
Abstract
Objective
this meta-analysis evaluates the effects of mind-body exercise (MBE) on cognitive function in older adults with or without mild cognitive impairment (MCI). We examined the impact of different MBE, including yoga, tai chi, qigong, and meditation, on six cognitive domains: attention, executive function, working memory, verbal memory, processing speed, and visual-spatial construction.
Methods
We searched eight electronic databases from inception till August 2024. The literature search, study selection, data extraction, methodological quality assessment and statistical analyses were performed.
Results
A total of 45 studies, comprising 4602 participants, were included. Results indicated that MBE had a moderate positive effect on visual-spatial construction (Hedges’ g = 0.46) and small effects on other domains such as verbal memory (Hedge's g = 0.24), processing speed (Hedge's g = 0.26), working memory (Hedges’ g = 0.15) and executive function (Hedges’ g = 0.10). However, there was no improvement in attention (Hedge's g = 0.08, 95% CI = −0.07 to 0.23). The meta-regression analysis further revealed that participants with MCI experienced greater improvements in visual-spatial construction and executive function than healthy participants. Additionally, significant differences were observed among intervention types, with yoga and tai chi showing stronger effects on visual-spatial construction and verbal memory than meditation.
Conclusions
These findings suggest MBE is an effective intervention for improving cognitive function, especially in MCI populations and with certain types of interventions. Utilization of validated modules for MBE intervention and inclusion of long-term follow-up assessments to establish conclusive findings were also suggested.
Keywords
Introduction
The global population is undergoing aging at uneven speeds worldwide. The percentage of individuals aged 60 year and older is projected to rise, increasing from 12% in 2015% to 22% by 2050. 1 The typical aging process is linked to deterioration in physical well-being and reduction in cognitive abilities. In addition to generalized slowing, some older adults may also suffer from mild cognitive impairment (MCI) or any type of dementia. The estimated global prevalence of dementia is 47 million individuals, with a projected increase to 115.4 million individuals by 2050. 2 The significance of identifying effective interventions to ameliorate typical progressive cognitive decline or enhance cognitive function among the aging population is underscored by the substantial number of individuals impacted and considerable strain on healthcare systems. Therefore, clinicians and researchers have attempted to develop new treatments or intervention to prevent or delay cognitive impairment and to evaluate the efficacy of them.
Pharmacological interventions for mental diseases have demonstrated utility. However, several unmet requirements persist. 3 Empirical research demonstrated that engaging in cognitive training and regular exercise had a beneficial role in maintaining older adults’ cognitive and mental well-being.4,5 Various studies reported that exercise exerted positive effects on cognitive function through several mechanisms, such as the facilitation of neurogenesis, synaptogenesis, and capillarization, as well as elevation of brain-derived neurotrophic and insulin-like growth factors.6,7 The interaction of multiple factors contributed to the neuroprotective benefits of exercise on older adults’ cognitive function.
Since the efficacy of exercise has been proven, there has been growing interest in the field of mind-body exercise (MBE).8-11 MBE refers to a form of multimodal exercise that encompasses various activities that involve the relaxation of skeletal muscles, slow physical motion, and stretching, together with breathing techniques and cognitive attention, to maintain a meditative state. MBE involves Tai Chi, yoga, meditation, and qigong.9,11 Its use was appropriate for vulnerable populations, such as people experiencing cognitive decline, such as MCI, and those with limited exercise tolerance. This is owing to the leisurely, low-impact nature of the bodily motions in MBE, which is performed at a mild-to-moderate intensity level. 8
MBE consumes a smaller amount of energy metabolism relative to brisk walking and yields similar outcomes regarding cardiovascular health benefits by reducing blood cholesterol levels, body composition, and maximizing oxygen consumption.12,13 Furthermore, the movement attributes offer supplementary cognitive stimulation.8,14,15 The execution of coordinated sequential movements demand memory training as well as multiple higher cognitive functions, such as processing speed, visual-spatial construction, attention, multitasking, and planning.8,15 These findings suggest that MBE may serve as an alternative medical approach for the prevention or reversal of MCI.
Previous reviews independently conducted evaluations that specifically examined the effectiveness of Tai Chi,16,17 yoga,3,18 and meditation19,20 in enhancing cognitive function among older individuals. Discrepancies in the inclusion and exclusion criteria and varied methodologies used to analyze outcomes makes it difficult to establish significant comparisons within and between different domains. Therefore, conducting a single review that simultaneously examines multiple cognitive domains would be beneficial.
Recently, several studies performed a meta-analysis to examine the potential cognitive benefits of MBE.21-23 They reported that MBE might enhance neuroplasticity, a crucial factor for cognitive functions, particularly in aging populations at risk for cognitive decline. 22 Several studies have demonstrated that MBE is associated with improved brain activation patterns and increased gray matter volume in areas related to attention, memory, and executive function, while also promoting relaxation and reducing stress, thereby enhancing cognitive health.21,22 Additionally, the meditative aspects of MBE contributes to improved emotional regulation, which further supports cognitive health by mitigating the detrimental effects of chronic stress on the brain.22,23 MBE has also been shown to enhance functional connectivity between brain networks, leading to improvements in overall cognitive performance, particularly in tasks involving visuospatial memory and inhibitory control. 21 Furthermore, these exercises bolster physical health, indirectly benefiting cognitive function by improving circulation and reducing inflammation.21,24 These meta-analysis studies suggested that MBE present a promising intervention for preventing or slowing cognitive decline in the aging population.21,22 However, despite growing evidence supporting the cognitive benefits of MBE, the extent to which different types of these exercises affect various cognitive domains in older adults, including those with MCI, remains unclear. To address this, we conducted a comprehensive meta-analysis of randomized controlled trials (RCTs) and observational studies, evaluating the efficacy of MBEs on specific cognitive domain. To this end, we categorized cognitive domains into six areas including attention, executive function, working memory, verbal memory, processing speed, and visual-spatial construction based on widely used domain definitions.18,25-29
Additionally, considering the latest empirical studies on the efficacy of MBE on cognitive function, it is imperative to revise and update existing meta-analytical research. Hence, this meta-analysis aimed to investigate the efficacy of MBE on cognitive function in the aging population via studies published between 1989 and 2024. The findings of this study will offer practitioners with empirical evidence for the development of interventions aimed at maintaining and improving cognitive function. Additionally, it will shed light on areas that require further investigations.
Materials and Methods
Study Protocol Registration
We conducted a meta-analysis study in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and a study protocol. 30 The protocol of this meta-analysis study was performed following a pre-established protocol registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42023401854).
Study Selection Criteria
Two reviewers independently searched and screened the retrieved studies according to predefined selection criteria. The inclusion criteria for the meta-analysis were as follows: 1) Population: healthy older people or patients with MCI aged 55 years or older; 2) Intervention: any type of mind-body exercise (ie, yoga, meditation, tai chi, and qi gong)31-33; 3) Comparison: control groups not receiving specific intervention or minimal intervention (Passive controls: no intervention, or waitlist control and care as usual) or receiving some form of activity (Active controls: education, physical exercise, and cognitive training) 34 ; 4) Outcomes: changes in at least one cognitive domain, such as processing speed, working memory, verbal memory, attention, executive function, or visual-spatial construction18,26,28,29; and 5) Study Design: RCTs and observational studies.
Exclusion criteria were: 1) case reports, case series, conference proceedings, and published abstracts, 2) people with moderate-to-severe cognitive impairment (dementia or Parkinson's disease) or neurological disorders (Alzheimer's disease, epilepsy, schizophrenia, and multiple sclerosis), 3) studies including other psychological or psychopharmacological therapies in addition to MBE as an intervention and 4) articles without specific statistical information. There were no limitations on the language, country, and participants’ gender or ethnicity.
Literature Search Strategy
Two researchers independently searched eight electronic databases, which included PubMed, PsycINFO, Web of Science, Google Scholar, the Cochrane Central Register of Controlled Trials (CENTRAL), ProQuest Dissertations, EMBASE, and Scopus, for articles from inception till August 2024.
The search terms included five groups: (older adults OR older people OR elderly OR aging OR senior) AND (cognition OR cognitive domain OR cognitive function OR attention OR memory OR processing OR verbal OR language OR fluency OR visuospatial OR visual spatial OR executive function OR working memory OR short term memory) AND (mind body exercise OR Mindful exercise OR meditative movement OR Qigong OR Baduanjin OR Tai Chi OR Taiji OR Yoga OR meditation OR Mindfulness-based stress reduction) AND (randomized OR random OR randomly OR randomization OR randomization OR RCT OR RCTS). Furthermore, the bibliographies of the selected studies were manually searched to identify additional studies.
Data Extraction
Data from the selected studies were independently extracted by two research assistants via a predefined data extraction form: author, title, year of publication, experimental design, sample size, population type (MCI or healthy), mean age of the population, type of mind-body exercises in the intervention group, intervention type for the control group, measurement, cognitive domain assessed, intervention frequency, period, training duration, and pre- and post-out comes. Extracted data were cross-checked, and a consensus was reached by consulting a third researcher in case of disagreements.
Quality Appraisal
Study quality assessments were performed by two independent researchers via the Physiotherapy Evidence Database (PEDro) scale. 35 This tool contained 11 yes/no items: 1) eligibility criteria specified, 2) random allocation, 3) concealed allocation, 4) groups similar at baseline, 5) subject blinding, 6) therapist blinding, 7) assessor blinding, 8) less than 15% dropouts, 9) intention-to-treat analysis, 10) between-group statistical comparisons, 11) and point measures and variability data. The classification of each study was based on its quality, which was categorized as outstanding (9-10), good (6-8), fair (4-5), or bad (<4). All disagreements or discrepancies were settled via discussions with an independent, experienced literature reviewer.
Statistical Analysis
To display the findings in forest plots and synthesize them, meta-analyses were performed using the meta-package (version 6.1-0) in R version 4.1.0 (R Foundation for Statistical Computing).36,37 Hedges’ adjusted g was used to calculate the effect sizes for the standardized mean difference (SMD). In this meta-analysis, the SMD was chosen over the Mean Difference (MD) because the included studies utilized different instruments to measure cognitive outcomes. SMD standardizes the results across diverse scales, allowing for comparison of effect sizes even when different measurement tools are used.38,39 This approach ensures a more consistent and interpretable summary of intervention effects on cognitive function. SMD values of 0.15–0.40, 0.40–0.75, and > 0.75 were considered small, medium, and large, respectively. 40 To pool the summary SMD, random-effects models were applied. This method had a more conservative weighting estimate as it considered real differences in the intervention efficacy in each study and sampling variability (actual sample distribution). 41 Furthermore, it allowed the conclusions to be generalized to a wider array of situations, since this provided a better reflection of the “real world”. 42
Tests for heterogeneity were conducted and assessed using I2, Tau2, and Q statistics, which provided an estimate of the percentage of variability in a meta-analysis explained by the differences across studies rather than by sampling errors. An I2 of less than 25%, 25%–50%, and over 50% was usually viewed as low, moderate, and high heterogeneity, respectively. 43 A p-value of < 0.05 for the Q statistic and Tau2 > 50% reflected significant heterogeneity. 44 Publication bias was assessed via the Kendall's τ and Egger's tests and funnel plots. 45
Additionally, a meta-regression analysis was conducted to explain heterogeneity between studies and to assess the impact of potential moderator variables. 46 Then, subgroup meta-analyses were conducted based on based on moderator variables that were found to be significant in a meta-regression. This helps to further explore and clarify the impact of these moderator variables on effect sizes within more homogeneous subgroups. 39 These analyses assessed the moderating effects of intervention frequency, duration, period participant type (ie, MCI or healthy older), intervention type (ie, yoga, tai chi, qi gong, meditation), and control type (ie, passive control, physical activity, others).
Results
Study Selection
The flow diagram for literature search and study selection was shown in Figure 1. A total of 5407 records were retrieved. Articles were screened in accordance with study characteristics (name of first author, publication year, and title), irrelevant and duplicates were removed, and 117 relevant studies were reviewed. Among these, 75 literatures were excluded due to their failure to meet the study criteria unavailability of data extraction, non RCT, and unsuitable participants). Additionally, three literatures were identified through snowballing search. In total, 45 articles were considered and included nine, 26, 21, 27, 24, and 13 studies on attention, executive function, working memory, verbal memory, processing speed, and visual-spatial construction, respectively.
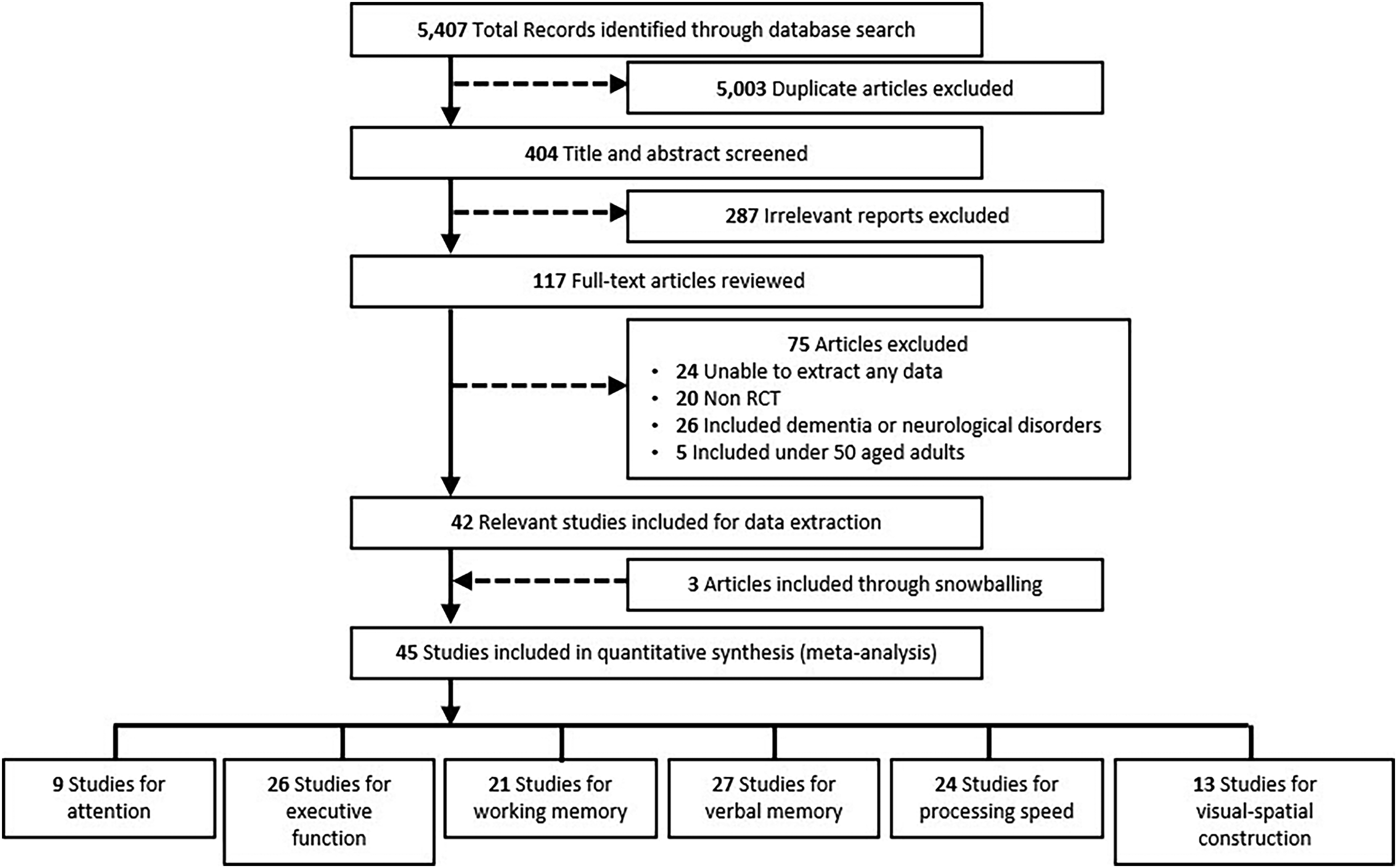
Flow Diagram of Study Selection.
Study Characteristics
Table 1 provides a comprehensive overview of the key attributes of the studies that have been incorporated in this analysis. The studies were conducted and published from 1989 to 2024. Of the include studies, five involved two control groups and the remaining had only one control group. The intervention group included various mind-body exercises such as yoga, meditation, Qigong, and Tai chi, while the control group included no intervention, newspaper music, exercise, brisk walking, aerobics, education, or cognitive training programs. The sample size ranged from 15–792, and a total of 4602 older adults (3460 healthy people and 1142 patients with MCI) were included in 63 RCTs. Of these, 2274 and 2328 participants were assigned to mind-body exercises and control conditions, respectively. The participants’ mean age ranged from 59–84 years. Intervention period ranged from 2 to 240 weeks. Various training session times (12-150 min) and weekly training sessions (1-7) were described.
Characteristics of the Eligible Studies.

Note: Abbreviations: C, control group; I, intervention group; MCI, Mild Cognitive Impairment.
Quality Assessment
Table 2 summarizes the results of the methodological quality of the included trials. The quality of the eligible trials varied from fair to good, with a score range of 3 to 9 points, and the average PEDro score was 6.49. Of the 45 studies, 28 studies classified as excellent or good, which represented low-risk bias and 16 studies as fair quality, which represented moderate-risk bias. Of the studies, three controlled trials did not use randomization. Furthermore, 18 controlled trial employed allocation concealment. Only 1 study reported therapist blinding and 21 studies reported blinding assessors, respectively.
Quality Assessment of the Included Studies (n = 37).

Efficacy of Mind Body Exercises on Each Cognitive Domain
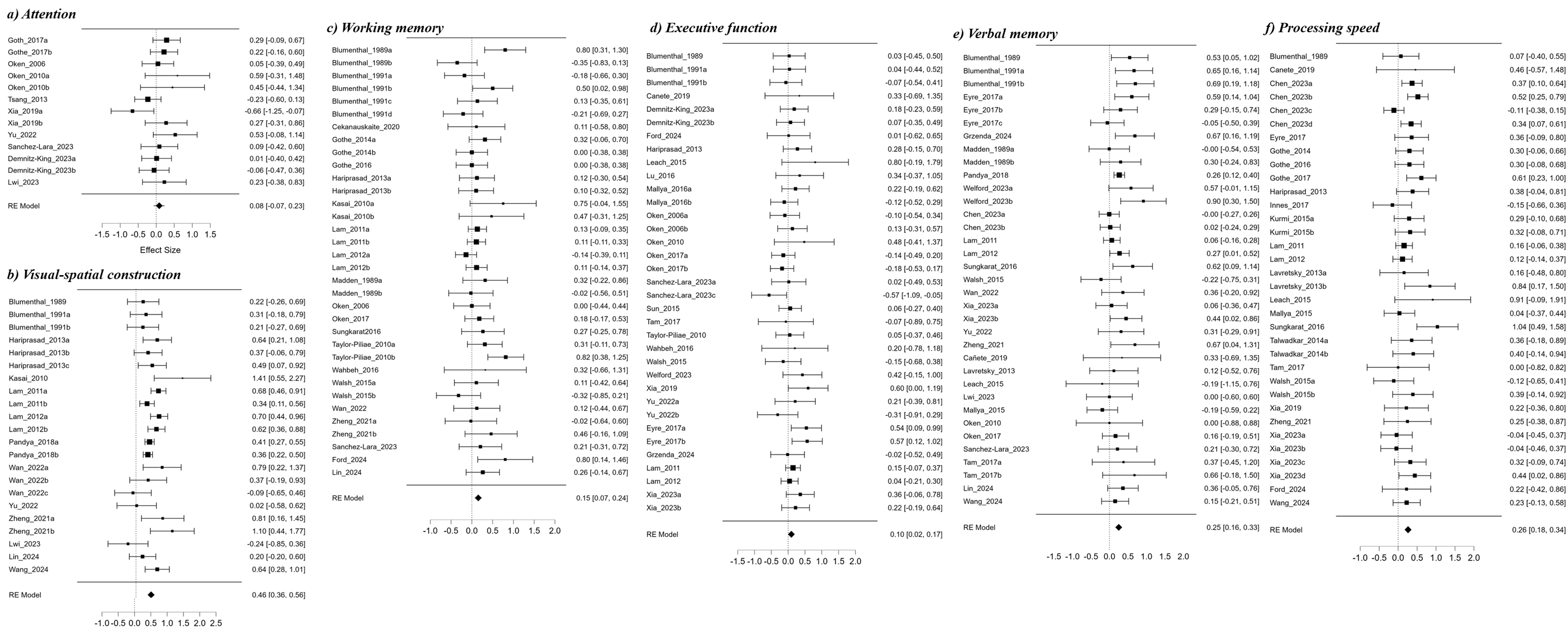
The Result of Meta-analysis in Each Cognitive Domain. a) attention, b) visual spatial construction, c) working memory, d) executive function, e) verbal memory, and f) processing speed.
Summary of the Meta-analysis Results.

Additionally, the meta-regression analysis indicated that none of the moderators had a statistically significant impact on effect size. Specifically, MBE period in weeks did not significantly impact attention outcomes (Estimate = −0.01, p = 0.20). Similarly, the duration of each session in minutes showed no significant effect on the results (Estimate = 0.00, p = 0.60). The frequency of sessions per week also did not significantly influence attention outcomes (Estimate = 0.09, p = 0.27). Participant type was analyzed with MCI participants compared to healthy participants as the reference group, showing no significant difference (Estimate = −0.30, p = 0.21). For intervention type, both Taichi (Estimate = −0.28, p = 0.11) and Qigong (Estimate = −0.10, p = 0.55) had no statistically significant differences in comparison to Yoga, which was the reference group. When looking at control type, exercise as a control was borderline significant (Estimate = 0.31, p = 0.07) compared to no intervention, while other control types showed a similar effect but were not statistically significant (Estimate = 0.31, p = 0.11) (Table S1).
The meta-regression analysis for visual-spatial construction showed that the MBE period (in weeks) did not have a significant effect on outcomes (Estimate = −2.91e-4, p = 0.59). However, the duration of each session (in minutes) had a significant negative effect on visual-spatial construction outcomes (Estimate = −0.00, p = 0.03) suggesting that longer session durations had a statistically significant but minimal negative impact on visual-spatial construction. Frequency of sessions per week did not significantly influence outcomes (Estimate = 0.04, p = 0.35). For participant type, MCI participants showed significantly better improvement in visual-spatial construction compared to healthy participants (Estimate = 0.24, p = 0.00). Regarding intervention type, meditation was the reference group, and both Taichi (Estimate = 0.76, p = 0.23) and Qigong (Estimate = 0.63, p = 0.06) showed moderate positive effects, with Yoga showing the highest effect (Estimate = 0.80, p = 0.02). In terms of control type, exercise (Estimate = 0.13, p = 0.17) and other controls (Estimate = −0.22, p = 0.11) did not show significant differences compared to no intervention (Table S1).
Since participant type, intervention type, and control type were identified as significant moderators in the meta-regression, subgroup meta-analyses were conducted to explore the differences in intervention effectiveness based on these moderators (Table S1). Figure S2 shows the results of a subgroup meta-analysis on visual-spatial construction, focusing on two participant characteristics: a) healthy older adults and b) individuals with MCI. For the healthy older adults, the overall effect size was moderate at 0.36 [0.28 to 0.45], indicating a positive impact of the intervention. In contrast, the MCI group demonstrated a larger effect size of 0.61 [0.45 to 0.77], suggesting that the intervention was more beneficial for participants with MCI.
The Figure S3 displays the effects of different control types on visual-spatial construction. Studies with “no intervention” show a moderate positive effect, with a pooled effect size of 0.41 [0.33 to 0.50]. In contrast, studies where “exercise” was used as the control demonstrate a stronger positive effect, with a pooled effect size of 0.56 [0.40 to 0.72]. Lastly, studies utilizing other control types exhibit a smaller, non-significant effect on visual-spatial construction, with a pooled effect size of 0.21 [−0.25 to 0.67]. This indicates that MBE interventions show a larger effect size when compared to “no Intervention” and “exercise” controls, but the effect size is smaller and non-significant compared to other control type.
The Figure S4 represents the effects of different MBE types on visual-spatial construction. Studies using “yoga” interventions show a moderate positive effect, with a pooled effect size of 0.39 [0.30, 0.47]. In contrast, studies using “tai chi” interventions demonstrate a stronger positive effect, with a pooled effect size of 0.56 [0.38, 0.75]. Studies using “qigong” interventions also show a significant positive effect, with a pooled effect size of 0.51 [0.20, 0.82]. Lastly, studies using “meditation” exhibit a smaller and non-significant effect on cognitive function, with a pooled effect size of −0.24 [−0.85, 0.36].
The meta-regression analysis in Table S1 indicated that neither intervention period (Estimate = −0.00, p = 0.67) nor session frequency (Estimate = −0.01, p = 0.74) had a significant effect on working memory outcomes. Additionally, duration (Estimate = 0.00, p = 0.39) and participant type (MCI vs Healthy; Estimate = −0.02, p = 0.81) did not significantly impact the outcomes. Among intervention types, none of the comparisons (Yoga: Estimate = −0.11, p = 0.54; Taichi: Estimate = −0.13, p = 0.60; Qigong: Estimate = −0.22, p = 0.20) showed statistically significant effects compared to meditation. Similarly, control types (Exercise: Estimate = −1.30e-4, p = 0.99; Others: Estimate = 0.17, p = 0.28) did not differ significantly from no intervention. Overall, no significant moderators were identified for working memory outcomes. Overall, no significant moderators were identified in this analysis.
The meta-regression analysis showed that the MBE period (Estimate = 0.00, p = 0.35) did not significantly impact executive function. Similarly, neither the duration of each session (Estimate = −3.83*10^−4, p = 0.74) nor the frequency of sessions (Estimate = −0.03, p = 0.16) had a significant effect on executive function. However, participant type was a significant moderator, with MCI participants showing greater improvement compared to healthy participants (Estimate = 0.16, p = 0.04). Among intervention types, Taichi (Estimate = 0.35, p = 0.02) showed a significant positive effect compared to Meditation, while Yoga (Estimate = 0.07, p = 0.43) and Qigong (Estimate = 0.19, p = 0.07) had a marginally non-significant positive effect. Control types, including exercise (Estimate = 0.08, p = 0.40) and other controls (Estimate = 0.11, p = 0.30), did not differ significantly from no intervention. These results suggest that MCI participants and Taichi interventions are associated with greater improvements in executive function.
As participant type was identified as a significant moderator in the meta-regression, a subgroup meta-analysis was conducted to investigate the differences in intervention effectiveness based on this moderator (Table S1). The subgroup meta-analysis revealed that the intervention had a small and statistically significant effect on executive function in participants with MCI, with an effect size of 0.22 (95% CI: 0.07 to 0.37, p = 0.00) with low heterogeneity (I2 = 19.717%). In contrast, the intervention had a non-significant effect on executive function in healthy participants, with an effect size of 0.04 (95% CI: −0.05 to 0.13, p = 0.40). The heterogeneity for this group was zero (I2 = 0.00%), suggesting no variability among the study results (Figure S5).
The meta-regression analysis revealed that neither MBE period (Estimate = −1.08*10^−4, p = 0.87) nor participant type (MCI vs Healthy; Estimate = −0.04, p = 0.62) significantly impacted verbal memory outcomes. Additionally, session duration (Estimate = −0.00, p = 0.26) and frequency (Estimate = −0.02, p = 0.64) also had no significant effects. Among intervention types, both Taichi (Estimate = 0.18, p = 0.21) and Qigong (Estimate = 0.28, p = 0.02) showed significant positive effects compared to Meditation. Yoga showed a smaller, non-significant effect (Estimate = 0.03, p = 0.83). Control types, including Exercise (Estimate = 0.08, p = 0.43) and Other controls (Estimate = 0.13, p = 0.26), did not differ significantly from no intervention.
The subgroup meta-analysis showed that Yoga had the most substantial effect on verbal memory with an effect size of 0.41 (95% CI: 0.25 to 0.56), indicating a moderate and statistically significant improvement. Taichi demonstrated a smaller yet statistically significant effect size of 0.12 (95% CI: 0.00 to 0.25). Qigong also showed a moderate effect with an effect size of 0.28 (95% CI: 0.09 to 0.47), which was statistically significant. In contrast, Meditation had a small and non-significant effect on verbal memory, with an effect size of 0.10 (95% CI: −0.09 to 0.28) (Figure S6).
The meta-regression analysis showed that neither MBE period (Estimate = −0.01, p = 0.19) nor session duration (Estimate = −4.38e-4, p = 0.81) significantly impacted processing speed outcomes. Session frequency (Estimate = 0.01, p = 0.74) and participant type (MCI vs Healthy; Estimate = −0.07, p = 0.41) also showed no significant effects on processing speed. Among intervention types, Yoga (Estimate = 0.02, p = 0.86) and Qigong (Estimate = 0.12, p = 0.39) showed small, non-significant effects compared to Meditation, while Taichi had a negative, non-significant effect (Estimate = −0.05, p = 0.74). Control types, including Exercise (Estimate = 0.01, p = 0.87) and other control types (Estimate = 0.16, p = 0.26), did not significantly differ from no intervention. These findings suggest that none of the examined moderators significantly influenced processing speed improvements.
Discussion
This meta-analysis assessed the efficacy of the four most used types of MBE on specific cognitive functioning in older individuals with or without MCI. The findings suggested that MBE intervention had the potential to ameliorate cognitive function and decelerate the progression of MCI towards dementia. The intervention efficacy of MBE on various cognitive domains exhibited varied magnitudes, and ranged from small to moderate. The effect sizes in visual-spatial construction, processing speed, verbal memory, executive function, and working memory were Hedges’ g = 0.48, 0.26, 0.25, 0.10, and 0.15, respectively. A positive trend was observed in the attention domain; however, it did not reach statistical significance. Our findings supported previous findings that MBE interventions enhanced overall cognitive function in older people with small and moderate effects.3,8,9
Cognitive functions can be categorized into six main areas based on their inherent properties. Verbal memory was an individual's capacity to retain and recall previously acquired knowledge presented in written or spoken forms. Age-related decline in verbal working memory was associated with reduced phonological capacities. 47 Visual-spatial ability referred to the cognitive ability to perceive and process information linked to planar and three-dimensional spaces and exhibited an age-related loss. Attention was a cognitive function that involved the rapid processing of information, and becomes more limited as individuals aged. 48 Executive function referred to a complex concept conceptualized in various contexts. It encompassed various of cognitive processes at a higher level, such as planning, directing and sustaining attention, organizing, abstract reasoning and problem-solving, self-regulation, and motor control. 49 Working memory encompassed the cognitive processes of encoding, retaining, and retrieving information. There was a significant correlation between memory loss and dementia in older adults with normal cognitive functioning. 50 Processing speed was the ability to describe how the brain received, understood, and responded to information. Processing speed decline commonly occurred in otherwise healthy, normal individuals who showed no signs of neurodegenerative disease, which subsequently resulted in functional impairment and other morbidities. 51
Previous studies suggested plausible hypotheses to explain the beneficial impact of MBE on cognitive functions in the older adults. 9 Mind-body exercises emphasized the profound link between the body and mind via coordinated body movements, rhythmic respiration, awareness of feelings, and weight shifting.52,53 MBE demanded skill-related learning processing, which included memorization or imitation, and activated certain regions of the brain, such as cingulate cortex, hippocampus, frontal lobe, and sensorimotor cortex.54-57 Furthermore, data indicated that engaging in physical exercise led to an increase in inflammatory biomarkers (ie, brain-derived neurotrophic and tumor necrosis factors) which played crucial roles in enhancing cognitive performance.58,59
Several studies contributed to a further comprehensive understanding of the mechanical and molecular underpinnings by which MBE enhanced cognitive performance. According to Silva et al (2024), physical exercise positively affects cognition and brain health by improving neuroplasticity, cerebral blood flow, and synaptic connections. These mechanisms contribute to better cognitive function, particularly in attention, memory, and executive function. 60 Raichlen & Alexander (2017) propose an evolutionary neuroscience model linking exercise to improved cognitive abilities, arguing that the human brain has evolved to benefit from physical activity. 61 Exercise enhances the brain's adaptive capacity, which is critical for tasks requiring executive function and memory. They also suggest that exercise, particularly aerobic activities, leads to enhanced cognitive resilience in aging. 62 Further supporting these findings, research highlights the link between exercise, dopamine regulation, and cognitive enhancement, particularly in older adults. Dopamine, which plays a critical role in motivation and cognitive processing, is positively influenced by physical activity, potentially explaining the cognitive benefits observed in various tasks. 63 Recently, Stillman et al (2020) suggested that exercise slows cognitive decline in older adults through three distinct mechanisms at cellular, brain, and psychological levels. 64 At the cellular level, exercise stimulates the release of neurotrophic factors such as BDNF, NGF, and IGF-1, which support neuronal growth, synaptic plasticity, and long-term potentiation (LTP), all critical for memory and learning. At the brain level, physical activity leads to structural changes, including increased gray and white matter volumes, particularly in the hippocampus, which is essential for memory. Additionally, exercise enhances the thickness of the cerebral cortex, associated with higher-order cognitive functions. Finally, at the psychological level, exercise reduces stress, depression, and anxiety, fostering an improved mood and mental state that further supports cognitive health and reduces the risk of cognitive decline. 64 In conclusion, physical exercise enhances cognitive function by fostering brain plasticity, improving neurochemical balances, and supporting better functional connectivity across brain regions. These findings support the idea that exercise is a low-risk, non-invasive intervention to promote brain health across the lifespan, which can be applied to mind-body exercises such as MBE.
Specifically, the synthesized results indicated a moderate effect only in visual-spatial construction, which suggested that MBE could be more effective in enhancing visual-spatial construction than other cognitive domains. These findings were consistent with previous research on the efficacy of MBE interventions for visual-spatial construction in healthy older adults and persons with or without MCI.8,65,66
In contrast to other research findings, this study did not observe a statistically significant impact on attention. 8 Additionally, the sub-analyses in the attention domain showed that the efficacy of MBE was the opposite in both groups (it decreased in the MCI group and increased in the healthy group), although it was not significant. The insignificant efficacy and heterogeneity between the two groups on attention in our findings could be attributed to the inclusion of a small number of effect sizes (only 13 controlled trials in nine studies), which may not adequately capture the real effect.
The meta-regression analysis results show that in certain cognitive domains, such as visual-spatial construction and executive function, participants with MCI exhibited a significantly larger effect compared to healthy participants (Table S1). Specifically, for visual-spatial construction, MCI participants showed a larger improvement (Estimate = 0.24, p = 0.00), and for executive function, they demonstrated a similarly larger improvement (Estimate = 0.16, p = 0.04). This may be because individuals with MCI are more likely to experience noticeable benefits from cognitive interventions due to their initial deficits. The meta-regression findings align with previous literature suggesting that cognitive interventions, such as exercise, may have a more pronounced impact on populations with greater cognitive decline. Recent research compared the effects of physical exercise on cognitive function in both healthy older adults and individuals MCI. 67 This research found that while exercise interventions had some beneficial effects on cognitive functioning in healthy older adults, the evidence was mixed, with some analyses showing significant improvements and others not. In contrast, individuals with MCI showed more consistent and significant improvements in overall cognitive function due to exercise interventions, with effect sizes ranging from g = 0.25 to 0.57. Populations with more cognitive vulnerability, such as those with MCI, likely benefit more from interventions as there is more room for improvement in these groups. 67 In summary, the results highlight that MCI participants tend to benefit more from MBE in specific domains such as visual-spatial construction and executive function, which could be because these individuals experience more cognitive deficits, and thus, greater potential gains from intervention.
In addition to the characteristics of the participants, we investigated whether the frequency or duration of the intervention influenced the effects of MBE on cognitive outcomes. Meta-regression analyses revealed that the total duration of the intervention (measured in weeks), the length of each session (in minutes), and the frequency of sessions per week did not have a significant impact on cognitive outcomes across all six domains (Table S1). The results indicate that differences in the amount of exercise do not significantly explain the variations in effect sizes observed. In order to gain a deeper understanding of this relationship, we performed subgroup analyses categorized by the frequency and duration of the interventions. The frequency was categorized into two groups for five cognitive domains (executive function, verbal memory, working memory, visual-spatial construction, and processing speed): those participating in three or fewer sessions per week and those engaging in four or more sessions per week (Table 1, Figure S9-S18). For the attention domain, studies were categorized as 1–2 sessions/week versus 3 sessions/week, as no study reported a frequency of ≥4 sessions/week (Table 1, Figure S7 and S8). The duration of the intervention was consistently classified as 12 weeks or less compared to more than 12 weeks across all domains. The findings aligned with the meta-regression results, indicating that there were no significant differences in cognitive outcomes among the various frequency and duration subgroups (Figures S7–S18). The consistent findings across various analytical methods suggest that the cognitive advantages associated with MBE do not significantly depend on the dosage. This implies that even programs with lower frequency or shorter duration could provide similar cognitive benefits. The results underscore the practical benefits of adopting MBE with a degree of flexibility, especially in contexts that include older adults who may have differing levels of availability, mobility, or physical capability.
Additionally, the meta-regression analysis revealed that interventions like yoga, qigong, and tai chi demonstrated significantly greater effects on visuospatial construction and verbal memory compared to meditation as shown in the Table S1. This could be attributed to the fact that meditation, unlike other interventions, is a sedentary behavior. Recent researches have shown that sedentary behavior negatively impacts biological aging and contributes to health issues such as chronic inflammation, which is a known risk factor for cognitive decline.68-70 Falck et al (2017) found that sedentary behavior is closely linked to cognitive decline, particularly in older adults, with prolonged sitting being associated with impairments in memory, attention, and executive function. 68 Sjögren et al (2014) further highlighted the detrimental effects of sedentary behavior on health by connecting it to biological aging and emphasizing the importance of reducing sedentary time for maintaining cognitive health. 69 Voss et al (2014) discussed how sedentary behavior can lead to chronic inflammation, which in turn increases the risk of cognitive decline. 70
Specifically, the results of the meta-regression for visual-spatial construction show that both Taichi and Yoga exhibited stronger effects compared to the reference intervention, meditation, as shown in the Table S1. Yoga had the highest positive impact on visual-spatial construction (Estimate = 0.80, p = 0.02), followed by Tai chi (Estimate = 0.76, p = 0.23), and Qigong (Estimate = 0.63, p = 0.06), though the latter two were not statistically significant. A possible explanation for this improvement in visual-spatial construction relates to the characteristics of these MBE exercises. Unlike meditation, which is often associated with sedentary behavior, MBEs like yoga, Tai chi and Qigong impose considerable cognitive demands on spatial processing. 71 Enhanced visuo-spatial construction could be attributed to the characteristics of MBE, since it placed significant cognitive demands on spatial processing. 71 Engaging in them enhanced the sensitivity of tactile and proprioceptive sensations,72,73 both of which had positive correlations with visuo-spatial abilities. 74 Additionally, they incorporated upper-body motions reinforced by the lower extremities to sustain postural stability akin to goal-directed upper-body motions. 71 Hence, Yoga, Qigong and Tai chi may have a stronger influence on visuo-spatial ability in goal-directed upper-body motions than other interventions like meditation. This assertion was supported by empirical evidence that indicated that engagement in Tai chi and Qigong activated the parietal lobe, an area of the brain closely associated with spatial processing.13,75,76
Our finding found that MBE like yoga, tai chi, and qigong significantly improved cognitive domains, particularly visuospatial construction, and verbal memory, with larger effects observed in individuals with MCI compared to healthy participants. MCI participants exhibited greater improvements in both visuospatial construction (Estimate = 0.24, p = 0.00) and executive function (Estimate = 0.16, p = 0.04), likely due to their initial cognitive deficits providing more room for improvement. In contrast, meditation, a sedentary behavior, demonstrated smaller effects on cognitive functions. Recent studies suggest that sedentary behavior contributes to cognitive decline through chronic inflammation and biological aging, making active MBE more beneficial. Yoga, tai chi, and qigong impose cognitive demands on spatial processing, enhancing visuospatial abilities by engaging tactile and proprioceptive sensations. These findings suggest that active MBEs are a low-risk, effective intervention for improving cognitive function, particularly in older adults with MCI.
This study has several limitations that warrant consideration. First, the utilization of multiple assessment tools to test the same cognitive domain for comparison with MBE intervention posed challenges in interpreting the findings of the meta-analysis. Second, the search strategy used was restricted to articles published in English. Consequently, it was important to acknowledge the possibility of language bias. Third, we excluded studies with cross-sectional and one-group pretest-posttest designs, as they may have only offered a partial explanation for the relationship between cognitive improvements and MBE interventions. Fourth, there was moderate heterogeneity in some cognitive domains, such as verbal memory, working memory and visual-spatial construction, which suggests variability in study designs, participant characteristics, or intervention protocols. Fifth, other limitation is the lack of standardized, validated modules for MBE interventions across the included studies, which may affect the consistency of results. Additionally, the absence of long-term follow-up assessments limits the ability to determine the sustained effects of MBE on cognitive function. Finally, although this meta-analysis examined various MBE interventions for cognition, it failed to consider various factors, such as the participants’ psychological status, presence of current medication, and participants’ gender and ratios. Future research should address these gaps to establish more conclusive findings.
The main strength of this meta-analysis was that a relatively large number of researches, which adheres to rigorous and robust methodological standards were included to assess the efficacy of MBE in enhancing cognitive functioning among the aged population. The results indicated that MBE could be efficacious in improving cognitive function among older people with or without MCI. The results may offer clinicians empirical data to support their decision making regarding the potential cognitive advantages of MBE for older people with or without MCI. Nevertheless, methodological constraints and the limited number of studies hindered the ability to definitively establish the potential advantages of MBI interventions on older adults’ cognitive function and mental well-being. In addition, our review recommended the implementation of additional randomized controlled studies that adhered to standardized research procedures. It also suggested the utilization of validated modules for MBE intervention and inclusion of long-term follow-up assessments to establish conclusive findings.
Supplemental Material
sj-docx-1-chp-10.1177_2515690X251363709 - Supplemental material for A Meta-Analysis of Studies of the Effect of Mind Body Exercise on Various Domains of Cognitive Function in Older People With or Without Mild Cognitive Impairment
Supplemental material, sj-docx-1-chp-10.1177_2515690X251363709 for A Meta-Analysis of Studies of the Effect of Mind Body Exercise on Various Domains of Cognitive Function in Older People With or Without Mild Cognitive Impairment by Ji-Woo Suk, Kahye Kim and Jaeuk U. Kim in Journal of Evidence-Based Integrative Medicine
Footnotes
Authors’ Contributions
The authors confirm contribution to the paper as follows: study conception and design: J-WS and JUK; data collection: J-WS and KK; analysis and interpretation of results: J-WS and JUK; draft manuscript preparation: J-WS and KK. All authors reviewed the results and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grant number (KSN2313022) from the Korea Institute of Oriental Medicine and by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (RS-2023-KH138802).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Informed Consent
Not applicable. This study did not involve human participants.
Trial Registration
Not applicable. This study is a systematic review and was not registered as a clinical trial.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.