
Abstract
Background.
This study aimed to identify the factors of CAM usage for general health and to determine the factors associated with the usage of different types of CAM after the diagnosis of chronic diseases among The Malaysian Cohort participants.
Methods.
This was a cross-sectional study derived from The Malaysian Cohort (TMC) project, a prospective population-based cohort aged between 35 to 65 years old that recruited from April 2006 to September 2012. Association between the CAM usage and contributing factors were determined via logistic regression.
Results.
The sample were mostly female (58.1%), Malays (43.1%), came from urban (71.9%), aged 44 years and below (26.8%) and had secondary education (45.9%). The prevalence of CAM usage varied across diseases; 62.8% in cancer patients, 53.3% in hypercholesterolemia, 49.4% in hypertensives and 48.6% in diabetics. General CAM usage was greater among female (OR: 1.54, 95% CI: 1.49, 1.59), Chinese (OR: 1.15, 95% CI: 1.12, 1.19), those with higher education (OR: 3.12, 95% CI: 3.00, 3.25), urban residents (OR: 1.55, 95% CI: 1.50, 1.61) and older people (OR ranging from 1.15 to 1.75) while for post-diagnosis of chronic diseases usage, the odds were higher among those with lower education and living in rural areas.
Conclusion.
Health status, educational level, age, living location and types of chronic diseases were significant factors that influence CAM usage for the intent of either health maintenance or disease treatment. Further exploration on CAM safety and benefit are crucial to minimize the adverse effect and to ensure the efficacy of CAM product.
Keywords
Recently, the use of complementary and alternative medicine therapy for disease prevention and maintenance of well-being has been increasing worldwide, both in developed and developing countries. 1 The development of complementary and alternative medicine has been influenced by the diverse cultural and historical conditions, which is primarily based on a holistic approach—emphasizing on health rather than on disease. 2
Malaysia is a multiethnic country consisting of 3 major ethnic groups: Malays, Chinese, and Indians. In 2005, it was estimated that 29.25% of the Malaysian population had ever used complementary and alternative medicine with consultation. 3 The prevalence of complementary and alternative medicine used varied between ethnicity with Chinese showing the highest prevalence (32.98%), followed by Malays (31.36%) and Indians (18.14%). 3 There was a substantial disparity of 37% difference in prevalence of complementary and alternative medicine used before and after diagnosis of diseases. 4 Previous studies conducted in Malaysia found that the prevalence of complementary and alternative medicine used in chronic disease also varied significantly: 58.5% to 62.5% in diabetes, 5,6 62.6% in hypertension, 7 46.1% in cancer, 8 and 9.6% to 30.7% in hypercholesterolemia. 9,10
Currently, the development of many types of complementary and alternative medicine is not at par with modern scientific standards, especially in terms of the objective and unbiased evaluation of their efficacy and safety attributes. Hence, it is crucial to share national experience and information on complementary and alternative medicine usage on the international platform for the purpose of public health risk stratification and intervention. Knowledge on the pattern of complementary and alternative medicine usage and its associated factors might assist health care professionals to better understand and manage the personalized care of the patients based on their ethnocultural background. This is highly important especially to understand the interaction between natural products and conventional medicine that can cause noticeable morbidity from inadvertent alterations in body systems. 11 This knowledge will also help pharmacologists and pharmacists to monitor complementary and alternative medicine safety in the general population.
The objectives of this study were to identify the factors of complementary and alternative medicine usage for general health and to determine the factors associated with the usage of different types of complementary and alternative medicine after the diagnosis of hypertension, hypercholesterolemia, diabetes, and cancer among the Malaysian Cohort study subjects. We hypothesized that social demographic factors and disease state played a role in complementary and alternative medicine usage.
Methods
Data Sources and Samples Selection
This was a cross-sectional study derived from the baseline of the Malaysian Cohort (TMC) project, a prospective population-based cohort that recruited from April 2006 to September 2012. 12 It involved 97 492 individuals from the original 106 527 TMC subjects aged between 35 and 65 years consisting of Malays (42 042), Chinese (31 876), Indians (15 199), and other ancestry groups (8375). The sampling method was based on a mixed approach that included purposive, cluster, and targeted sampling. The ethical approval was granted by the institutional review and ethics board of Universiti Kebangsaan Malaysia (Project Code: FF-205-2007), in accordance with the Declaration of Helsinki. All subjects gave their written consent prior to study.
Selection of Variables
All the variables including sociodemographic risk factors, types of complementary and alternative medicine used, and 4 major noncommunicable diseases in the analyses (cancer, hypertension, diabetes mellitus, and hypercholesterolemia) were assessed using self-report questionnaires.
Dependent Variables
There were 2 dependent variables used for the analysis. The first dependent variable was complementary and alternative medicine usage throughout the subject’s life, which was coded as ever or never. The second dependent variable was the usage status (coded as either yes or no) of different types of complementary and alternative medicine after being diagnosed with diabetes, hypertension, hypercholesterolemia, and cancer. The “after diagnosis” status was based on the algorithm that the age of usage of specific complementary and alternative medicine should be after the age of diagnosis of the specific disease in the dataset. In this study, we captured complementary and alternative medicine such as acupuncture, aromatherapy, and garlic (the full list of complementary and alternative medicine is available in Supplemental Materials). Then the list of complementary and alternative medicine was categorized into 6 categories such as natural products, manipulative, and body-based practices based on a previous study conducted in Singapore. 13
Independent Variables
Sociodemographic factors that were included were age, gender, ethnicity, education level, and locality. Age was categorized into 6 groups—<45, 45 to 49, 50 to 54, 55 to 59, 60 to 64, and ≥65 years—based on a previous study. 3 Ethnicity was defined based on paternal grandfather. Education level was based on the highest education level achieved according to 3 categories: no schooling/primary school level, secondary school level, or university/college level. The locality of the subjects was based on the recruitment center: either rural or urban.
Major noncommunicable diseases that were assessed in the analyses were cancer, hypertension, diabetes mellitus, and hypercholesterolemia. Cancer was defined by diagnosis and had received treatment. Hypertension was defined by diagnosis with medication; and/or having systolic blood pressure (BP) of ≥140 mm Hg and/or diastolic BP of ≥90 mm Hg at the point of recruitment, measured either lying or standing. 14 Diabetes mellitus was defined by diagnosis with medication; and/or having fasting plasma glucose level of ≥7.0 mmol/L at the point of recruitment. 15 Hypercholesterolemia was defined by diagnosis with medication; and/or having fasting plasma total cholesterol level of ≥6.2 mmol/L and low-density lipoprotein level of ≥4.1 mmol/L at the point of recruitment. 16,17 All diseases were categorized into present or absent.
Statistical Methods
This study consisted of 2 parts of analyses. The first part involved multivariable logistic regression to investigate the associations between the complementary and alternative medicine usage and the risk factors (sociodemographic factors and the 4 diseases). In the second part, multivariable logistic regression was performed for each type of complementary and alternative medicine in order to investigate the sociodemographic factors that influenced the usage of complementary and alternative medicine after the diagnosis of a particular disease.
For each multivariable logistic regression, we fitted a model that included all the selected factors having Wald statistics with P < .05 (2-tailed). The goodness of fit of the models were assessed using Nagelkerke’s pseudo-R 2 and the area under the receiver operating characteristic curve (AUC). The statistical significance level was set at P < .05 (2-tailed). All analyses were performed using SPSS IBM software version 22 (IBM Corp, Armonk, NY).
Results
In general, the characteristic of the sample were mostly female (58.1%), Malay (43.1%), came from urban area (71.9%), aged 44 years and younger, and had secondary education (45.9%; Supplemental Table S1). The prevalence of using complementary and alternative medicine was higher among females compared to males (55.2% and 47.2%, respectively). Complementary and alternative medicine usage was highest among Chinese (60%), followed by Malays (51.3%), Indians (43.3%), and other ethnic groups (39.1%; Table 1). Most complementary and alternative medicine users had higher education level, stayed in urban areas, and were of age 65 years and older (Table 1). The prevalence of complementary and alternative medicine usage among subjects with history of cancer (62.8%) and hypercholesterolemia (53.3%) was higher than subjects with diabetes mellitus (48.6%) and hypertension (49.4%; Table 1). After controlling for all variables (confounding effects), the strengths of the associations were different—either increased or decreased although most of the effect direction remained. The odds ratio increased from crude to adjusted odds ratio for some variables such as gender (female from 1.37 to 1.54), education level (eg, university from 3.08 to 3.12), age (eg, 65 years old and older from 1.07 to 1.95), hypertension (from 0.83 to 0.88), diabetes (from 0.85 to 1.01), and hypercholesterolemia (from 1.10 to 1.14; Table 1). While some variables showed reduced strength of odds ratio from crude to adjusted: for example, Chinese reduced from 1.42 to 1.15, urban residents from 1.95 to 1.55, cancer from 1.58 to 1.38, and hypercholesterolemia from 1.10 to 1.14 (Table 1).
The Association Between CAM Usage and Sociodemographic Factors and 4 Major Noncommunicable Diseases Among TMC Subjects at Baseline (N = 97 492).

Abbreviations: TMC, the Malaysian Cohort; CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio.
*Denotes significance at P value of .05. Adjusted with sociodemographic factors and 4 major diseases.
The final model consisted of gender, age, ethnicity, education level, locality, and types of diseases. The combination of these factors explained about 10% of complementary and alternative medicine usage. As shown in Table 1, the odds of complementary and alternative medicine usage was higher for females compared to males (odds ratio [OR] = 1.54; 95% confidence interval [CI] = 1.49, 1.59; P < .001). The Chinese had significant higher odds of using complementary and alternative medicine compared to Malays (OR = 1.15; 95% CI = 1.12, 1.19; P < .001), while Indians and other ethnic groups had less odds of using of complementary and alternative medicine compared to Malays ([OR = 0.65; 95% CI = 0.63, 0.68; P < .001] and [OR = 0.72; 95% CI = 0.69, 0.76; P < .001], respectively). Subjects who had tertiary or secondary levels of education had triple and double the odds of complementary and alternative medicine usage, respectively, when compared to those who had no formal education or only had primary education. Those living in urban areas had 55% higher odds of using complementary and alternative medicine compared to those living in rural areas. The odds of complementary and alternative medicine usage increased by age, 95% higher odds for those with the age of 65 years and older, down to 15% higher odds for those within the of age 45 to 49 years if compared to those with the age of below 45 years (Table 1). Subjects with cancer history had 38% higher odds of using complementary and alternative medicine compared to those without cancer history, whereas hypercholesterolemia subjects had 14% increased odds of using complementary and alternative medicine compared to non-hypercholesterolemia subjects. Hypertensive subjects had 12% lower odds of using complementary and alternative medicine compared to nonhypertensive subjects. There was no significant association between complementary and alternative medicine usage and the diabetic status of subjects (OR = 1.01; 95% CI = 0.97, 1.04; P = .746).
Specific Complementary and Alternative Medicine Usage After the Diagnosis of Hypertension
Hypertensive patients used several type of complementary and alternative medicine after diagnosis. There were 47% patients that used energy therapy, 44.5% used manipulative body practice, 25% used mind-body complementary and alternative medicine, 41.6% used whole-medical-systems, 46.8% used natural products, and 46.9% used other types of complementary and alternative medicine (Figure 1).

Types of complementary and alternative medicines used by diseases.
Among subjects with hypertension, the significant factors associated with the usage of natural products after diagnosis were ethnicity, level of education, locality, and age (Table 2). The Chinese have less odds of using natural products after the diagnosis if compared to Malays (OR = 0.79; 95% CI = 0.70, 0.89; P < .001). However, there was no difference of this pattern of usage among the Indians and other ethnic groups if compared to the Malays. There was an inverse relationship between the level of education and the odds of natural products consumption after the diagnosis, with 27% (OR = 0.73; 95% CI = 0.65, 0.82; P < .001) and 34% (OR = 0.66; 95% CI = 0.58, 0.75; P < .001) reduction of odds of usage for secondary and tertiary education levels if compared to primary education level, respectively. Hypertensive subjects who lived in urban areas had 33% (OR = 0.67; 95% CI = 0.60, 0.75; P < .001) less odds of using natural products after the diagnosis compared to those who lived in rural areas. There was significant association between natural products usage after hypertension diagnosis with the older subjects, with the peak of 61% higher odds in the 55 to 59 years age group if compared to the 44 years and younger age group.
Characteristics Associated With the Usage of Complementary Alternative Medicines After the Diagnosis of Hypertension.

Abbreviations: CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval.
*Denotes significance at P value of .05. Adjusted with sociodemographic factors.
Only age and education level were associated with the use of whole-medical-systems complementary and alternative medicine after the diagnosis of hypertension (Table 2). There was a significant association between this pattern of usage for those within the 55 to 59 years age group if compared to the 44 years and younger age group (OR = 1.51; 95% CI = 1.13, 2.03; P = .006). However, this significant pattern was not seen among the older and younger age groups. Besides that, the odds of postdiagnosis usage of this complementary and alternative medicine type showed a decreasing trend with higher levels of education. The odds were 31% (OR = 0.69; 95% CI = 0.53, 0.89; P = .004) and 36% (OR = 0.64; 95% CI = 0.49, 0.85; P = .002) lower for those who received secondary and tertiary education level if compared to those with primary education level, respectively.
The level of education and age were significantly associated with other types of complementary and alternative medicine used after the diagnosis of hypertension (Table 2). There were lower odds of those with higher education levels in using other types of complementary and alternative medicine postdiagnosis in comparison with those with primary school or no schooling, with 50% (OR = 0.50; 95% CI = 0.35, 0.70; P < .001) and 48% (OR = 0.52; 95% CI = 0.36, 0.75; P = .001) lower odds in secondary and tertiary education, respectively. In comparison with the lowest age group, the only age group that showed significant association with other complementary and alternative medicines usage was those within the 55 to 59 years age group, which showed 50% higher odds (95% CI = 1.03, 2.18; P = .035).
There was no significant association between the sociodemographic factors and the usage of manipulative and body-based practices, as well as energy therapies, after the diagnosis of hypertension.
Specific Complementary and Alternative Medicine Usage After the Diagnosis of Hypercholesterolemia
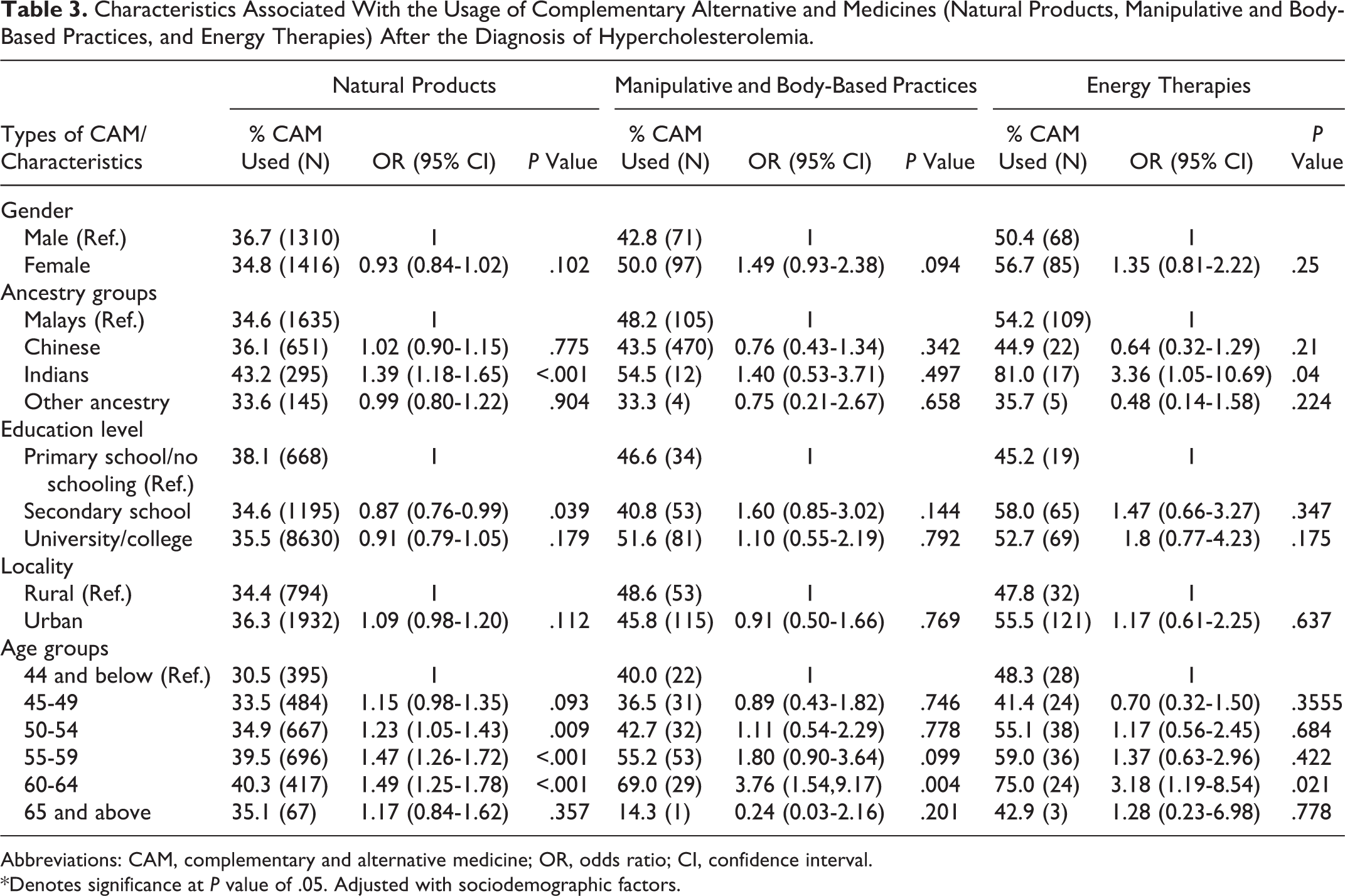
Figure 1 shows that the prevalence of hypercholesterolemia patients that used energy therapy was 43.8%, 41.3% used whole-medical-systems, 43.6% used natural products, and 46% used other types of complementary and alternative medicine.
Among subjects with hypercholesterolemia, there were significant associations between the usage of natural products after hypercholesterolemia diagnosis and the following factors: being Indian (OR = 1.39; 95% CI = 1.18, 1.65; P < .001); having secondary level of education (OR = 0.87; 95% CI = 0.76, 0.99; P = .039); and being in the older age groups. The odds of postdiagnosis usage of natural products increased by age, with the peak of 49% higher odds (95% CI = 1.25, 1.78; P < .001) for the 60 to 64 years age group in comparison with the lowest age group (Table 3). Similarly, there were also significant associations between the postdiagnosis usage of energy therapies and being Indian (OR = 3.36; 95% CI = 1.05, 10.69; P = .04) and being in the 60 to 64 years age group (OR = 3.18; 95% CI = 1.19, 8.54; P = .021). However, for the postdiagnosis usage of manipulative and body-based practices, only those in the 60 to 64 years age group showed a significant association (OR = 3.76; 95% CI = 1.54, 9.17; P = .004; Table 3).
Characteristics Associated With the Usage of Complementary Alternative and Medicines (Natural Products, Manipulative and Body-Based Practices, and Energy Therapies) After the Diagnosis of Hypercholesterolemia.
Abbreviations: CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval.
*Denotes significance at P value of .05. Adjusted with sociodemographic factors.
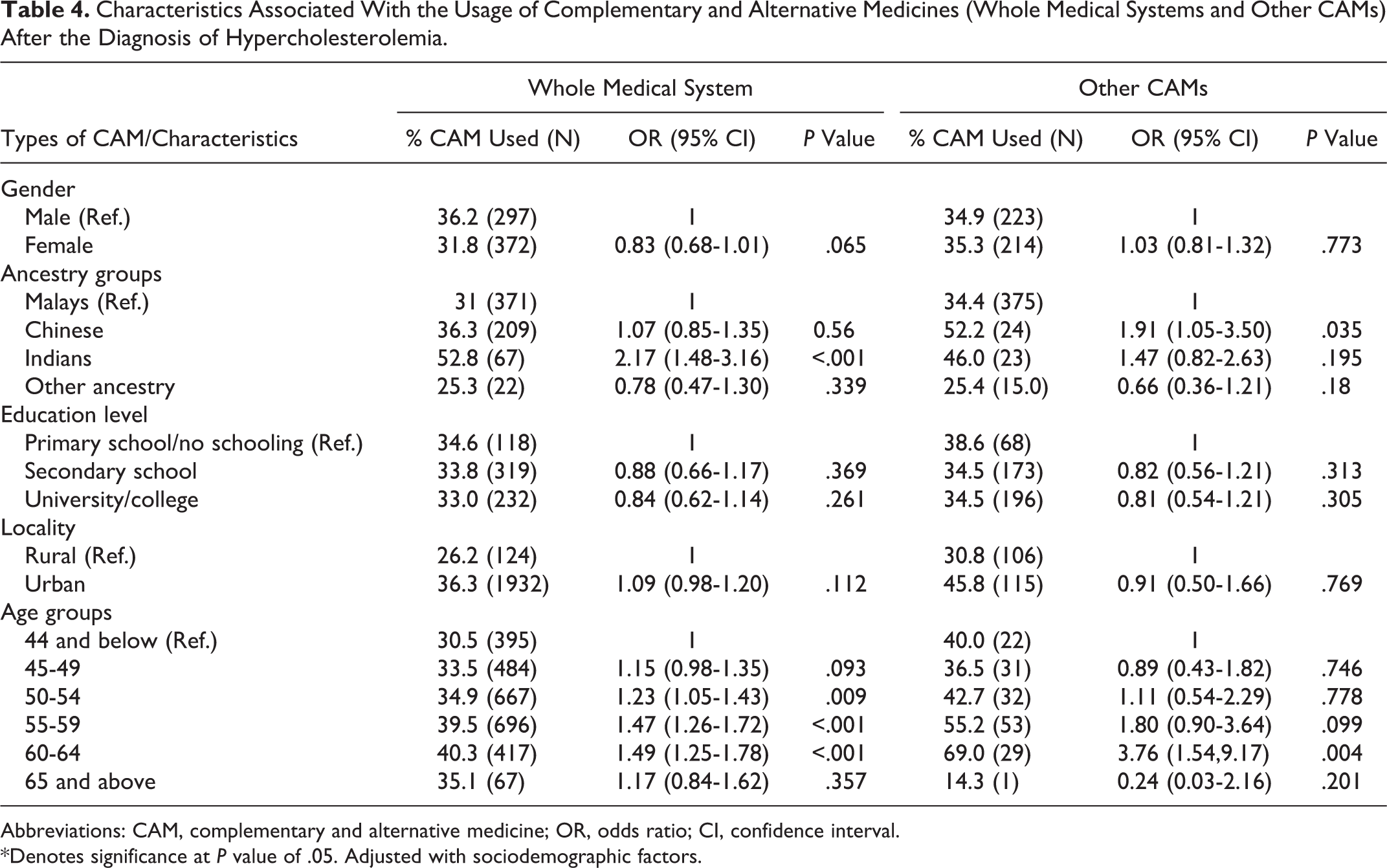
A pattern of similar characteristics was observed for the postdiagnosis usage of whole medical system, which were significantly higher risk among Indians (OR = 2.17; 95% CI = 1.48, 3.16; P < .001), among those with older age (OR range = 1.23-1.49), and lived in urban areas (OR = 1.09; 95% CI = 0.98, 1.20; P = .112). Interestingly, a slightly different characteristic was found for postdiagnosis usage of other complementary and alternative medicines, whereby a significantly higher odds was seen among Chinese (OR = 1.91; 95% CI = 1.05, 3.50; P = .035) and those within the 60 to 64 years age group (OR = 3.76; 95% CI = 1.54, 9.17; P = .004; Table 4). There were no significant difference in type of complementary and alternative medicine used between urban and rural.
Characteristics Associated With the Usage of Complementary and Alternative Medicines (Whole Medical Systems and Other CAMs) After the Diagnosis of Hypercholesterolemia.
Abbreviations: CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval.
*Denotes significance at P value of .05. Adjusted with sociodemographic factors.
Specific Complementary and Alternative Medicine Usage After the Diagnosis of Diabetes Mellitus
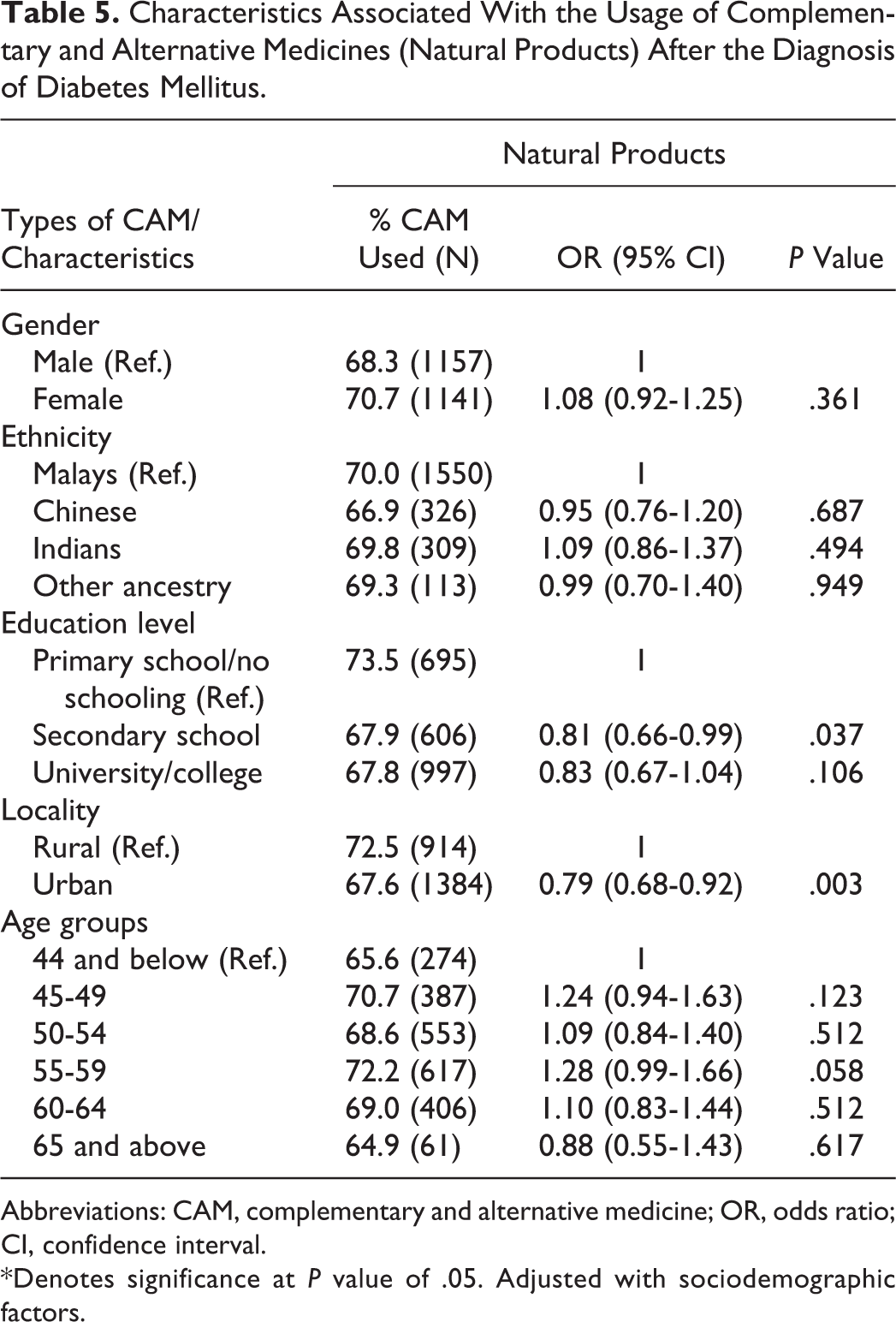
Only 18% of diabetic subjects used energy therapy, 18.4% used manipulative body practice, 16.3% used whole-medical-systems complementary and alternative medicine, 18.9% used natural products, and 19.5% other types of complementary and alternative medicine (Figure 1).
There were significant associations between the postdiagnosis usage of natural products among diabetics patients and having secondary level of education (OR = 0.81; 95% CI = 0.66, 0.99; P = .037) and living in urban areas (OR = 0.79; 95% CI = 0.68, 0.92; P = .003; Table 5). The postdiagnosis usage of other types of complementary and alternative medicines in the analyses showed no significant association with any of the sociodemographic factors.
Characteristics Associated With the Usage of Complementary and Alternative Medicines (Natural Products) After the Diagnosis of Diabetes Mellitus.
Abbreviations: CAM, complementary and alternative medicine; OR, odds ratio; CI, confidence interval.
*Denotes significance at P value of .05. Adjusted with sociodemographic factors.
Specific Complementary and Alternative Medicine Usage After the Diagnosis of Cancer
Only a small proportion of subjects with history of cancer used whole-medical-systems complementary and alternative medicine, which is 1.6%; 1.4% used energy therapy and 1.3% used manipulative body practice. This pattern of usage can also be seen for the usage of natural products, 1.3%, and 1.9% for other types of complementary and alternative medicine (Figure 1).
Among subjects with history of cancer, there was null relationship between the sociodemographic factors in this study and the postdiagnosis usage of any of the complementary and alternative medicine types (Supplementary Table 1).
Discussion
Our study has shown that health status, educational level, age, and living location were the significant factors that associated with complementary and alternative medicine usage for either general health maintenance or disease treatment. Education level is the strongest determinant of complementary and alternative medicine usage (OR = 2.03-3.12), followed by living location (OR = 1.55). In addition, the strength of effect for age is increasing by increasing of age (OR = 1.15-1.95). The reasons that might influence this are discussed later in this section. The types of disease diagnosed determined the usage of different types of complementary and alternative medicine.
The prevalence of complementary and alternative medicine usage among patients with diabetes and hypertension in our study was slightly lower compared with previous studies conducted in similar populations but higher in hypercholesterolemia and cancer. 5–9 The inconsistency was probably due to different study design where our study was based on cohort while other studies were in clinical settings. This study demonstrated that complementary and alternative medicine usage in general was higher among those with the following characteristics: female, Chinese, higher education level, lived in urban area, and older age group. The use of natural products was the only complementary and alternative medicine that showed association with at least one of the sociodemographic factors with the postdiagnosis usage for all the selected chronic diseases (hypertension, hypercholesterolemia, and diabetes) except for cancer. Among hypertensive, hypercholesterolemia, and diabetic subjects, those who used natural products postdiagnosis had a similar pattern of characteristics; they had lower education level, lived in rural area, and were older in age. The only difference was their ethnicity; Malays had higher odds of starting natural products after the diagnosis of hypertension, whereas Indians started after the diagnosis of hypercholesterolemia. A cross-sectional study conducted in similar population also supported this finding where complementary and alternative medicine users in hypertensive patients were predominantly Malays. 6
Disparity in the pattern of complementary and alternative medicine used between the general population and postdiagnosis of chronic diseases might be because the highly educated participants used complementary and alternative medicine to maintain their general health rather than to treat a disease. 18–20 We postulated that higher probability of complementary and alternative medicine usage might be influenced by higher health awareness among those who were highly educated with higher income that those who usually live in urban areas compared to those in rural areas. Furthermore, education levels might be seen as an indicator of information access of the knowledge of health benefits of complementary and alternative medicine that led to its usage. 19 Thus, the higher odds of Chinese using complementary and alternative medicine in general might reflect their higher health awareness. 21
Conversely, those who used complementary and alternative medicine after being diagnosed of chronic diseases were mainly less educated and lived in rural areas. This is consistent with previous studies that adults living in rural areas have lower knowledge and awareness toward their disease. 22,23 The majority of the rural area subjects were involved with agriculture for their livelihood; most were settlers at the Malaysian government’s Federal Land Development Authority agricultural scheme, which focused on rubber and oil palm. 12 The decision of complementary and alternative medicine usage among these groups might be influenced by the fact that chronic diseases are seen as incurable 6 and lead to their loss of trust in regular health care. 24 This is supported by a previous study, which found that 30% of chronically ill people were using complementary and alternative medicine to treat their disease. 24 Their easy access to complementary and alternative medicine–related natural products that can be collected or planted in their surrounding environment might further influence their postdiagnosis complementary and alternative medicine usage. 6 That older people were more likely to consume herbal and natural products compared to younger participants might be due to their knowledge (and belief) in traditional remedies to cure chronic diseases. Although socioeconomic status was not taken into account in this study, lower education level and older age might reflect low socioeconomic status, which influence the use of complementary and alternative medicine rather than conventional medicine. 19 This pattern of complementary and alternative medicine usage might also be inclined by cultural backgrounds and shared beliefs of the affected individuals. 6,19,25
In this study, we were unable to detect association between several types of complementary and alternative medicine postdiagnosis usage and diseases. One of the reasons was misclassification bias of the type of complementary and alternative medicine. This is due to the complex nature of the typology of complementary and alternative medicine that differs based on cultural background, origin, and belief. The definition of complementary and alternative medicine itself is highly dependent on the unique rules and regulations that are applied to food and medicine in each country. For example, a single plant can be defined as food, functional food, dietary supplement, or herbal medicine in different countries. This makes it difficult to define the concept of herbal medicines for the purpose of national drug regulation. 1 Other biases that existed in this study were recall and reporting biases, which is the weakness of self-reported questionnaires. These biases are known to reduce the power of the study in detecting true associations. Despite all the biases and weaknesses of this study, to our knowledge the present study is the first large prospective population-based cohort study in Malaysia that has comprehensive assessments of exposure, diet, and physical activity on top of the largest repository of biological specimens (blood and urine) in the country. 12 In addition, several innovative technologies were used in our TMC study to ensure data quality including “e-questionnaire” (the questionnaire was downloaded to tablet PCs and used by the enumerators to interview the participants) and in-house Cohort Information Management System, which manages many key aspects of the study including registration, questionnaire data, biophysical data, results of blood tests, biobank, and follow-up data as well as extensive quality control of data including listening to audio recording of interviews to detect and correct errors and checking of biophysical data. 12
Conclusion
In conclusion, health status, educational level, age, and living location are the significant factors that influence complementary and alternative medicine usage for the intent of either general health maintenance or disease treatment. The usage of different types of complementary and alternative medicine is highly dependent on the types of disease diagnosed. Cultural beliefs and ethnic background also play a role in complementary and alternative medicine usage. Future investigation on complementary and alternative medicine’s safety and benefit are important to minimize the adverse effect, to ensure the efficacy of the complementary and alternative medicine product, and to provide education to patients as well as health providers.
Supplemental material
Supplemental Material, Supplemental_Material_765945 - Utilization of Complementary and Alternative Medicine in Multiethnic Population: The Malaysian Cohort Study
Supplemental Material, Supplemental_Material_765945 for Utilization of Complementary and Alternative Medicine in Multiethnic Population: The Malaysian Cohort Study by Noraidatulakma Abdullah, Boekhtiar Borhanuddin, Afzan Effiza Abdul Patah, Mohd Shaharom Abdullah, Andri Dauni, Mohd Arman Kamaruddin, Shamsul Azhar Shah, Rahman Jamal in Journal of Evidence-Based Integrative Medicine
Footnotes
Acknowledgments
We thank all UKM Medical Molecular Biology Institute (UMBI) and The Malaysian Cohort staff members and research assistants. The voluntary participation of all the subjects is greatly appreciated.
Author Contributions
RJ contributed to the design, implementation of the research, and was in charge of overall direction and planning. MSA, AD, and MAK performed the measurements. AEAP and MSA provided the data. BB and NA performed the analysis. NA interpreted the results and drafted the manuscript. RJ and SAS provided critical manuscript revision. All authors approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Malaysian Cohort Study was supported by a top-down grant from the National Biotechnology Division, Ministry of Science, Technology and Innovation (MOSTI), Malaysia (ER-05-01-02-MEB001).
Ethical Approval
Ethical approval was granted by the institutional review and ethics board of Universiti Kebangsaan Malaysia (Project Code: FF-205-2007), in accordance with the Declaration of Helsinki. All subjects gave their written consent prior to study.
Supplemental material
Supplementary material for this article is available online.