
Abstract
Objective
This review synthesizes current evidence on the efficacy of acupuncture in managing chemotherapy-induced peripheral neuropathy (CIPN) in cancer patients, focusing on its mechanisms, clinical applications, and future research directions.
Methods
This narrative review synthesizes and critically appraises findings from randomized controlled trials (RCTs), meta-analyses, and preclinical studies, evaluating acupuncture's impact on pain relief, neurological function, and quality of life. Key databases were searched for studies published up to 2024.
Results
Nineteen RCTs (n = 1174) demonstrated significant improvements in CIPN symptoms with acupuncture, particularly in reducing neuropathic pain (eg, via endogenous opioid modulation) and enhancing sensory function (eg, BDNF-mediated neuroplasticity). Optimal protocols involved 2–3 sessions/week for 4–12 weeks, targeting acupoints such as ST36 and LI4. Acupuncture outperformed pharmacotherapy (eg, duloxetine) in safety and patient-reported outcomes.
Conclusion
Acupuncture is a promising adjunctive therapy for CIPN, offering multimodal mechanisms and clinical benefits. Standardization of protocols and further high-quality RCTs are needed to strengthen evidence and guide integration into oncology care.
Keywords
Introduction
Chemotherapy-induced peripheral neuropathy (CIPN) is a debilitating condition affecting 19%–85% of cancer patients, with prevalence influenced by chemotherapy type (eg, taxanes and platinum drugs), cumulative dose, and patient-specific factors such as age and comorbidities.1–6 Notably, paclitaxel exhibits high neurotoxicity, inducing CIPN in up to 79.1% of patients, often persisting post-treatment and significantly impairing quality of life.5–12 The pathophysiology involves neurotoxic agent-induced neuronal damage, oxidative stress, and disrupted nerve conduction, which may necessitate dose reductions or treatment discontinuation, further complicating cancer management.1–5,13–18 Clinically, CIPN manifests as pain, numbness, and tingling, impairing daily function and emotional well-being, with associated anxiety and depression exacerbating patient distress.19,20°Current pharmacologic therapies (eg, duloxetine—which is cautiously recommended in the American Society of Clinical Oncology (ASCO) guidelines based on limited efficacy—and gabapentin) often demonstrate suboptimal outcomes and adverse effects, underscoring the need for alternative strategies.21,22 Acupuncture, a Traditional Chinese Medicine (TCM) modality, has emerged as a potential intervention by modulating pain pathways and promoting neurological recovery through targeted needle stimulation.8–11 Preclinical and clinical studies suggest its utility in mitigating cancer-related symptoms, warranting further investigation into its mechanisms, clinical applications, and integration into multidisciplinary CIPN management to optimize patient outcomes.8–11,21–23
The Basic Principles and Therapeutic Mechanisms of Acupuncture
Conventional CIPN management uses antiepileptics and antidepressants like duloxetine for neuropathic pain, but these are palliative and do not address neurodegeneration or sensory deficits affecting quality of life.24,25
Acupuncture is gaining attention as a therapeutic option for CIPN, supported by clinical trials showing its effectiveness in pain management and quality of life.26–28 As part of TCM, it works through various mechanisms, including neuromodulation and microcirculation enhancement.29–33 Preclinical studies indicate it may promote nerve regeneration and modulate inflammation, distinguishing it from conventional drugs and making it a promising complementary treatment for CIPN.29–33
While preliminary findings are encouraging, further rigorous clinical investigations are needed to fully elucidate acupuncture's therapeutic potential and optimize treatment protocols for CIPN management. Future research should particularly focus on its long-term effects on nerve regeneration and functional recovery, as well as potential synergistic effects with conventional therapies.
Neurophysiological Mechanisms of Acupuncture in CIPN Management
Acupuncture exerts comprehensive neuromodulatory effects through multi-level mechanisms involving molecular, neural pathway, and systemic interactions. At the molecular level, acupuncture stimulates endogenous opioid release (β-endorphins, enkephalins) binding to μ-/δ-opioid receptors,10,34 while concurrently modulating neurotransmitters (serotonin, dopamine) for pain and mood regulation. 35 These effects are amplified through neurotrophic factor activation, particularly brain-derived neurotrophic factor (BDNF), which enhances neuronal survival, synaptic plasticity, and neurogenesis.1,32,33
The intervention's analgesic efficacy is mediated through hierarchical neural pathways: peripherally, it alters nociceptive signal transmission via Aδ/C-fiber modulation36,37; centrally, it activates descending inhibitory pathways (brainstem-thalamocortical circuits) and reorganizes pain-processing neural networks.36,37 Simultaneously, acupuncture induces autonomic nervous system rebalancing, shifting sympathetic hyperactivity to parasympathetic predominance,7,38 thereby restoring homeostasis - a critical effect for chronic neuropathic pain management.35,36,39
Complementing these neural effects, acupuncture improves microcirculation to facilitate tissue repair36–38,40 and promotes neuroadaptive responses through acupoint-specific stimulation (eg, ST36, LI4).12,13,28,36,37,39,41 This integrated mechanism profile underlines acupuncture's clinical value in CIPN by concurrently addressing pain perception, nerve regeneration, and systemic physiological function. 12 (Figure 1)

Proposed Mechanisms of Acupuncture in Alleviating CIPN.
Applications of Acupuncture in Pain Management
Acupuncture is increasingly recognized as an evidence-based modality for neuropathic pain management, including CIPN.38,39 Its efficacy is attributed to the modulation of chronic pain mechanisms, such as neuroinflammation and oxidative stress, within the central nervous system.12,24 As a safe, non-opioid option, it offers a personalized approach for high-risk populations and shows synergistic potential with pharmacotherapy, potentially allowing for reduced analgesic doses and fewer side effects. 14
Acupuncture Treatment Protocol
Integrating acupuncture into treatment requires understanding optimal practices for efficacy, focusing on frequency, duration, acupoint selection, and supportive therapies.
Frequency and Duration of Acupuncture Treatment
Acupuncture frequency and duration significantly affect outcomes, with common regimens being two to three sessions weekly for 4 to 12 weeks. 40 Studies show that twice-weekly sessions for eight weeks improve pain and quality of life in CIPN patients, while a 12-week weekly electro-acupuncture protocol reduces neuropathic symptoms in colorectal cancer patients. 35 Evidence indicates that a structured, individualized treatment schedule enhances outcomes, and consistent frequency reinforces therapeutic effects for lasting relief. 29
Selection of Acupoints and Theoretical Basis
The selection of acupoints is fundamental to the effectiveness of acupuncture. Research indicates that specific acupoints, such as LI4 (Hegu), ST36 (Zusanli), and SP6 (Sanyinjiao), are frequently utilized in the treatment of CIPN, as they are believed to influence the nervous system and promote healing. 33 The theoretical basis for these selections is rooted in TCM, which posits that these points can regulate the flow of Qi (energy) and blood, thereby alleviating pain and restoring function. A systematic review identified these acupoints as core targets for acupuncture interventions aimed at CIPN, underscoring their relevance in clinical practice. 30 Moreover, the choice of acupoints can be adapted based on individual patient profiles, symptoms, and underlying conditions, allowing for a personalized approach that may enhance treatment efficacy. 22 This flexibility in acupoint selection, combined with a solid understanding of TCM principles, can lead to improved clinical outcomes for patients receiving acupuncture for neuropathic pain. (Table 1)
Acupuncture Point Protocol.
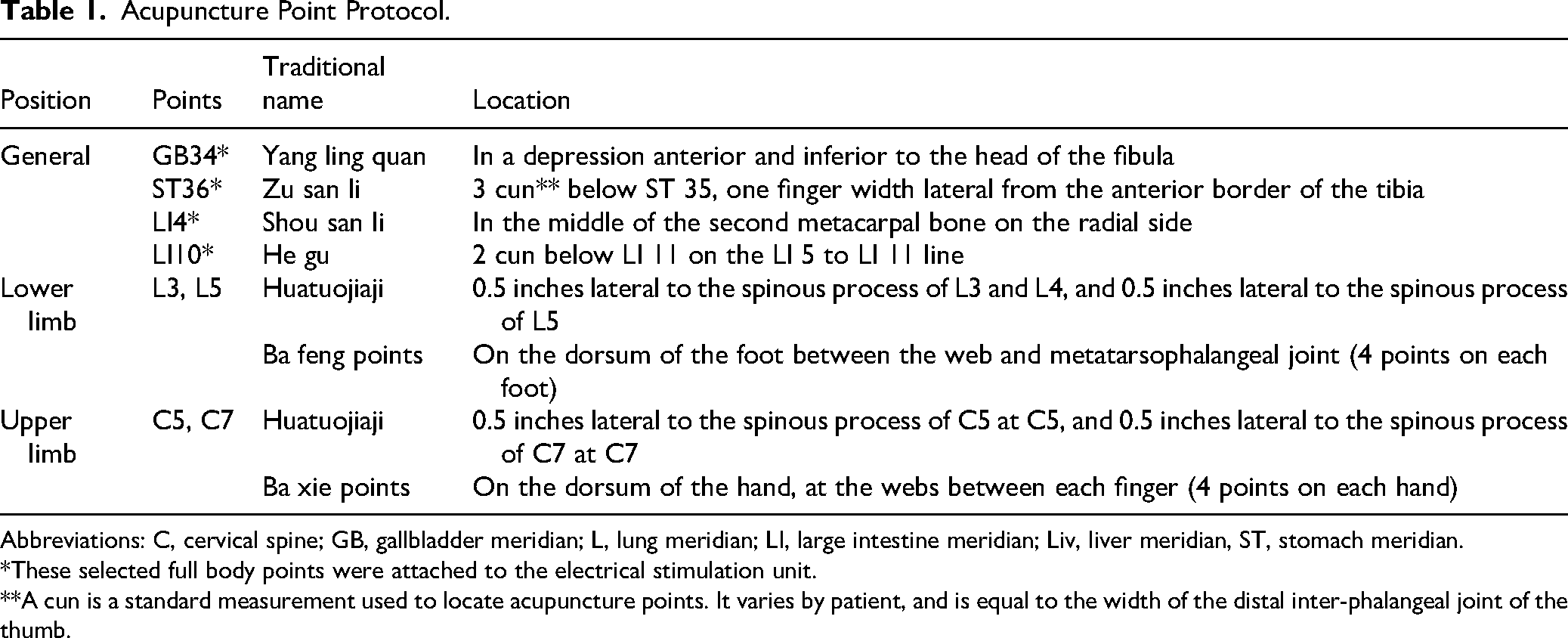
Abbreviations: C, cervical spine; GB, gallbladder meridian; L, lung meridian; LI, large intestine meridian; Liv, liver meridian, ST, stomach meridian.
*These selected full body points were attached to the electrical stimulation unit.
**A cun is a standard measurement used to locate acupuncture points. It varies by patient, and is equal to the width of the distal inter-phalangeal joint of the thumb.
In summary, a review of the current literature suggests an emerging consensus on several key aspects of acupuncture for CIPN. Commonly employed elements include the use of core acupoints such as ST36 (Zusanli), LI4 (Hegu), and SP6 (Sanyinjiao), a treatment frequency of 2–3 sessions per week, and a duration ranging from 4 to 12 weeks. However, significant inconsistencies remain, particularly regarding the optimal total number of sessions, the specific parameters for electroacupuncture stimulation (eg, waveform, intensity), and the customization of point prescriptions for different neurotoxic agents. Establishing standardized protocols that address these variables is a critical next step for the field.
Clinical Research on Acupuncture in the Treatment of CIPN
Recent clinical research, including 19 randomized controlled trials (RCTs, n = 1174), suggests that acupuncture significantly improves CIPN symptoms—such as neuropathic pain, sensory function, and quality of life compared to conventional medications (eg, duloxetine, gabapentin) and sham interventions.29,3336–38,40 A network meta-analysis further supports the superiority of electroacupuncture (EA) in treatment efficacy, with additional benefits of fewer adverse effects and higher patient satisfaction. 40 (Figure 2.) However, heterogeneity in acupuncture protocols and outcome measures underscores the need for standardized methodologies. While current evidence positions acupuncture as a promising alternative or adjunct to pharmacotherapy, further rigorous trials are warranted to optimize protocols and confirm its comparative effectiveness within multimodal CIPN management.23,34 Evaluating acupuncture efficacy is vital for understanding its effects on pain management and quality of life, using quantitative and qualitative measures like pain scores and functional assessments. These standards aid clinical practice and research, allowing clinicians to objectively measure patient responses and make informed decisions about integrating acupuncture into care plans.

Schematic of a Representative Electroacupuncture (EA) Protocol for CIPN. This Illustration Depicts the Common Therapeutic Principle of Combining Local Points (eg, Lumbar Huatuojiaji) with Distal Points (eg, ST36, LI4) to Regulate Qi and Blood Flow, Alleviate Nerve Inflammation, and Reduce Pain.
The application of acupuncture in the context of CIPN can be broadly categorized into two strategies: prevention during chemotherapy and treatment of established CIPN. A few studies have explored the prophylactic potential of acupuncture. For instance, Huang et al 36 reported that acupuncture concurrent with oxaliplatin chemotherapy may reduce the incidence of severe CIPN. In contrast, the majority of existing RCTs, such as the pilot trial by Lu et al 28 and the study by Bao et al, 39 have focused on treating patients who had already developed significant neuropathic symptoms after chemotherapy, demonstrating improvements in pain and sensory function.
The efficacy of acupuncture may vary depending on the neurotoxic agent involved. The most substantial evidence exists for CIPN induced by taxanes (eg, paclitaxel) and platinum-based drugs (eg, oxaliplatin). Studies on taxane-induced CIPN, primarily in breast cancer patients, have consistently shown positive effects on sensory symptoms and pain.28,39 Similarly, trials focusing on oxaliplatin-induced CIPN in patients with colorectal cancer have also reported benefits, particularly in reducing cold-induced allodynia and numbness.35,41 Evidence for vinca alkaloid-induced CIPN is currently more limited, reflecting a gap in the literature that future research should address.
The temporal profile of CIPN—whether acute or chronic—also merits consideration. Acupuncture has been investigated predominantly for chronic, persistent CIPN that remains after chemotherapy cessation. The positive outcomes in these studies suggest a role in long-term symptom management and functional recovery. Its role in managing the acute, transient neuropathic symptoms that occur immediately during or after specific chemotherapies (eg, acute oxaliplatin-induced cold sensitivity) is less well-defined, though some pilot studies indicate potential utility. 41
However, the interpretation of these promising findings must be tempered by significant methodological limitations prevalent in the current evidence base. Many of the cited RCTs are characterized by small sample sizes, which constrain their statistical power and the generalizability of the results. Furthermore, there is considerable heterogeneity in acupuncture protocols, including variations in needling technique, stimulation parameters, and session frequency, complicating the identification of a universally optimal treatment regimen. The inherent challenges in blinding both practitioners and patients in acupuncture trials also introduce potential for performance and detection bias. These limitations collectively underscore the need for more rigorous and standardized future investigations.
Future Research Directions and Challenges
The exploration of acupuncture, particularly in the context of its mechanisms and clinical applications, presents a promising avenue for future research. As acupuncture continues to gain recognition in the medical community, understanding its underlying mechanisms and identifying relevant biomarkers will be crucial for optimizing its efficacy and expanding its clinical use.
Building on current mechanistic insights, future research should be channeled into specific, actionable priorities, beginning with the execution of large-scale, multicenter RCTs that employ rigorously standardized and reproducible acupuncture protocols to definitively establish efficacy across diverse patient populations.11,4°Concurrently, there is a critical need to explore and validate objective biomarkers—such as microRNAs, inflammatory cytokines, and data from proteomic or metabolomic analyses—to elucidate the mechanisms of action, monitor treatment response, and ultimately personalize therapy.13,23 Furthermore, practical studies investigating the integration of acupuncture into structured, multimodal integrative oncology care pathways are essential to assess its comprehensive impact on clinical outcomes, patient-reported experiences, quality of life, and healthcare utilization. 40 Addressing these interconnected priorities will be pivotal in generating the robust evidence base required to solidify acupuncture's role in mainstream CIPN management.
Conclusion
Acupuncture shows promise for alleviating CIPN in cancer patients, but current studies have limitations like small samples and varied techniques. Balancing diverse research on acupuncture's efficacy is crucial, as some studies show significant improvements in pain while others do not, highlighting the need for robust trials. Future research should involve larger, multi-center studies to assess efficacy and mechanisms of acupuncture in managing CIPN. Additionally, integrating acupuncture into clinical practice requires considering patient needs and a collaborative approach among healthcare providers. Generating robust evidence that meets the criteria for inclusion in major oncology guidelines, such as those from ASCO and the National Comprehensive Cancer Network (NCCN), is essential for its wider adoption.
Ultimately, while the current evidence suggests a potential benefit of acupuncture in mitigating CIPN, a concerted effort is needed to address the gaps in the literature. This includes establishing clear guidelines for acupuncture practice in oncology, fostering interdisciplinary collaborations, and encouraging ongoing education for healthcare providers. By doing so, we can improve patient outcomes and quality of life for those navigating the challenges of cancer treatment, while also paving the way for further advancements in integrative oncology.
Footnotes
Author Contributions
Conceptualization:XQ.Investigation:XQ, LTY, JYW. Writing - Original Draft: XQ. Writing - Review & Editing: XQ, LJC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is supported by the Linglong Yingcheng Hospital Original Foundation (YCYY2023ZZ002).