed additional but less consistent benefits, supported by smaller single-center trials.27,30
The methodological quality of the available studies, however, remains a limiting factor in interpreting these results. Common sources of bias included small sample sizes, lack of participant blinding, and incomplete reporting of allocation concealment and adherence.25–33 Furthermore, heterogeneity in outcome measures and intervention protocols complicates the synthesis of evidence and may contribute to variability in observed effects. These issues underscore the need for larger, well-designed randomized controlled trials using standardized pain, function, and quality-of-life instruments, along with clear intervention descriptions, to enable more reliable comparisons across studies.
Franzoi et al (2021) 21 offered a broad synthesis of endocrine therapy side effect management, emphasizing acupuncture, physical activity, and behavioral strategies for musculoskeletal symptoms. Our review confirms these findings and extends them by narrowing the focus to hand-specific arthralgia, incorporating recent high-quality RCTs that demonstrate improvements in both pain and function.28–35
Roberts et al (2017) 37 identified moderate-quality evidence for acupuncture and exercise in addressing musculoskeletal side effects of aromatase inhibitors, but highlighted limitations due to small sample sizes and outcome heterogeneity. Our updated analysis incorporates more recent randomized controlled trials with improved methodological reporting and a specific focus on hand-related outcomes, thereby enhancing the contextual and clinical relevance of the findings. However, the overall methodological quality of the included studies remains moderate, with common limitations including small sample sizes, lack of blinding in behavioral interventions, and variability in outcome measures.28–35
Chan et al (2020) 38 reviewed various interventions for endocrine therapy-related symptoms and reported inconsistencies, particularly regarding HRQoL. Our results similarly show mixed effects on HRQoL, but more robust and consistent improvements in pain and function, likely due to the focused scope and stricter inclusion criteria.
Condorelli and Vaz-Luis (2018) 36 stressed that adverse effects of endocrine therapy are often overlooked in follow-up care, leading to reduced adherence. Our findings support this concern, showing that unmanaged hand pain and dysfunction can significantly impair daily activities.28–35 Effective non-pharmacological strategies, when tailored and integrated into survivorship care, could improve tolerability and support long-term adherence to endocrine therapy.
Compared with earlier reviews, our synthesis incorporates more recent randomized controlled trials with clearer methodological reporting, a focus on hand-related and function-oriented outcomes, and inclusion of a wider range of non-pharmacological approaches. Rather than strengthening the overall evidence base, this review provides an updated and integrative overview of available studies, highlighting emerging but still underutilized interventions and identifying persistent gaps that warrant further high-quality research.
Implications for clinical practice and research
The findings of this review support the integration of non-pharmacological interventions, particularly acupuncture and structured exercise programs, into the supportive care of breast cancer survivors receiving aromatase inhibitors. Acupuncture protocols in the included RCTs typically involved 12 sessions delivered over 6 to 12 weeks, using manual acupuncture techniques.25,32,33 Frequently stimulated acupoints included LI4 (Hegu), LI11 (Quchi), ST36 (Zusanli), SP6 (Sanyinjiao), and LR3 (Taichong), often supplemented by local points around the affected joints. Treatment was well tolerated, with only mild and transient adverse effects such as bruising or soreness reported. Consistent with current ASCO clinical practice guidelines, acupuncture can be recommended, when feasible, as an adjunctive therapy to relieve aromatase inhibitor–related arthralgia in appropriately selected patients. 34
Exercise interventions also demonstrated favorable outcomes and can be feasibly implemented in survivorship care. Combined aerobic and resistance training performed at moderate intensity (approximately 150 min per week of aerobic activity plus two weekly sessions of strength training) yielded significant improvements in pain, function, and quality of life. 28 Pilates and walking programs represent additional low-cost, accessible options that can be adapted to individual preferences and physical capacity.29,31 Incorporating these approaches within multidisciplinary oncology rehabilitation programs may improve adherence and enhance functional recovery.
Future research should aim to standardize acupuncture and exercise protocols, ensure adequate blinding where feasible, and assess cost-effectiveness and long-term sustainability. Pragmatic clinical trials with clear reporting of adherence and patient acceptability would provide further evidence to guide implementation in routine care.
Finally, no randomized controlled trials specifically evaluated occupational therapy interventions. This represents a notable research gap, as occupational therapy strategies—such as joint protection education, activity modification, ergonomic adaptations, and graded hand exercises—are directly applicable to the daily activity limitations reported by affected patients. Evidence from rheumatology populations suggests that such interventions can improve hand function, reduce pain, and support independence. 39 Incorporating occupational therapy approaches into future trials may therefore enhance symptom management and optimize adherence to endocrine therapy through improved functional capacity and quality of life. 40
Strengths and Limitations
A strength of this review lies in its focused scope on hand arthralgia induced by adjuvant endocrine therapy, an underexplored but significant adverse effect. The systematic methodology, strict inclusion criteria, and synthesis of recent RCTs enhance the clinical relevance of the findings. Moreover, the evaluation of both pain and functional outcomes offers a more comprehensive understanding of intervention effects.
This review has several limitations. First, only studies published in English or Spanish were included, which may have introduced language bias and excluded potentially relevant research published in other languages. Second, substantial heterogeneity was observed across the included trials regarding intervention type, duration, comparator, and outcome measurement tools. Together with the small number of eligible studies, these differences limited the feasibility of conducting a meta-analysis or subgroup analyses. Consequently, the findings should be interpreted as a qualitative synthesis intended to summarize current evidence rather than to provide pooled effect estimates.The inability to blind partici-pants and therapists—due to the nature of the interventions—introduces performance bias, while allocation procedures were often inadequately reported. Functional out-comes were frequently secondary endpoints, and long-term effects remain unclear due to short follow-up durations. Finally, the absence of trials involving occupational therapy highlights a persistent gap in the evidence base.
Conclusions
This review summarizes current evidence on non-pharmacological interventions for managing aromatase inhibitor–induced arthralgia in breast cancer survivors. Acupuncture and structured exercise programs, particularly those combining aerobic and resistance components, show the most consistent benefits in reducing pain and improving physical function. Progressive relaxation and neuromuscular taping may offer complementary effects, although further validation is needed. Despite encouraging results, methodological limitations and heterogeneity across studies constrain the overall strength of evidence.
Future research should prioritize well-designed randomized trials with standardized outcome measures, adequate blinding where feasible, and long-term follow-up to assess durability of effects. Incorporating occupational therapy interventions, evaluating cost-effectiveness, and integrating patient-reported outcomes will be essential to enhance clinical applicability. In practice, evidence-based implementation of acupuncture and exercise within multidisciplinary survivorship programs could improve symptom control, adherence to endocrine therapy, and quality of life for women affected by AIA.
Supplemental Material
sj-docx-1-chp-10.1177_2515690X261423036 - Supplemental material for Effectiveness of Non-Pharmacological Interventions for Hormone Therapy-Induced Hand Arthralgia in Breast Cancer Patients: A Systematic Review
Supplemental material, sj-docx-1-chp-10.1177_2515690X261423036 for Effectiveness of Non-Pharmacological Interventions for Hormone Therapy-Induced Hand Arthralgia in Breast Cancer Patients: A Systematic Review by Nuria Muñoz-Bermúdez, Vanessa Abril-Esteban, Jorge Hugo Villafañe, Nuria Bonsfills-García, Roberto Ucero-Lozano, César del-Barco-Luengo and Vanesa Abuín-Porras in Journal of Evidence-Based Integrative Medicine
Supplemental Material
sj-docx-2-chp-10.1177_2515690X261423036 - Supplemental material for Effectiveness of Non-Pharmacological Interventions for Hormone Therapy-Induced Hand Arthralgia in Breast Cancer Patients: A Systematic Review
Supplemental material, sj-docx-2-chp-10.1177_2515690X261423036 for Effectiveness of Non-Pharmacological Interventions for Hormone Therapy-Induced Hand Arthralgia in Breast Cancer Patients: A Systematic Review by Nuria Muñoz-Bermúdez, Vanessa Abril-Esteban, Jorge Hugo Villafañe, Nuria Bonsfills-García, Roberto Ucero-Lozano, César del-Barco-Luengo and Vanesa Abuín-Porras in Journal of Evidence-Based Integrative Medicine
Footnotes
Authors’ Contributions Statement
Author Contributions: Conceptualization, N.M.-B., V.A.-E., and V.A.-P.; methodology, N.B.-G., R.U.-L., and C.d.-B.-L.; formal analysis, N.B.-G., R.U.-L., and C.d.-B.-L.; investigation, N.M.-B., V.A.-E., and V.A.-P.; writing—original draft preparation, N.M.-B., V.A.-E., and V.A.-P.; writing—review and editing, V.A.-P.; and J.H.V.; supervision, V.A.-P. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.