
Abstract
Terror-management theory (TMT) proposes that when people are made aware of their own death, they are more likely to endorse cultural values. TMT is a staple of social psychology, featured prominently in textbooks and the subject of much research. The implications associated with TMT are significant because its advocates claim it can partially explain cultural conflicts, intergroup antagonisms, and even war. However, considerable ambiguity regarding effect size exists, and no preregistered replication of death-thought-accessibility findings exists. Moreover, there is debate regarding the role of time delay between the manipulation of mortality salience and assessment of key measures. We present results from 22 labs in 11 countries (total N = 3,447) attempting to replicate and extend an existing study of TMT, Study 3 from Trafimow and Hughes, and the role of time-delay effects. We successfully replicate Trafimow and Hughes and demonstrate that it is possible to prime death-related thoughts and that priming is more effective when there is no delay between the priming and outcome measure. Implications for future research and TMT are discussed.
Keywords
One unique aspect of the human experience is humans’ recognition that death is inevitable. Terror-management theory (TMT) proposes that this awareness is a central feature of human psychology and that cognitive discomfort arises when people are reminded of the certainty of their own death. In an effort to alleviate this discomfort, humans create a culture of values to create feelings of purpose beyond simple survival (Rosenblatt et al., 1989). Terror-management studies often involve invoking some form of mortality salience: reminding participants, through a questionnaire or exercise (often a writing assignment), of their own unavoidable death. Most studies then go on to measure some outcome that is assumed to vary with this mortality salience, such as social judgments (e.g., Jonas et al., 2008), support for political leaders (e.g., Landau et al., 2004), or willingness to serve in the military (e.g., Taubman-Ben-Ari & Findler, 2006).
Per Google Scholar, at the time of this writing, the article originally proposing TMT (Greenberg et al., 1986) has garnered 1,979 citations, and the first empirical test of TMT (Rosenblatt et al., 1989) has been cited 1,041 times. However, there is considerable variance in effect sizes between mortality-salience groups and all other experimental groups, 1 and numerous studies have reported small effect sizes. In addition, the existing literature exhibits a wide range of sample sizes (e.g., the original study by Rosenblatt et al., 1989, collected data from only 32 participants; subsequent studies have used samples as small as 17 participants; see Burke et al., 2010). Given the negative relationship between sample size and effect size (Burke et al., 2018; Schindler et al., 2023; Slavin & Smith, 2009), we believe this research may suffer from inflated estimates of effect size because of a combination of publication bias against null findings and small sample sizes in published studies (Gelman & Carlin, 2014). Finally, recent preregistered replication attempts (Sætrevik & Sjåstad, 2019; Schindler et al., 2021) have failed to replicate key elements of TMT.
In addition to variability in effect-size estimates, there is also debate over the role of time-delay effects on mortality-salience induction. Some studies (e.g., Das et al., 2009; Greenberg et al., 1994) have found that death primes have an immediate effect on death-thought accessibility (i.e., the ease with which one may access death-related concepts, often operationalized with a word-fragment-completion task; for an example, see Greenberg et al., 1994) and worldview defense. Others (e.g., Cohen et al., 2013; Hirschberger et al., 2008) have found that the effect of death primes is apparent after a delay. At present, there is considerable disagreement about the role of time delay in the relationship between mortality salience and death-thought accessibility (Steinman & Updegraff, 2015).
The goal of the present article is twofold. First, we sought to test the time-delay hypothesis by performing a direct, multilab, registered replication and extension of Study 3 from Trafimow and Hughes (2012). In this study, participants were asked to write about either their own death or dental pain (the control condition). They were then randomly assigned to either immediately perform a word-fragment-completion or word-generation task (with the number of death-related words being a measure of mortality salience) or to do so after reading and evaluating an unrelated article (to introduce a delay between mortality-salience induction and the measurement of mortality salience). Trafimow and Hughes concluded that contrary to what most TMT theorists expect, death-thought accessibility was actually lower when a delay was inserted between a mortality-salience manipulation and the measurement of death-thought accessibility. We selected this experiment because of ease of replicability among multiple labs (including those not in the United States) and because it investigates key components of TMT: a mortality-salience induction, a measurement of death-thought accessibility, and a delay between the mortality-salience manipulation and measurement of death-thought accessibility. Although other terror-management studies have examined subsequent effects of mortality salience on the endorsement of social norms, in-group preference, and so on, we chose this study because it focuses on death-thought accessibility, which is assumed to be the mechanism through which mortality salience affects other variables of interest. To the best of our knowledge, there is no existing preregistered replication of this study.
The replication of Trafimow and Hughes (2012) also affords an opportunity to obtain an effect-size estimate for the basic impact of mortality-salience induction on death-thought accessibility (the basis of all terror-management research). Thus, a secondary goal of the present study is to determine with precision the extent to which mortality-salience tasks can increase death-thought accessibility. The Registered Replication Report format allays concerns about publication bias and procedural overfitting and provides unique insight not attainable through traditional approaches, such as meta-analysis.
Before collecting data, Drs. Trafimow and Hughes were in contact with S. C. Rife and provided necessary materials that were not publicly available. In consultation with our editor, they reviewed the proposed protocol and made recommendations for changes, all of which were made. Our protocol deviated from the original study in a number of minor ways. First, to allow a wide range of laboratories to participate, the coding of the outcome measure (see below) was automated in that key words were detected as part of the analysis process. Second, because TMT is widely known and taught in introductory psychology classes, we included a measure of familiarity with the theory at the end of the survey. Third, to better assess the extent to which time-delay effects affect mortality salience, we implemented a timing feature through our survey software that measured the delay between the mortality-salience induction and the measure of death-thought accessibility. This measure was unknown to participants. Finally, because some labs were in countries where English was not the first language of a majority of students, translations of the original materials were made by the participating labs.
The most significant deviation from the original study relates to the outcome (death-thought accessibility) measure. Trafimow and Hughes (2012) employed a word-creation task that asked people to arrange a set of letters into five different words and then coded the responses as either death-related or nondeath-related. Although this approach is a potentially valid method of assessing death-thought accessibility, it is not the most common in the terror-management literature. 2 A more common approach is to have participants complete a set of 25 words with empty characters, six of which could potentially be death-related. To simultaneously (a) conduct an exact replication of Study 3 from Trafimow and Hughes and (b) test TMT using the most common operationalization of death-thought accessibility, we randomly assigned participants to complete either a word-creation task or word-fragment-completion task.
Method
All data and materials related to this report are available on OSF at https://osf.io/atc39. A preregistration of the protocol, made before data collection began, is available at https://osf.io/h5rcu (see also an update to this registration at https://osf.io/2vunx, which includes the study protocol and predata-collection manuscript). The code used to clean and merge data from each lab is available at https://osf.io/hrq9e, and the code used in all exclusions and analyses is available at https://osf.io/7um43. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Sample size and characteristics
To determine the optimal sample size and minimum number of participating labs for the proposed replication effort, we simulated meta-analyses with various parameters (code available at https://osf.io/dnf2j). To reduce the likelihood of a Type II error, our parameters were deliberately conservative. We determined that a minimum of 13 labs with a minimum of 100 nonexcluded (see below) participants each would be necessary to detect a Cohen’s d of 0.19—half the effect size reported by Trafimow and Hughes (2012; 0.36 more death-related words in the mortality-salience/no-delay group compared with all other groups; this is equivalent to a Cohen’s d of 0.37, 95% confidence interval [CI] = [0.00, 0.73]), with .95 power. This simulation assumed each lab would recruit up to 200 participants divided into four separate groups and compared values from an experimental delay group (25% of the simulated data) with all other groups (75% of the simulated data) using values reported in the original article. Given that all other analyses would have more balanced designs (comparing data from one half of the data set with the other; see below), this analysis assumed circumstances least favorable to detecting differences between groups among all the analyses in the present article.
A review of recent terror-management publications indexed by PsycINFO (Dunne et al., 2015; Echebarria Echabe & Perez, 2015; Finch et al., 2016; McCabe et al., 2015; Rogers et al., 2016) indicates that it is common for research in this area to assess sex and age. Thus, a brief demographic questionnaire was included at the end of the study.
Materials and procedure
Data from all labs were collected through an online survey platform (https://surveys.lyceum.ws) provided by the lead lab. All labs recruited participants from their respective participant pools, and data collection took place over the Internet without the supervision of an experimenter. After signing up for the study, participants were immediately directed to a link to the study. This link was unique to each participating institution and allowed participating labs to customize materials (e.g., the informed-consent form) to maintain compliance with their institutional review boards.
Writing prompts
After completing a consent form, participants were first directed to one of two randomly assigned prompts. In the experimental condition, they were asked to “Please briefly describe the emotions that the thought of your own death arouses in you” and provided with a large text box to provide their response. They were also asked to “Write, as specifically as you can, what you think will happen to you as you physically die and once you are physically dead” and provided with a second box for their response. Both prompts are designed to force participants to contemplate their mortality by describing key elements of their death. In the control condition, participants were asked the same questions but relating to dental pain rather than death (i.e., “Please briefly describe the emotions that the thought of dental pain arouses in you” and “Write, as specifically as you can, what you think happens to you as you physically experience dental pain and once you have physically experienced dental pain”) and provided with identical boxes for their responses.
Death-thought accessibility
After completing the writing portion, participants were randomly assigned to either (a) proceed immediately to a death-thought-accessibility assessment or read a brief news article about a renovated hotel and answer four related questions. All participants were then randomly assigned to complete one of two death-thought-accessibility tasks. In one condition, participants were asked to complete a word-generation task that asked them to arrange the letters “C O B U R E S A T K I L D H P L M G V” into five separate words and were provided with a box for each response. Each participant received a score (range = 0–6 3 ) based on the number of death-related words they provided. In the other condition, participants were asked to engage in a word-fragment-completion task in which participants were asked to fill in 25 words with missing letters, six of which could be death-related (see Table 1). Each participant received a score (range = 0–6) based on the number of death-related words they provided. Translations for both tasks are available in the project’s OSF repository (see above). For both tasks, death-related words were automatically detected; in the word-completion task, specific letters and whole death-related words were detected, and in the word-generation task, any death-related word in the LIWC dictionary for a given language (see Pennebaker et al., 2007) of death-related words was detected.
Death-Related Words (English) From Word-Fragment-Completion Task

Demographics and confounds
A final section of the study asked participants to indicate their gender and age for descriptive purposes and (a) if they were able to determine the purpose of the study (and if so, what it was), (b) whether they had trouble understanding the instructions provided, and (c) if they had ever heard of terror management or death-thought accessibility.
After data collection was complete, the relevant data were extracted (code available at https://osf.io/hrq9e) and analyzed (code available at https://osf.io/7um43).
Exclusion criteria
Participants were removed from the final version of the data set for a variety of reasons. First, TMT is frequently taught in introductory psychology courses, and awareness of the theory could compromise results. Thus, participants who indicated that they were aware of TMT during data collection (e.g., because it was already discussed in a class) or were otherwise aware of the goal of the study were excluded. Second, participants were excluded if they did not follow instructions (e.g., responded to the writing prompt with an essay that was not linked to the topic of death or dental pain), indicating that they did not understand the instructions presented. Third, participants were removed if they did not complete all tasks (e.g., left one or more questions blank), indicating that they were not appropriately attentive to the tasks. Finally, participants were removed if they completed the entire study in fewer than 5 min, as recorded by the survey software, indicating that they were not spending enough time attending to the tasks. All exclusion decisions were automatically based on participants’ responses (or nonresponses) to questions at the end of the study.
Preregistered analysis plan
We preregistered our analysis plan (available at https://osf.io/h5rcu). Consistent with the analyses employed by Trafimow and Hughes (2012), a meta-analysis comparing the average number of death-related words provided by participants in the mortality-salience no-delay condition with the average number of death-related words in all other conditions (death/no delay, dental pain/no delay, and dental pain/delay) was conducted.
In addition to the test that replicated the original finding by Trafimow and Hughes (2012), we conducted three additional analyses. First, given that the original study employed a somewhat nontraditional analysis (comparing death words in the no-delay condition with all other conditions), we conducted a t test comparing death-related words in the treatment, delay group with death-related words in the treatment, no-delay group. Second, to test the overall effect of the mortality-salience manipulation, we ran a comparison of the number of death-related words provided by participants in both mortality-salience conditions (delay and nondelay) with the number of death-related words provided by participants in the control conditions (delay and nondelay). All analyses were performed using both the word-generation task from the original experiment and the more common word-fragment-completion task. A full description of all analyses is presented in Table 1.
Results
Primary analyses
All data sets and analysis scripts are available on OSF at https://osf.io/atc39. A total of 22 labs 4 collected data from a total of 4,641 participants (N = 3,415 after select participants were excluded; see above). Participant characteristics (sex and age) from all labs (see Table 2) are roughly consistent with those reported by Trafimow and Hughes (2012). Descriptive statistics for each lab are presented in Table 3.
Descriptive Data by Lab

Note: BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.
Planned Comparisons by Group and Dependent Variable

We first attempted to replicate the findings reported by Trafimow and Hughes (2012). Results from a random-effects meta-analysis using the word-generation task as a measure of death-thought accessibility are presented in Table 4 and Figure 1. One lab, METAlab, had to be excluded from this analysis because of an insufficient number of cases in one of the conditions. Fourteen of the labs reported results that were in the direction of the original hypothesis, four of which were statistically significant. Only five of all labs reported results in the opposite direction, only one of which was statistically significant. Across all participating labs, an average of 0.08, 95% CI = [0.01, 0.14], more death-related words were recorded by participants in the “other” condition compared with the pooled no-delay condition—a significant difference. As shown in Figure 1, heterogeneity of effect size was considerable, τ = .12, I2 = 77.77%, H2 = 4.5, Q19 = 71.87, p < .001. Because of one lab, Kassel Lab, reporting no death-related words on the word-generation task, this site was excluded from the test for heterogeneity but is included in the forest plot (this is the case for all subsequent heterogeneity tests using the word-generation task). The relationship between the time delay (as a continuous variable, measured by the amount of time participants spent on the page with the article and associated questions) and death-thought accessibility was statistically significant, b = −0.07, SE = 0.03, z = −1.97, p = .04. See Figures 2 and 3, which depict the word-generation task and the word-fragment-completion task, respectively (we also generated the same graphs using local-weighted regression to further interrogate this relationship; results are available on this project’s OSF page).
Differences in Death-Thought Accessibility by Experimental/Control Conditions by Lab (Word-Generation Task)

Note: Mean and standard deviation from the original study are averaged between the three groups (mortality salience/delay, dental pain/delay, and dental pain/no delay) in the “All other groups” category. However, Tramafow and Hughes (2012) did not report how many participants were in each group, so these numbers assume an equal distribution between the three. BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.

Forest plot of replication analysis (word-generation task as dependent variable).

Relationship between time delay and death-thought accessibility by lab (word-generation task as dependent variable).

Relationship between time delay and death-thought accessibility by lab (word-fragment-completion task as dependent variable).
Additional analyses
To obtain an effect-size estimate for the impact of mortality-salience inductions on death-thought accessibility and address the validity of TMT in a general sense, we examined differences between the mortality-salience (writing about your own death) and control (writing about dental pain) conditions, measuring outcomes on both dependent variables. As shown in Table 5 and Figure 4, for the word-generation task, participants who were assigned to write about their death (regardless of whether they were in the delay condition) provided an average of 0.06, 95% CI = [0.01, 0.10], more death-related words than participants in the control condition; five labs reported the expected, significant results, and the remainder had CIs that crossed zero. There was significant heterogeneity between data-collection sites, τ = .08, I2 = 67.12%, H2 = 3.04, Q20 = 56.62, p < .001. For the word-completion task, two labs produced the expected results, with the remaining CIs crossing zero (see Table 6 and Fig. 5). Participants in the death condition provided an additional 0.17, 95% CI = [0.06, 0.29], death-related words. Tests for heterogeneity were also significant, τ = .20, I2 = 62.72%, H2 = 2.68, Q21 = 51.46, p < .001.
Differences in Death-Thought Accessibility by Experimental/Control Conditions by Lab (Word-Generation Task as Dependent Variable)

Note: BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.

Forest plot of comparison between death-prime conditions (word-generation task as dependent variable).
Differences in Death-Thought Accessibility by Experimental/Control Conditions by Lab (Word-Fragment-Completion Task as Dependent Variable)

Note: BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.
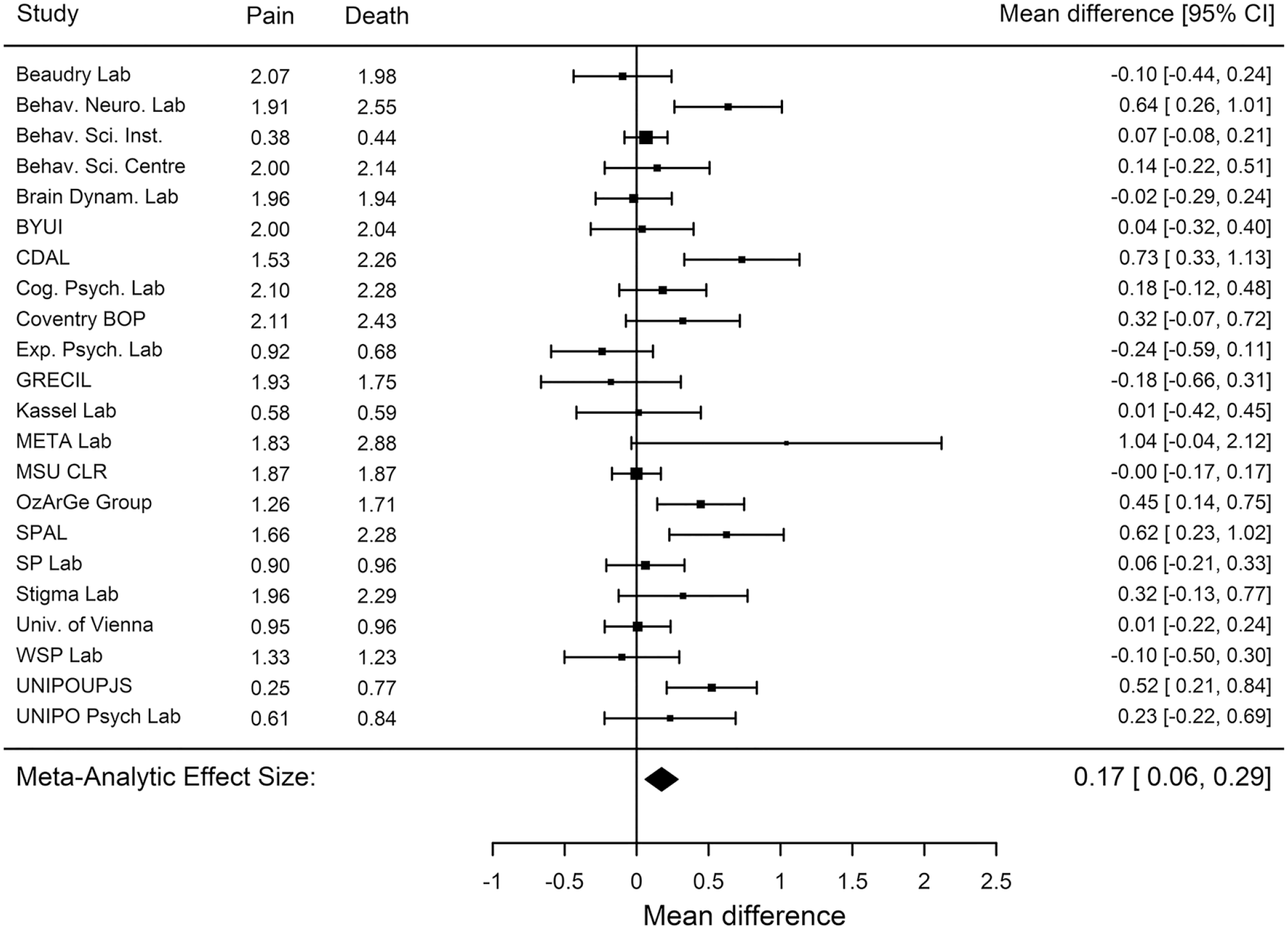
Forest plot of comparison between death-prime conditions (word-fragment-completion task as dependent variable).
Finally, we conducted a straightforward comparison of the delay/no-delay mortality-salience-induction groups on both dependent variables. This is a deviation from the analysis performed by Trafimow and Hughes (2012), who compared word counts in the delay/death group with all other groups (no delay/dental pain, delay/dental pain, no delay/death). Results for the word-generation task are presented in Table 7 and Figure 6. Eight labs reported significantly more words in the no-delay condition compared with the delay condition; only one reported more in the delay condition, and the rest had CIs that included zero. Overall, participants in the delay condition generated −0.11, 95% CI = [−0.02, −0.03], fewer death-related words than participants in the no-delay condition. Tests for heterogeneity between data-collection sites were significant, τ = .21, I2 = 93.3%, H2 = 14.92, Q17 = 158.54, p < .001. Statistically significant results in favor of the no-delay condition were also obtained using the word-completion task (see Table 8 and Fig. 7): Across all labs, an average of −0.2, 95% CI = [−0.31, −0.08], fewer death-related words were recorded by participants in the delay condition compared with the no-delay condition; nine labs reported significantly more death-related words in the no-delay condition, and the remainder had CIs that include zero. There was significant heterogeneity between data-collection sites, τ = .23, I2 = 76.39%, H2 = 4.24, Q21 = 80.78, p < .001.
Differences in Death-Thought Accessibility by Experimental/Control Conditions by Lab (Word-Generation Task as Dependent Variable)

Note: BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.

Forest plot of comparison between delay/no-delay conditions (word-generation task as dependent variable).
Differences in Death-Thought Accessibility by Experimental/Control Conditions by Lab (Word-Fragment-Completion Task as Dependent Variable)

Note: BYUI = Brigham Young University, Idaho Lab; CDAL = Cognitive Development and Aging Lab; Coventry BOP = Coventry Business and Occupational Psychology Lab; GRECIL = Grup de Recerca en Cognició i Llenguatge; METAlab = Memory, Emotion, Thought Awareness Lab; MSU Close Relationships Lab = Michigan State University Close Relationships Lab; OzArGeGroup = Özdoğru Research & Development Group; SPAL = Social and Personality Analytics Lab; SPlab = Social Psychology Lab; UNIPO Psych Lab = University of Presov Psychology Lab; UNIPOUPJS = Institute of Psychology, University of Prešov, Pavol Jozef Šafárik University.

Forest plot of comparison between delay/no-delay conditions (word-fragment-completion task as dependent variable).
Post hoc analyses
After data analyses concluded, a number of questions arose regarding low death-related response rates, particularly for German-language participants assigned to complete the word-generation task. Thus, we reran all the analyses presented above (a) with German-language participants removed and (b) using only English-language participants. These analyses presented results consistent with the original analysis, or what one might expect given the reduction in power associated with dropping participants from the analysis. Complete tables, plots, output, and code for all post hoc analyses are available as supplemental material available on the project’s OSF repository and Github repository.
Discussion
Across 22 labs, using data from 3,447 participants, we examined the extent to which death-thought accessibility after a mortality-salience induction is dependent on the passage of time. We replicated the findings of Study 3 from Trafimow and Hughes (2012), which found that participants in the no-delay condition produced more death-related words compared with participants in all other (death/delay, dental pain/no delay, and dental pain/delay) conditions. In addition, all other planned analyses showed evidence for successful death priming. We also produced evidence against the hypothesis that people initially suppress death-related thoughts given that participants who did not receive a delay between the writing task and the death-thought-accessibility assessment produced more death-related words than participants in the delay condition. These findings are in contrast to a large body of TMT literature that includes a delay and a meta-analysis (Steinman & Updegraff, 2015) that concluded studies that used a longer delay produced higher rates of death-thought accessibility. Indeed, in addition to finding that death-thought accessibility was higher in the no-delay group compared with the delay group, we also observed no consistent relationship between the amount of time participants spent in the delay condition—a finding directly at odds with Steinman and Updegraff (2015).
We also investigated a primary tenant of terror-management experiments: that thoughts about death can be induced through a writing task. We found that it was possible to successfully prime participants to think about death and that this finding is the strongest when there is no delay between the writing task and priming measure. This finding is, to a certain extent, in contrast to a number of recent failed TMT studies (e.g., Chew & Yap, 2022; Schindler et al., 2021; Treger et al., 2023), including a multilab project, ManyLabs 4 (Klein et al., 2022), which failed to replicate a seminal study in the TMT literature. 5 One key difference between the present study and that of Klein et al. (2022) is the outcome variable: In the present study, we directly assessed death-thought accessibility, whereas the failed studies examined worldview defense (e.g., Klein et al. assessed pro- and anti-American attitudes). Thus, one interpretation of these two findings is that death priming is possible but does not necessarily result in increased endorsements of a given cultural worldview, as suggested by the large body of published research on TMT (for a summary, see Burke et al., 2010).
However, even if one does assume that the hypothesized link between death-thought accessibility and worldview defense exists, a logical follow-up question is what effect size is necessary to generate said worldview defense. The effect size most favorable to TMT is 0.2 additional death-related words when a word-fragment-completion task is presented after a death prime as opposed to a control (dental pain). In practical terms, does this represent a meaningful increase in death-thought accessibility—one that would be expected to further lead to a measurable increase in worldview defense, across the wide variety of ways in which that outcome has been operationalized? If not, what effect size should one assume to be sufficient? It seems possible that even if the core tenants of TMT are correct, it may be difficult to induce a sufficient amount of death-thought accessibility using the instruments TMT researchers have traditionally employed. This interpretation reconciles the present findings with the replication failures discussed previously.
The finding that death-related thoughts are most accessible immediately after priming has some important implications for TMT more broadly. Greenberg et al. (1994) argued that because priming people to think about their death is unique—because humans are uniquely aware of their own mortality and motivated to avoid thinking about it—they will initially suppress death-related thoughts and that the effects of death-thought accessibility will emerge only after a short period of time has elapsed between the induction of mortality salience and measurement of the dependent variable. The present findings cast doubt on this interpretation because we show that death-related thoughts are most accessible immediately after people have been primed to think about their own mortality. One simple implication of these findings could be that TMT researchers should modify their protocols and remove any delay between the induction of mortality salience and the measurement of their outcome variables.
It is also possible to interpret these results in a manner more critical to TMT. The procedure of having people think about a concept (in the case of TMT, death) and then assessing the ease with which that concept (or related concepts) can be accessed is a well-established paradigm: priming. Despite recent failures to replicate key studies in social/behavioral priming (see e.g., Doyen et al., 2012; Pashler et al., 2012; Schindler et al., 2023; for replies and a recent discussion, see also Sherman & Rivers, 2021), it seems possible that more straightforward examples (e.g., semantic priming) are real phenomena. Thus, the present results can be viewed as a relatively mundane instance of successfully priming people to think about death—one that can be grouped with the large literature indicating it is possible to prime people to think about any number of concepts. However, this interpretation is inconsistent with the idea—advanced by TMT researchers—that death is a unique concept and one that can affect a wide array of outcomes and be moderated by an even larger number of variables. Future research should address this concern head-on by (a) attempting to replicate TMT findings without the use of a delay and (b) comparing the effect sizes of death-thought accessibility with other concepts (those not related to death). Suppose subsequent research indicates that expected behaviors do not emerge after death primes even when the delay is not included and that the effect size of death-thought accessibility is comparable with the priming of other concepts. In that case, it may be appropriate to conclude that as a concept, mortality is not as unique as TMT theorists suggest.
Limitations
The present research is limited in a number of ways, many of which are common to psychological research. First, although data were collected from a variety of countries and cultures, all participants were college students. Thus, findings should not be generalized to noncollege populations. Second, although every effort was made to ensure that translations of study materials were accurate, it is possible that some items were not faithfully translated (however, the fact that our conclusions held even when a post hoc analysis of English-only labs was performed seems to allay these concerns). Finally, although the total sample size was large, there was considerable variance in sample size across labs, with some recruiting fewer than 60 participants.
What is potentially the most consequential limitation, however, is the period during which data were collected. Data collection began in spring 2020 and continued for approximately 1 year across study sites. This period coincided with the COVID-19 pandemic and a significant amount of social unrest in the United States and elsewhere. We initially attempted to track the course of campus closures and other pandemic-related interventions at each study location (see https://osf.io/atc39/wiki/COVID-19%20Notes/) as part of a larger effort to analyze differences in findings based on the date range of data collection for each study site. In practice, this proved difficult to implement for all participating labs because the pandemic imposed considerable constraints on university faculty, who were already juggling a large number of responsibilities that were exacerbated by the pandemic. Much has been written about the COVID-19 pandemic from the perspective of TMT (e.g., Chew, 2022; Kuzhabekova, 2023; Li et al, 2021; Pyszczynski, et al., 2021; Shao et al., 2021). Overall, it seems that the impact of conducting a TMT study during a pandemic should be that death is already salient (because of ever-present reminders of the illness, media coverage, etc.), which would, in theory, increase death-thought accessibility (but see Schindler et al., 2021, who presented evidence to the contrary). Thus, the effects we present should be viewed as potentially being higher than what one would expect if data were collected under normal circumstances.
Summary and future directions
Our findings suggest that it is indeed possible to increase death-thought accessibility using standard death-priming tasks—particularly the word-fragment-completion task—and that inducing a delay between the death prime and assessment may decrease death-thought accessibility. Given that we find larger effect sizes when using a word-fragment-completion task, future terror-management studies should favor this outcome variable and avoid inserting delays between presentation of death primes and outcome measurement. However, given the failed TMT studies discussed previously, it is an open question whether the ability to increase death-thought accessibility actually results in the endorsement of culturally bound norms in an effort to reduce death-related anxiety, as TMT claims. Indeed, this is a strong claim, and the distance between priming death-related thoughts and the outcomes TMT predicts may be vast. In short, given the broader literature, it seems likely that although death-thought accessibility may be increased through experimental manipulations, the attitudinal and behavioral predictions postulated by TMT may not, in fact, emerge.
Footnotes
Acknowledgements
We thank David Lishner and Christopher Groves for bringing an error in an earlier version of the analysis code to our attention. We also thank Geoff Cumming and Wolfgang Viechtbauer for their assistance with analytical design.
Transparency
Action Editor: Katie Corker
Editor: David A. Sbarra
Author Contributions