
Abstract
In the article, “Insurance Reimbursement for Complementary Healthcare Services,” we reported that the likelihood of reimbursement for complementary health care services in New Hampshire was significantly lower as compared with services of primary care physicians. The relatively low likelihood of reimbursement for integrative health care suggests that many patients who want such services must pay for them out of pocket. Affordable access to these services may be similarly limited in other states; certainly the utilization of integrative health care services varies significantly across the US states, and such variation may be tied to likelihood of reimbursement. Unwarranted geographic variation in reimbursement for integrative health care services is likely to compound inequities in access to health care in general, particularly for people of lower socioeconomic status. The aspirational value of Health Justice asserts the obligation of societies to attend to the basic health needs of all, with particular attention to the disadvantaged. A new project under development, The Atlas of Integrative Healthcare, is intended to support the advancement of health justice. The Atlas project is expected to support the policy goals of the integrative health care community with regard to helping patients access the high-value integrative health care services that they need and want.
In the article, “Insurance Reimbursement for Complementary Healthcare Services,” 1 we reported the likelihood of insurance reimbursement for complementary health care services. We studied health claims for services provided to adults in nonemergent outpatient settings in New Hampshire in 2014. We found that, as compared with primary care physician services, the likelihood of reimbursement for any complementary health care service was 69% lower for acupuncturists, 71% lower for doctors of chiropractic, and 62% lower for doctors of naturopathic medicine. For CPT 99213 (reevaluation of an existing patient—the most frequently billed of all procedure codes), likelihood of reimbursement was 34% lower for acupuncturists, 77% lower for doctors of chiropractic, and 60% lower for doctors of naturopathic medicine. We noted that the cause of the observed differences is uncertain, but regardless of the reason or mechanism by which differences in reimbursement occur, the lack of reliable health insurance reimbursement for services that people need and want may lead to inequitable health care access and higher costs.
Need for Improved Patient Access to Integrative Health Care Services
Health care delivery in the United States is fragmented, disorganized, and aimed downstream at reactive treatment of acute illness and chronic conditions with insidious onset rather than health promotion and prevention of chronic diseases and pain disorders, which constitute the lion’s share of our health care burden. Increased utilization of integrative health care services (including complementary therapies) shows promise as a strategy for shifting the system from disease care to health creation, but many patients must venture outside conventional systems of health care delivery and reimbursement and, on their own, decipher how to locate and pay for integrative health care services. This fractured care pathway is inefficient, potentially harmful, and fails to put patients’ needs and preferences first. An important key to development of a patient-centered health care system is facilitation of full and affordable access to integrative health care services.
Geographic Variations in Utilization and Access to Integrative Health Care Services
The relatively low likelihood of reimbursement for integrative health care that we found in New Hampshire suggests that many patients who want such services must pay out of pocket. Affordable access to these services may be similarly limited in other states. Certainly the utilization of integrative health care services varies significantly across the US states. These geographic variations may result from differences in insurance coverage and reimbursement, differences across states in provider supply, and licensing and scope of practice, as well as differences in patient beliefs and preferences.
Geographic variations in the utilization of chiropractic services in the United States have been studied in detail. Few integrative health care services are covered under Medicare, but because coverage is available for chiropractic services, claims data are available for research on a national scale. Analysis of nationally representative Medicare data for 2007 found that chiropractic availability by state varied 6-fold, and chiropractic use per 1000 beneficiaries varied nearly 30-fold. 2 A subsequent study using similar methods found that the use of chiropractic care was strongly correlated with the regional supply of chiropractors. 3 A third study that focused on Los Angeles County (Figure 1) found significant variations in utilization of chiropractic services under Medicare by patient ZIP code and racial/ethnic category, and concluded that older blacks and Hispanics may be underserved with regard to chiropractic care. 4 The causes of geographic variations in health care utilization are not always known, but may be unwarranted, depending on patient need and preference.
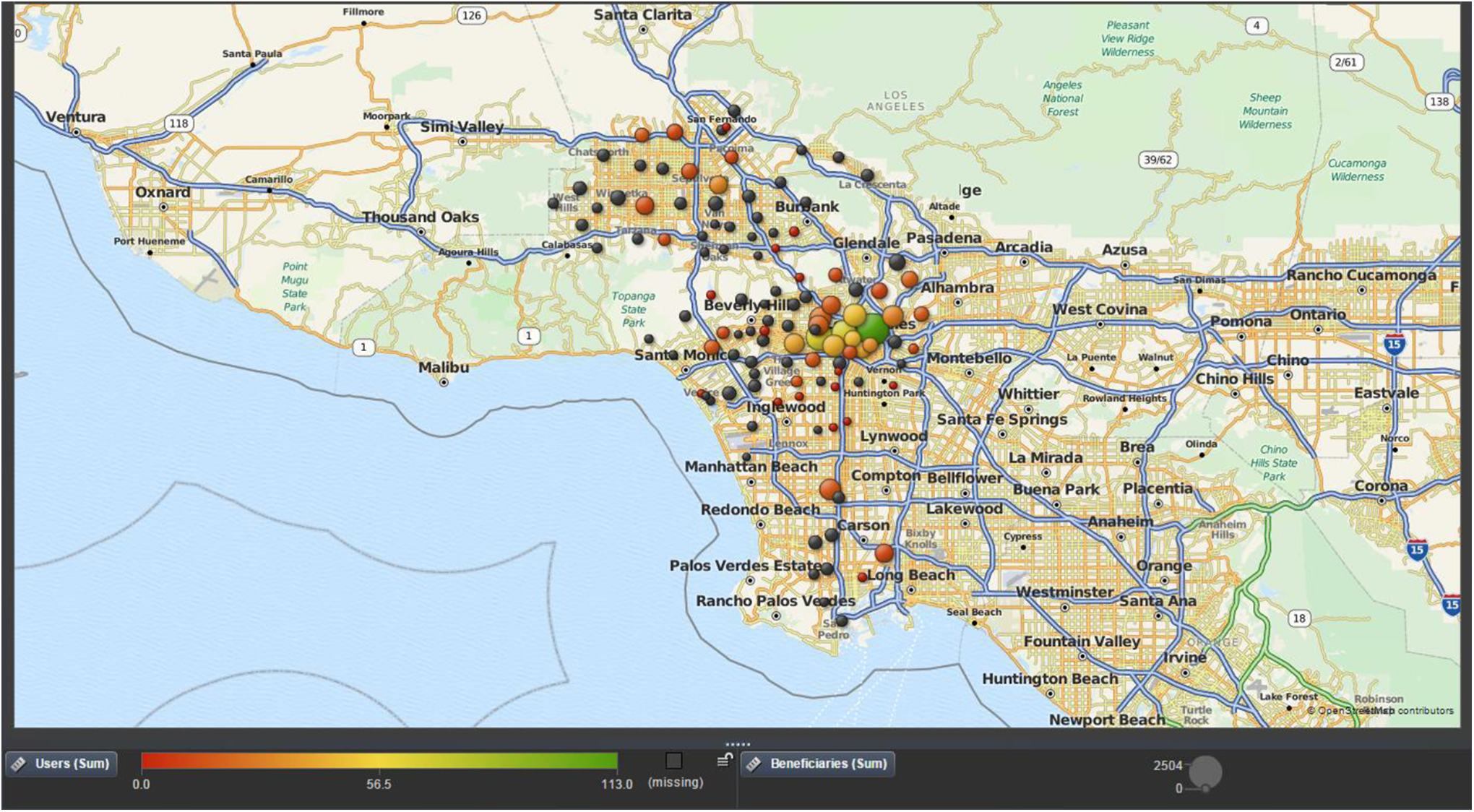
Use of chiropractic services under Medicare among Asians in Los Angeles County, 2008.
Unwarranted Geographic Variations
Where people live predicts both their ability to access health care services and their overall health status. Such geographic variation in access to necessary medical services is unwarranted. The concept of unwarranted variation in US health care, introduced by Wennberg, 5 refers to differences in medical service delivery that cannot be explained by type or severity of illness, or by patient preferences. Significant geographic variation in reimbursement for identical health care services is also unwarranted. However, despite a provision of the Affordable Care Act that prohibits discrimination in private health insurance coverage by provider specialty, 6 differences between states in the implementation of the law have been reported. 7 Unwarranted geographic variation in reimbursement for integrative health care services compounds inequities in access to health care, particularly for people of lower socioeconomic status.
Values-Based Health Care and Health Justice
Wherever people live, they should be able to access and afford the kinds of health care services that they need and want; this notion is consistent with widely held human values. In the effort to reform the US health care system, much attention has been paid to the need for value-based health care, with value defined as health outcomes achieved per dollar spent. 8 An important piece of this value equation is the human values that inform our notions of quality in health care. Among the domains of health care quality identified by the Institute of Medicine are patient-centered (respectful of and responsive to individual patient preferences, needs, and values) and equitable (not varying in quality because of patient personal characteristics). 9 These domains of quality rest on universal human values. High-quality health care is thus not only value-based, but also values-based. Where people are able to access affordable, equitable, and patient-centered care, there is Health Justice. 10 The aspirational value of health justice asserts the obligation of societies to attend to the basic health needs of all, with particular attention to the disadvantaged. 11 A recent commentary recommended efforts to advance the cause of health justice through integrative health care. 12
Atlas of Integrative Health
A new project under development, The Atlas of Integrative Healthcare, 13 is intended to support the advancement of health justice. By quantifying and illustrating unwarranted variations in access to integrative health care services, as well as differences in reimbursement as reported in our New Hampshire study, the Atlas will arm policy makers with the information needed to improve access and correct inequities. The Atlas will draw on multiple data sources, including state-level health claims databases, Medicare, Medicaid, private payers, and aggregated proprietary datasets, as well as state boards of registration and professional associations. To inform health policy efforts with up-to-date, state-by-state data, the Atlas Project will illustrate status, trends, and variations in licensure, scope of practice, provider supply, utilization of services, and insurance reimbursement for integrative health care services. The Atlas will support the policy goals of the integrative health care community and help patients access the health care services they need and want.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.