
Abstract
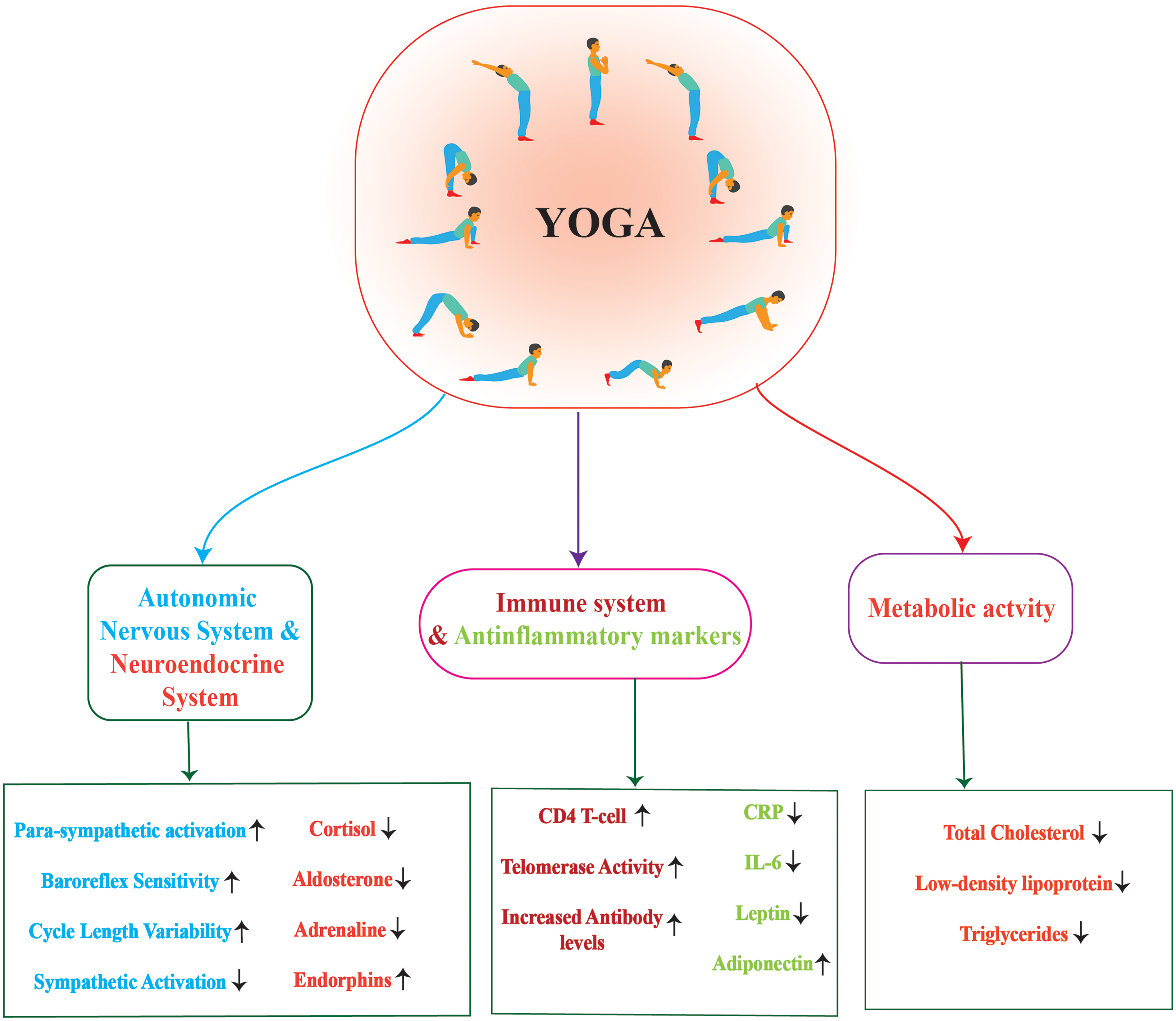
Modifiable and non-modifiable risk factors in Type 2 Diabetes (T2D) contribute to chronic inflammation characterized by elevated pro-inflammatory mediators and constitutively activated immune cells. Chronic inflammation in T2D leads to perturbations in metabolism, resulting in altered immuno-metabolic axis and further vascular complications. Hence, reducing inflammation by targeting modifiable risk factors such as adiposity, sedentary lifestyle and psychological stress in T2D may facilitate efficient clinical management. Yoga has been shown to improve glucose metabolism, reduce psychological stress, and decrease obesity, hence we sought to review the role of Yoga on cellular mechanisms regulating the immuno-metabolic axis in T2D. Elevated levels of inflammatory mediators such as IL-1b, IL-6, TNF-a, and CRP contributing to insulin resistance are reduced upon practicing Surya Namaskara, Pranayama, and meditation and further improved glycemic index in T2D individuals. Specific Asanas and Pranayama significantly decreased adipokines including leptin, adiponectin, and vaspin in subjects with high BMI, triglycerides and HOMA-IR values, and concomitantly reduced inflammation. Bidirectional activation of inflammatory mediators and stress hormones including epinephrine, catecholamines and cortisol manifesting in diabetes are also reduced upon practising meditation and Yoga. Yoga practices such as Pranayama, Asanas and Mudras improve insulin sensitivity, contribute to weight management, mitigate stress levels in T2D, and maintain immuno-metabolic homeostasis.
Introduction
Type 2 Diabetes (T2D) is multi-genic and complex metabolic disorder associated with chronic and low grade inflammation characterized by increased pro-inflammatory mediators contribute to a) reduced insulin production upon decreasing β-cell mass and b) simultaneously induce insulin resistance in various tissue types, c) recurrent infections due to constitutive activation of immune cells and d) vascular complications. Over the years, studies have demonstrated that glucose induced constitutive activation of mediators of the innate and adaptive immune system plays an important role in the pathogenesis of aforesaid morbidities. On the other hand, T2D is also associated with metabolic reprogramming at both systemic and tissue/organ levels. Progressive alterations in organ specific metabolites in T2D influence chronic activation of immune system which leads to perturbed immuno-metabolic axis. Pre-clinical and clinical studies have demonstrated that inflammatory mediators disrupt insulin signalling in various insulin responsive tissues such as adipose, muscle and endothelial cells causing insulin resistance in T2D.1,2 Inhibitors of NF-κβ, JNK, and NLPR3 inflammasome activation cause serine phosphorylation of IRS1 resulting in its degradation and leading to reduced insulin sensitivity. 3 On the other hand, FFA, macrophage and neutrophil infiltration inflammasome/IL-1β signalling, and inflammation within pancreatic beta cells contribute to decreased beta cell mass and functions.4–7 Further, IL-1β, IL-6, TNF-α and CRP are released into the circulation and cause metabolic inflammation which leads to perturbed metabolism in various tissues that results in disrupted immuno-metabolic axis. Studies have also established how constitutive and low grade activation of innate immune cells in T2D will contribute to recurrent infections and vascular pathologies.1,8
Various modifiable (obesity, sedentary life style and mental stress) and non-modifiable (genetic and epigenetic) factors in T2D contribute to excess inflammatory milieu. For example, insulin resistance is influenced by obesity and the accumulation of excess fat in the liver and other tissues. Insulin resistance and chronic low-grade inflammation are both exacerbated by adipokines and inflammatory markers released by adipose tissue in obese individuals. 9 Sedentary life style leading to increased adiposity also contributes to elevated levels of inflammatory mediators. Similarly, another modifiable risk factor of T2D, chronic stress adversely affects lipid and glucose metabolism and thereby increases the production of stress hormones and induces hyper activation of immune cells that cause a surge of pro-inflammatory cytokines and concomitantly results in insulin resistance. Glucocorticoids and catecholamines regulate the stress system, which involves the peripheral and central neural systems and affects glucose homeostasis upon chronic stimulation and further induces inflammation. 10 Taken together, improving modifiable risk factors such as adiposity, sedentary lifestyle and psychological stress significantly ameliorate inflammatory conditions and promote beneficial effects on metabolism in T2D.Top of Form
Physical activity is an essential part of managing diabetes and has many advantages, including reduced inflammation and oxidative stress, improved insulin sensitivity, BMI and quality of life. 7 The production of anti-inflammatory cytokines, such as IL-4, is stimulated by exercise while decreasing pro-inflammatory mediators such as IL1- β, IL-6,TNF- α, IL-18 and CRP which are associated with T2D complications. 11 Yoga, an ancient Indian form of composite lifestyle intervention that includes physical activity, breath regulation, relaxation, and meditation has been shown to exert beneficial effects on reducing adiposity, and stress and reversing the adverse effects of a sedentary lifestyle in the context of T2D. Several independent studies have shown that Yoga practice improves metabolism and inflammatory conditions in various diseases, including T2D. Similarly, a non-randomized study of 86 participants reported that a 10-day holistic yoga program increased β-endorphins and decreased IL-6 and TNF-α, suggesting improved inflammatory regulation, though the specific effects of yoga were confounded by other intervention components such as stress management and group discussions. 12 This suggests that practicing Yoga facilitates the restoration of immuno-metabolic homeostasis in T2D by reducing inflammation, adiposity and stress hormones. However, all these modifiable factors exert and manifest inflammation via distinct signalling pathways. Hence, we hypothesize that practicing a set of Yoga techniques targeting specific modifiable risk factors (adiposity, stress or diet) and induced inflammation may benefit patients. The beneficial effect of Yoga on regulating several indices of T2D management such as glycemic control, lipid profile and body mass index are known. 13 Understanding how specific yoga techniques influence each biological mechanism associated with adiposity, stress, and inflammation is crucial for T2D management in the clinical setup, which is still under investigation. Potential evidence supporting the universal applicability of yoga is another concern due to the limited diversity of demographic groups studied, as many studies focused on specific populations. The lack of data supporting whether yoga can slow down, or reverse diabetic complications also needs to be resolved. Hence, in the present review based on mounting evidence and seminal findings, we describe a) examine if modifiable risk factors manifest in chronic inflammation using distinct pathways; b) role of Yoga in reducing effects of these risk factors on chronic inflammation and maintaining metabolic homeostasis.
Yoga Practise Improves T2D Associated Chronic Inflammation
Inflammatory signalling in T2D such as JNK and IKKβ/NF-κβ pathways are activated in insulin responsive tissues including adipocytes, hepatocytes, skeletal muscle, endothelial cells and macrophages in response to obesity and high-fat diets. 2 Elevated levels of TNF-α, IL-1β, or AGE bind to their receptors such as TNFR, IL-1R, or RAGE respectively and induce ER stress and ROS resulting JNK and IKKβ/NF-κβ activation in metabolic dysregulation. 14 IKKβ activation due to obesity increases NF-κβ translocation and concomitant expression of several indicators and possible mediators of inflammation that result in insulin resistance. This also causes JNK activation in obese individuals and stimulates IRS-1 phosphorylation at serine sites specifically on serine-302, serine-307, serine-636, and serine-639, causing proteasomal degradation of insulin receptor/IRS-1. 2 Studies also showed that IL-1β reduces the levels of IRS-1 by decreasing transcription of IRS-1 mRNA levels, which leads to reduced glucose uptake in adipocytes. 15 Rodent model of IL-1α-/- reduced fasting glucose levels and improved overall insulin sensitivity when compared to wild type. 16 IL-1β together with IL-6 levels are often considered as the best predictors for T2D, compared to other cytokines. 17 Resistin is another cytokine mainly produced by adipocytes and immune cells including macrophages which have reportedly been involved in inducing insulin resistance. Resistin activates intracellular signalling via NF-κβ pathway which further induces the generation of several other cytokines including TNF-α, MCP-1, IL-6, IL-12, ICAM and VCAM.18–21 NF-κβ activation in the adipose tissue due to the chronic hyperglycaemia and the AGEs that are produced in excess. 22 Free fatty acids, hyperglycaemia, PKC activators, and oxidants are examples of non-inflammatory cell/cytokine-mediated factors that activate NF-κβ leads to translocation into the nucleus, promote transcription of genes responsible for the development of insulin resistance.2,23 Hyperglycaemia mediated upregulation of NADPH during the activation of PKC and NF-κβ promotes the overexpression of the NADPH enzyme. Further authors showed hyperglycaemia and elevated levels of FFA contribute to the increased production of superoxide at the mitochondrial level and nitric oxide via NOS. 24
This brief overview of tissue specific inflammatory events in T2D and associated consequences instigates us to investigate how practicing Yoga exerts beneficial effects on the constitutive activation of the immune system. In the most recent studies, the beneficial effects of Hata Yoga on cortisol levels, and conventional measures of inflammation such as IL-1β, IL-6, CRP, INF-γ and TNF-ɑ, are demonstrated. Additionally, Hata Yoga also improves BDNF, telomerase activity, endorphins, and IgA levels. 12 The benefits of Yoga are frequently studied in older populations and people with immune function dysregulation by incorporating standard Yoga practice involving Shithilikarna vyayama (Loosening exercises), Surya Namaskara, Yogic poses, pranayama (Breathing practice) and Dhyana (Meditation). A study was conducted to evaluate Hata Yoga-based intervention in reducing inflammation and stress in subjects with chronic disease and overweight/ obesity (44 female and 42 males; age 40.07 ± 13.9) were introduced for physical Yoga postures followed by breathing exercises (Pranayama) for one hour. Results showed that plasma IL-6 levels were reduced compared with the baseline (P = .036) in males but not in females and interestingly, TNF-ɑ was reduced in females. 25 A study involving 14 elderly women (Control group, n = 7 and Yoga group, n = 7) aged between 70-80 practicing Hatha Yoga for ten weeks showed a significant increase in albumin and a declined level of fibrinogen, hs-CRP and ESR. 26
Yoga has many health benefits in preventing and controlling hyperglycaemia. A prospective-based randomized study was conducted on diabetic subjects for 24 weeks (n = 104). Participants engaged in 40-min Yoga sessions five days a week (Multifaceted individualised yoga). Following the intervention, there were notable changes in various parameters: Body mass index (25.6 ± 2.9 vs 28.0 ± 3.2 kg/m2), waist–hip ratio (0.94 ± 0.06 vs 0.99 ± 0.05), glycated hemoglobin (7.2 ± 1.8 vs 9.4 ± 1.9%), IL-6 (32.0 ± 21.5 vs 43.5 ± 34.3 pg/mL), and hs-CRP (5.1 ± 3.7 vs 9.5 ± 15.6 mg/L) (P ≤ .05). HDL cholesterol (49.2 ± 15.0 vs 40.4 ± 7.2 mg/dL) and higher serum total antioxidants (1.9 ± 0.4 vs 1.4 ± 0.4 mmol/L) were also seen in the intervention group (P < .001), suggesting that short-term Yoga intervention may reduce glycaemic index and inflammatory markers. 27 Similarly, another study was conducted where T2D subjects were randomly assigned for Yoga intervention for 3 months (Yoga group = 150, non-Yoga group = 150). BMI, HbA1c, blood glucose, lipid levels, IL-6, TNFα, and TBARS levels were significantly reduced in Yoga group. 28 Moreover, subjects who practiced Yogasana showed notable changes in PTGIS, adiponectin, and sleep quality. These findings imply that regular Yogasana practice may be effective as an adjuvant therapy for T2D management. 29 Substantial improvements in total cholesterol, triglycerides, fasting plasma glucose, postprandial blood sugar, LDL, and VLDL, along with an increase in HDL, were found in a separate 12-week yogic intervention study involving elderly women with T2D (n = 20; Yoga group:10, control: 10). This indicated that elderly women with T2D may benefit from Yoga intervention in terms of their lipid profiles and blood sugar levels. 30 Additionally, 31 reviewed and introduced a novel Yoga program for T2D prevention (YOGA-DP) among high-risk people in India. This study suggests that Practicing Yoga (combining techniques like Dhyana, Pranayama, Asana, Surya Namaskar, and Shithilikarna Vyayama) for a duration of 24 weeks will help in prevention of T2D. 31 Taken together, all these studies demonstrated Yoga exerts beneficial effects on improving glycaemic index and thereby reducing inflammation in T2D (Figure 1).

Yoga improves high glucose induced inflammation: Activated JNK and NF-κβ triggers the serine phosphorylation of IRS, inducing insulin resistance affecting both glucose uptake and fatty acid oxidation. On the other hand, the expansion of adipose tissue reduces oxygen availability, leading to hypoxia. This hypoxia activates HIF-1ɑ, which in turn stimulates the transcription of genes related to apoptosis, VEGF, GLUT, and PAI-1. Consequently, this inhibits adipocytes from secreting anti-inflammatory adipokines, contributing to insulin resistance. Yoga practice such as Hata yoga consisting of (Surya Namaskara, Pashchimottaanasana, Shashankasana, Ushtrasana, Bhujangasana, Naukasana, Pavanamuktasana, Ardha kati chakrasana, Halasana, Sarvangasana and Shavasana) reduce inflammation by improved insulin resistance and reduced secretion of anti-inflammatory markers.
Yoga in Improving Adiposity and Associated pro-Inflammatory Milieu in T2D
Obesity is the global concern for the development of T2D which is estimated to affect 300 million people by 2025. 32 Over the years, in-vitro, preclinical and clinical studies have demonstrated that adipose tissue plays a significant role in maintaining whole-body metabolic homeostasis due to its critical biological roles as an energy storage reservoir and a key endocrine organ that secretes adipokines including pro and anti-inflammatory chemokines. 33 Hence, the severity of adiposity regulates inflammatory pathways which results in increased insulin resistance and subsequently manifests in T2D. During obesity, the advanced stage of adipose tissue hypertrophy recruits IL-1β secreting pro-inflammatory M1 macrophages due to excess saturated fatty acids. Similarly, Th1 and Th17 cells secrete the TNF-ɑ and IL-17/IL-22 cytokines and induce the recruitment of M1 macrophages to adipose tissue in a purinergic-dependent pathway. 34 Obesity-driven IR is the primary event of T2D development in association with WAT, skeletal muscle and liver. 35 One of the hypotheses linking obesity, insulin resistance and T2D concentrated on elevated FFA flux from the adipose tissue causes insulin insensitivity in the tissues such as liver and muscle due to lipotoxicity/ectopic fat accumulation. 33 Chronically increased FFA levels exert lipotoxicity on the pancreatic β-cell causing dysfunction in obesity, insulin resistance disrupts major signalling pathways including MAPK and PI3 K/AKT, and their interacting with PPARγ and FOXO transcription factors, results in dyslipidaemia and hyperglycaemia. 36 This condition triggers the accumulation of FFA in the liver, alongside insulin-stimulated lipogenesis, resulting in the formation and release of triglycerides. Secretion of pro-inflammatory cytokines such as IL-6 and TNF-α have profound effects on triglyceride synthesis, storage and hydrolysis through the downregulation of PPARγ leads to insulin resistance. TNF-ɑ also inhibits adiponectin and resistin production in obese subjects and promotes insulin resistance due to reduced fat oxidation. 37 The potential mechanism of resistin on the insulin signalling pathway includes resistin stimulated MAP kinase activation and upregulation of the expression of ATP-2, which further stimulated PTEN gene at the promoter region. Overexpression of PTEN resulted in dephosphorylation of PIP3 and blocked IRS-PI3K-PIP3-PDK-Akt signalling pathway. This led to reduced phosphorylation of Akt and PDK. 38 MCP-1 is a cytokine that plays an important role in requirement of macrophages to the site of inflammation in obese conditions. Diet induced insulin resistance ob/ob and db/db mice exhibited increased levels of MCP-1 in adipocytes, Several studies have shown that adipocyte specific expression of MCP-1 alone is sufficient for macrophage requirement and can lead to insulin resistance.39,40 To support this, CCR2-/- developed resistance to obesity induced insulin resistance. 41 Rather than playing a direct role in insulin signalling, MCP-1 plays a vital role by recruiting macrophages and other inflammatory cells to adipocytes while facilitating the secretion of several inflammatory mediators by macrophages and adipocytes.
Elevated CRP levels were associated with obesity, diabetes, smoking and sedentary lifestyle. 42 CRP expression was increased in adipocytes in TNF-α and resistin dependent pathways. 43 CRP also facilitates CVD risk in diabetic patients by increasing the production ICAM-1 and MCP-1 by endothelial cells.44,45 High levels of CRP in obese subjects were reduced by exercise and improvement of insulin sensitivity.46,47 SAA is a group of proteins that are produced in reaction to inflammatory stimuli. Though the predominant manifestation of SAA1 and SAA2 in the liver is well recognized, recent studies have shown that adipocytes were major contributors to SAA1 and SAA2 in humans. 48 Undoubtedly, large adipocytes associated with insulin resistance produce more SAA2 than smaller adipocytes. 49 Increased levels of SAA were measured in individuals with compromised glucose tolerance and T2D. SAA triggers the production of multiple pro-inflammatory mediators such as IL-6, IL-8, MCP-1, and PAI-1 was observed suggesting that it may influence insulin signalling indirectly. Interlukin-8 (IL-8) predominantly produced by macrophages plays an important function in the requirement of neutrophils and lymphocytes to the site of inflammation. 50 Elevated levels of IL-8 were found in obese males. 51 It has been demonstrated that IL-8 may have a direct effect on insulin signalling by inhibiting Akt phosphorylation through ERK or p38 MAP kinase pathway in fully differentiated human adipocytes. 52 SAA, PAI-1, angiotensinogen, and other factors contribute to endothelial dysfunction in T2D through potential pathogenic inflammatory mechanisms. TNF-α, IL-6, MCP-1, visfatin, and PAI-1 levels were highly expressed in activated macrophages and/or other cells of these diabetic subjects with an extensive generation of leptin and adiponectin by adipocytes. 53 These above studies demonstrate activation of various signalling pathways leads to manifestation of constitutive and chronic inflammation in obesity.
Yoga is a mind-body practice which has shown number of health benefits, including improving BMI and exerting beneficial effects on obesity. Practicing Yoga is a useful way to intervene as we explore the complex relationship between adiponectin and obesity, specifically looking at the dynamic interaction between adipose tissue and its effect on metabolic health upon reducing inflammation. Multiple studies have shown the effect of practicing Hata Yoga for a regular period on lowering inflammation in the body by reducing the pro and anti-inflammatory cytokine levels. 12 A randomized controlled trial of a YBLI for 12 weeks comprised of Asanas (Postures), Pranayama (Breathing technique), Shavasana and Meditation (Relaxation technique) significantly reduced the levels of adipokines (leptin, adiponectin, TNF-α, HIL-6), oxidative stress markers (TBARS and 8-OHdG) with an elevation of dismutase (SOD) in the subjects with metabolic syndrome with a characteristic high waist circumference, high triglyceride, and high-density lipoprotein cholesterol levels. 54 A study on obese women found that an 8-month aerobic exercise (AE) program reduced HOMA-IR by 18.9% (P = .012) and upper abdominal fat by 6.2% (P = .021), while a 6-week AE program reduced HOMA-IR by 26.7% (P = .046), but neither benefit was maintained at follow-up (2-4 years later), highlighting the necessity of sustained exercise for long-term metabolic health 55 Contrary to these findings another study for analyzing the HOMA-IR, 34 obese participants were subjected to a short-term Yoga intervention, and parameters such as weight, waist-hip ratio, blood pressure, IL-6, Vitamin D along with the diabetic factors were measured. Interestingly this 10-day intervention showed significant reduction of weight, waist/hip ratio, BMI, IL-6, neopterin, vaspin and diabetic factors such as homeostatic model assessment-insulin resistance, fasting insulin, blood glucose, and lipid profile. 56 In another study conducted on South Korean overweight adolescents (n = 30), a 12-week exercise intervention was given categorizing them into three groups 1) resistance training 2) aerobic training and 3) diet only. Both resistance and aerobic training programs improved insulin sensitivity with reduced muscle mass along with body mass. The dietary intervention failed to show any difference in insulin resistance, but the reduction in muscle mass was low compared to the other two groups. 57 Papp et al,2016 introduced a Hata yoga-based high-intensity Yoga (HIY) intervention consisting of a Suryanamaskara sequence weekly once for six weeks to 54 healthy subjects, and high ApoA1 and adiponectin levels with lower HbA1c levels were observed. 58 A randomized study of novice and female Yoga practitioners was assessed for the effect of Iyengar yoga a part of hatha Yoga on the serum IL-6 and CRP levels, where IL-6 levels were 41% higher in the participants who did not perform Yoga. 59 A clinical trial with a sample size of 19 participants, the levels of IL-6 and CRP were assessed. The trial involved a Hata Yoga therapy intervention (twice weekly for 70 min) and compared it to a control group receiving standard medical therapy over an 8-week program, findings indicated a decrease in IL-6 and CRP levels as a consequence of the Yoga therapy in subjects with chronic heart failure. 60 Multiple studies examined the relationship between the frequency of Iyengar Yoga practicing is inversely corelated with obesity related parameters, including waist circumference, BMI, body fat, LDL, vLDL and triglycerides. 61 Similar studies examined the effects Yoga on obesity suggesting that 6 days Yoga and diet programme resulted in significant improvement in BMI (1.6%), TC (7.7%), HDL cholesterol (8.7%) and fasting serum leptin levels (44.2%). Another intervention studied three months intervention involving Yoga asana and pranayama (n = 50 male) showed decrease in the BMI, Total cholesterol, vLDL, triglycerides and systolic and diastolic blood pressure. 62 A pilot study conducted by Dhananjai and colleagues demonstrated that Vini yoga a type of hata yoga with breathing techniques, specific Yogasana (Pashchimottaanasana, Halasana, Vajrasana and Naukasana) followed by meditation among 56 obese subjects (n = 32 females and n = 24 males) for 12 weeks resulted in significant decrease in weight, BMI, hip and waist circumference, and other anthropometric measurements. 63 ). Furthermore, total cholesterol, triglycerides, LDL, vLDL and fasting glucose all considerably decreased (P < .01), whereas HDL significantly increased. A baseline study of long-term Yoga practitioners (n = 15) and healthy controls (n = 15) concluded that Yoga practice over an extended period is linked to improved insulin sensitivity and a reduction in the adverse correlation between body weight or waist circumference. 64 Taken together, Yoga tends to influence inflammatory markers in obese individuals helping in managing adiposity and promoting metabolic health (Figure 2).

Yoga reduces inflammatory milieu in obese individuals and maintains metabolic homeostasis: In lean adipose tissue, the predominant macrophage population consists of M2 macrophages, fostering increased insulin sensitivity through the secretion of IL-10. The hypertrophy of adipocytes, stemming from excessive eating and sedentary behavior, prompts the release of MCP-1 into the bloodstream, attracting circulating monocytes to adipose tissues. Upon differentiation into activated M1 macrophages, these infiltrating monocytes contribute to a state of mild inflammation in adipose tissue and a decline in adiponectin levels by releasing proinflammatory cytokines like TNFα, IL-6, and MCP-1. Furthermore, these secreted cytokines act as adipokines, inducing insulin resistance and thereby resulting in impaired insulin responsiveness in the liver and skeletal muscle. Thus, by incorporating the specific Yoga practice such as Trikonasana, Halasana, Pashchimottaanasana, Ushtrasana, Naukasana, Shashank asana, Sarvangasana and Dhyana the excess adipokine secretion can be regulated.
Yoga Ameliorates Stress Induced Inflammatory Changes in T2D
Hormonal responses to stress in the acute and chronic phase leads to manifestation of several pathological events including development of T2D which is mainly explained as a result of long-term chronic stress. stress-induced diabetes is often explained in association with glucocorticoids as these molecules participate in gluconeogenesis and cause the depletion of glycogen. Glucocorticoids inhibit glucose utilization by muscles and white adipose tissue and develop hyperglycaemia in the system. 65 The mechanism is well explained by the GLUT-4 translocation to the cell surface and the blocking of insulin resulting in the inability of skeletal muscle to absorb glucose. Increased lipolysis and glycerol formation in the white adipose tissue driven by glucocorticoids interfere with insulin signalling via gluconeogenesis. Insulin secretion by the pancreas is also challenged by the high corticosteroids during chronic stress.66,67 Another stress hormone, catecholamines accelerates glycolysis, glycogenolysis and gluconeogenesis while suppressing insulin-mediated glycogenesis during physiological conditions that cause hyperglycaemia. 68 β-AR activated in the adipocytes stimulate free fatty acid production and affect the MAPK/PKB signalling developed to insulin resistance. 69
Psychological stress disrupts the body's balance, resulting in physiological abnormalities and diabetes. Various forms of stress influence glucose metabolism and promote T2D complications by causing β-cell failure, insulin resistance, and neuroendocrine involvement. 70 A study was conducted to examine the role of stress responses in the prediabetic condition in Latino adults. The authors concluded the study with the negative impact of stress on behavioural and cognitive development, specifically related to food behaviours which can be mitigated by personalized approaches that address the influence of stress and provide coping mechanisms and support to promote healthy behaviours in pre-diabetes. 71 A study by 72 aimed to understand the connection between psychological stress and T2D. In their study, patients with T2D showed higher cortisol levels, indicating increased biological stress reactivity, which may contribute to an increase in cardiovascular pathologies. Patients with these co-morbidities exhibit a stronger subjective reaction to stress, however, it is unclear whether this reaction occurs before or after the issues. 72 A longitudinal relationship between inflammatory stress responses and mental health in T2D individuals have been demonstrated and the findings indicated that increased IL-6 were associated with depression symptoms and lower mental health-related QoL in T2D subjects. 73 Sedentary lifestyle is a major contributor to increased stress. According to a cross-sectional study, the iCARE cohort of adolescents and young people had a high prevalence of poor sleep, with nearly 50% experiencing daytime dysfunction and poor sleep quality. Even though there were no changes in sleep ratings between those with T2D and controls, poor sleep was linked to higher stress levels and less effective glycaemic control, emphasizing the necessity of addressing sleep quality in clinical settings. 74 These investigations demonstrate psychological stress induce immune activation in T2D both directly and via an increase in glucose levels.
By regulating the SNS, HPA, peripheral nervous system, limbic system, endocrine functions, and inflammatory responses to counteract stress. This promotes parasympathetic activation and a transition from sympathetic to parasympathetic activity by lowering vagal stimulation, which in turn decreases activation of the HPA axis and sympathoadrenal system, leading to a reduction in the production of stress hormones, indicating the possible direct and beneficial effect of Yoga on physiological pathways associated with stress. 75 The effects of Hatha yoga on blood pressure (BP) and neurohormonal modulation were evaluated in a pilot study school student (n = 31). Compared to the control group (−0.07/−0.79 mm Hg), the yoga group had a higher BP decrease (−3.0/−2.0 mm Hg), with a substantial decline among prehypertensive students (−10.75/−8.25 mm Hg vs 1.8/1.0 mm Hg, P = .02 for systolic BP). Hypothalamic-pituitary-adrenal (HPA) and sympathetic nervous system (SNS) activity did not significantly alter, but a little decrease in α-amylase activation indicated a decreased SNS drive. These results encourage more research to validate yoga's function in regulating blood pressure in young people. 76 Sudarshana Kriya Yoga is known to have antidepressant effects on alcohol-dependent subjects. A study was conducted for a two-week duration, participants were randomized into Sudarshana Kriya Yoga or control groups. Sudarshana Kriya Yoga involved alternate-day supervised breathing exercises (Ujjayi pranayama, Bhastrika pranayama, Cyclical breathing). The results showed that both group's BDI scores decreased, with a significant depletion in the Yoga group. A similar trend was observed in the plasma cortisol and ACTH levels as well. This study indicated that Sudarshana Kriya Yoga may have antidepressant effects in alcohol-dependent individuals, possibly mediated by reduced stress hormone levels.77,78 A nonrandomized prospective study for 10 days (n = 86), showed reduced cortisol levels and elevated β-endorphin levels suggesting even a short-term Yoga-based lifestyle can be beneficial in stress management. 25 The foundation of Yoga is the idea that the body and mind are inextricably linked which enhances blood circulation, muscle strength, flexibility, and oxygen uptake. 79 A poor mood and psychological stress both play a role in managing diabetes. 80 Stress stimulates the HPA and SNS, as well as parasympathetic withdrawal, which raises levels of epinephrine, norepinephrine, catecholamines, cortisol, leptin, prolactin, growth hormone, glucagon and neuropeptide which may lead to manifestation of diabetes. 81 A comparative clinical trial conducted by 82 demonstrated how mind-body training (n = 80) can regulate inflammation and catecholamines levels compared to the control group. This study demonstrated significant increase in anti-inflammatory cytokine and reduced pro-inflammatory cytokine by potentially regulating stress responses. 82 Another study focused on transcendental meditation (n = 19) showed that the regular practice of meditation reduces the plasma catecholamines by regulating the sympathetic-adrenal medulla system. 83 A randomized study of 33 participants introduced to kundalini Yoga was analyzed for multiple variables including urinary catecholamines and salivary cortisol to understand the relationship between cognitive behaviour and Yoga. Improved levels of these variables suggested promising stress management through Yoga84,85 in their study, demonstrated how a single 15-min bout of 6 breaths per minute would be sufficient to cause a reduction in stress hormones. This simple 15-min breathing reduces arterial norepinephrine, adrenocorticotrophic hormone, cortisol, and arterial epinephrine in the subjects (n = 10). 85 A group of researchers investigated how three Yoga poses (Nadi Shuddhi Pranayama, Kati Chakrasana, and Vakrasana) affected depression and glycaemic control in people with T2D (n = 9). The results revealed that the participant's FBS, PPBS, and RBS values decreased over the course of the two visits, falling between baseline and visit 2 by 131.33 ± 12.89 to 122.33 ± 10.63 (P < .0001), 183.3 ± 28.02 to 167.11 ± 13.95 (P = .0052), and 181.81 ± 20.8 to 169.22 ± 21.79 (P = .0050), respectively. Interestingly, the HAM-D score also decreased from 9 to 3.44 in the participants (P < .0001). 86 A study compared the stress and inflammation status in the long-term (n = 15) and short-term meditators(n = 58) with an age-matched healthy controls (n = 24). Baseline measurement of the markers such as cortisol, β-endorphin, TNF-α and IL-6 were compared in three groups and significant (P < .05) differences were observed in the plasma levels of these markers along with BMI and blood pressure among the meditator groups versus control. 87 Taken together, practising Yoga displays beneficial effects on reducing stress hormones and thereby improve glucose homeostasis along with reducing inflammation in T2D (Figure 3).

Yoga improves stress induced inflammation in T2D: Activated HPA axis plays a major role in the stress induced inflammation. This activation leads to the secretion of glucocorticoids and cortisol, which then interact with receptors on the surface of immune cells (T-cells). At the cellular level, specifically in signal transduction pathways, stress hormones have a pivotal role by inhibiting pathways associated with inflammation, including NF-κβ. This suppressed secretion of proinflammatory cytokines contribute overall modulation of inflammatory response, which in turn leads to depression/anxiety. Introduction of Yoga asanas such as Surya Namaskara followed by Dhyana, Bhujangasana, Parsvakonasana, Pashchimottaanasana, Pavanamuktasana, Halasana, Sarvangasana and Shavasana, reduce stress by modulating the neuroendocrine axis.
Yoga for T2D Complications
T2D patients are often associated with micro and macrovascular complications such as retinopathy, nephropathy, and cardiovascular disorders. Several studies have attempted to show Yoga to facilitate management of T2D complications. A systematic review and meta-analysis of 12 randomized controlled trials (RCTs) involving 800 participants revealed that yoga practices, particularly Hatha and Iyengar yoga, significantly reduced fasting blood glucose by 18.76 mg/dL and HbA1c levels by 0.53%. These improvements suggest enhanced glycemic control and reduced oxidative stress in retinal microvasculature. 88 Another study involving 50 elderly diabetic participants demonstrated that yoga improved oxidative stress markers, reducing malondialdehyde levels by 0.25 nmol/mL and increasing superoxide dismutase activity by 0.35 U/mg protein. These changes indicate enhanced antioxidant defences and a potential slowing of diabetic nephropathy progression. 89 Building on these findings, another meta-analysis of 12 studies with 864 participants found that Sudarshan Kriya helped to decrease fasting blood glucose by 25.89 mg/dL and HbA1c by 0.48%. This effect was attributed to the downregulation of the NF-κB pathway and reduced levels of inflammatory cytokines such as TNF-α and IL-6, which play a critical role in the development of nephropathy and cardiovascular complications. 90 Further supporting these outcomes, an RCT involving 60 participants practicing Vinyasa yoga demonstrated notable reductions in total cholesterol (12.8 mg/dL) and oxidative stress markers, including a 0.36 nmol/mL decrease in malondialdehyde. These changes indicate improved endothelial function and a lower risk of atherosclerosis. 91 A broader systematic review and meta-analysis of 23 studies involving 2473 participants further reinforced these findings, reporting reductions in fasting blood glucose by 14.3 mg/dL and HbA1c by 0.45%. This evidence supports role of Yoga in mitigating systemic inflammation and vascular dysfunction. 92 Similarly, a comprehensive systematic review of 25 studies with 1217 participants highlighted that various yoga styles, including Restorative and Yin yoga, were associated with improvements in fasting blood glucose, lipid profiles, and body composition. These findings underscore the potential of yoga in preventing both microvascular and macrovascular complications of diabetes. 93 In addition to these larger studies, smaller-scale trials have also yielded promising results. A pilot RCT involving 29 participants at risk for diabetes found that yoga therapy led to an 8.9 mg/dL reduction in fasting blood glucose, reflecting improved metabolic function and autonomic balance. 94 Another RCT with 60 diabetic participants revealed a significant decrease in DNA damage markers, including a 0.42 ng/mL reduction in 8-hydroxy-2′-deoxyguanosine levels, suggesting enhanced mitochondrial function and reduced oxidative stress. 95 These findings align with earlier research indicating that yoga practice could lower fasting blood glucose by 21.9–76.6 mg/dL and HbA1c by 1.0–1.6%, highlighting its therapeutic potential in enhancing AMPK activation and GLUT4 translocation for improved glucose uptake. 96 Collectively, these studies suggest that yoga modulates critical molecular pathways, including Nrf2, eNOS, and TGF-β, leading to improved metabolic, vascular, and renal health. By addressing key mechanisms such as oxidative stress, inflammation, and glucose metabolism, yoga emerges as a promising adjunctive therapy for managing diabetic complications (Figure 4).
Yoga exerts beneficial effects on nonmodifiable risk factors of T2D & reduce chronic inflammation and associated complications.
List of Asanas with Their Targeted Effects and Supporting References. the Table Presents various Yoga Postures (Asanas), Their Associated Physiological or Therapeutic Effects Based on Specific Biomarkers, and the Corresponding Scientific References Supporting These Effects.

Conclusion
Constitutive systemic metabolic imbalance in diabetic milieu might act as either precursor or substrate to activation of immune signalling network over the time leading to end organ complications. T2D is considered as a chronic inflammatory disease and a bidirectional activation between immune system and glucose/lipid metabolism is observed. Although the development of the disease is majorly due to the combined effect of defective insulin secretion and the inability of the specific tissues to sense and respond to the secreted insulin, they are mechanically regulated by multiple pathways which are perturbed during the hyperglycaemia/hyperlipidaemia conditions subsequently activate chronic inflammation. The activated NF-κβ and JNK pathways result in insulin resistance and associated chronic inflammation in T2D with a reduced production of anti-inflammatory markers whereas the overproduction of SAA1 and SAA2 by adipocytes associated with the obesity triggers the expression of various pro-inflammatory markers. Distinct to these mechanisms the autonomic-vagal regulation and the HPA axis play an important role in the stress-associated development of T2D. Activation of the parasympathetic system and anti-stress mechanisms alter the psychological and metabolic profiles in T2D subjects with reduced insulin resistance, increased sensitivity, better glucose tolerance and fatty acid oxidation. Understanding and tackling the pathophysiologic mechanism associated with T2D is the current challenge for the disease management. Lifestyle modification along with Yoga promotes psychosomatic and spiritual health and holistic living. Healthy Yogic diet, tailored activity patterns in the form of Asanas, relaxation, and positive attitude as well as psychosomatic harmonizing effects of pranayama can turn out as best lifestyle ever designed. Outcome from the clinical studies have already shown how Yoga practices such as pranayama, bandha, mudras, asanas, mindfulness and cleansing can improve chronic inflammatory conditions and thereby improving glycaemic index and associated metabolic perturbations. Though Integrative practices like Yoga could play a complementary role in managing Type 2 Diabetes (T2D) by addressing both physiological and psychological factors the scientific evidence on Yoga remains limited. The lack of Yoga standardization is one of the key challenges. Different Yoga (Kundalini, Hatha, Vinyasa) follows diverse styles including duration, intensity and objectives. Reporting of research outcomes adhering to specific guidelines such CONSORT will improve the reliability of data. 100 Smaller sample size, lack of randomization and blinding, drop-out rate during the intervention, subjective self-reported data and use of a weak control group (mismatched or waitlist group) reduce the statistical significance of the studies. Most of the Yoga interventions are restricted to short term which can truncate the actual findings. Another key challenge is understanding the mechanical insight of Yoga using various models. Incorporating Yoga in animal models and cell lines is less practical due to the difficulties of training/mimicking the asanas. Although few in vivo studies highlighted how stretching affects the inflammatory markers the complexity of Yoga prevents to consider the translational application. 101 The holistic benefits of Yoga are often hindered by lifestyle habits such as alcohol consumption, junk food and smoking. Addressing these limitations is crucial for advancing our understanding of how Yoga impacts health and well-being effectively and providing a link for future research directions of Yoga in T2D management. Larger RCTs with various populations are required to ensure generalisability across age, gender, and ethnicity, as well as different T2D severity levels. Standardising Yoga interventions (duration, intensity, and style) will increase study comparability and prevent bias. Mechanistic studies focusing on the physiological and biochemical mechanisms by which Yoga impacts glycaemic control, insulin sensitivity, and stress markers in T2D patients, as well as follow-up to assess the long-term sustainability of Yoga's benefits and combination interventions (eg, dietary changes, exercise), will rule out disease progression and management challenges. Satvik diet along with Yoga intervention will improve physical and mental health. The plant based/vegetarian diet are rich in phytochemicals and antioxidants which are known to reduce inflammation, oxidative stress, cortisol levels and improve gut health and cognitive function which enhances the effectiveness of Yoga.The mutiomics approach can provide a comprehensive view of how Yoga influence on various mechanisms such as inflammation, stress and insulin resistance of T2D by assessing the changes in gene expression(transcriptomics), proteome (proteomics) and metabolome (metabolomics). The accessibility of Yoga sessions in community health programs, clinics, and digital platforms, in addition to personalised education, emphasises the benefits of Yoga by instructing patients on how it complements pharmacological treatments and dietary interventions will improve T2D management. Standard medical guidelines for T2D management can also incorporate stress management strategies like pranayama (breathing exercises) and mindfulness.
Footnotes
Abbreviations
Acknowledgments
We gratefully acknowledge the Department of Biotechnology (DBT)-BUILDER, Government of India (GOI BT/INF/22/SP43065/2021) and Manipal Academy of Higher Education, Manipal for infrastructure.
Author Contributions
HBJ, ASN and RB performed the literature survey, collected the data and prepared the original draft. KRH, AN, SU and NKM provided advice and contributed to the writing, MJ and BH supervised, conceptualized, and curated the data for the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank DST-SATYAM, Government of India (DST/SATYAM/2020/247(G)) for the financial support.
{kind=link}
{kind=link}