
Abstract
Global vaccine hesitancy, intensified by crises such as the COVID-19 pandemic, represents a significant threat to immunization coverage. This narrative review discusses immunization safety monitoring frameworks and vaccine hesitancy in crisis-affected regions, particularly in Lebanon, Ukraine, and Sudan. By examining and reflecting on these case studies, this review aims to examine challenges, highlight context-specific strategies, and propose solutions for enhancing vaccine uptake and trust in fragile and conflict-affected areas. A structured narrative review was conducted, collecting evidence from global frameworks and region-specific case studies. The review explored factors impacting vaccine hesitancy, the role of adverse events following immunization (AEFI) monitoring systems, and innovative technological interventions. Key sources included peer-reviewed articles, reports from humanitarian organizations, and systematic reviews. The review showed that vaccine hesitancy is affected by interconnected factors, including sociopolitical and cultural conflicts, and misinformation. Lebanon’s persistent economic and political instability, Ukraine’s disruptions caused by the ongoing war, and Sudan’s fragile healthcare infrastructure pose challenges to vaccine coverage. Successful interventions to address hesitancy included transparency in AEFI reporting, integration of real-time monitoring systems, and community-led initiatives. It is critical to mitigate vaccine hesitancy in crisis-affected regions through robust safety monitoring frameworks and tailored communication strategies. Global cooperation and frameworks, technological innovations, and context-specific approaches are imperative for improving the resilience of immunization systems and ensuring health security in fragile settings. Furthermore, these insights are crucial in informing public health communication policies and behavior change interventions to improve public trust and thus reduce vaccine hesitancy.
Plain language summary
Vaccines are one of the most effective preventive interventions for disease. However, vaccination is often resisted in crisis-affected countries. To identify common barriers and effective solutions to improve vaccine confidence, this study explores the role of vaccine safety monitoring and communication strategies in reducing vaccine hesitancy in Lebanon, Ukraine, and Sudan.
Keywords
Introduction: The global challenge of declining vaccine coverage
Vaccination is considered among the most effective public health interventions, having markedly reduced the burden of infectious diseases globally and avoided millions of deaths annually, thus contributing to remarkable gains in human health and life expectancy.1,2 Notwithstanding these successes and its proven efficacy, global vaccine coverage has significantly declined over the last few years, threatening to put global health safety at risk. For example, global coverage in childhood immunization, specifically the DTP3 vaccine dose, dropped from 86% to 81% between 2019 and 2021 worldwide, along with 14.5 million infants lacking the DTP1 vaccine dose and an additional 6.5 million partially vaccinated in 2023. 3
The decline in vaccine coverage originates from a combination of interconnected challenges, such as misinformation, systemic inequalities, and disruptions to healthcare infrastructures, with vaccine hesitancy playing a central role.4,5 In 2019, vaccine hesitancy was identified by the World Health Organization (WHO) among the top 10 threats to global health. 6
In fact, vaccine hesitancy is not to be treated as a singular problem but originates from an interplay of social, cultural, political, and economic factors. Safety-related concerns often play an important role in vaccine hesitancy, particularly in settings characterized by misinformation and a general distrust of the authorities. 7
The rise of social media has facilitated the rapid spread of misinformation and conspiracy theories associated with vaccines, consequently increasing anxieties about safety and creating an aura of fear and doubt about vaccination. 8 The COVID-19 pandemic further intensified these existing challenges, with significant disruptions in immunization programs in over 170 countries, contributing to the largest rise in unvaccinated children in three decades, with 25 million children in 2021 alone missing their routine vaccinations. 9 These disruptions were visible in fragile and conflict-prone countries, where health infrastructures are already stretched and access to essential services is limited. 10
Research showed that strengthening immunization safety monitoring can help address vaccine hesitancy and rebuild public trust in vaccination programs. Robust surveillance systems, including active and passive surveillance, adverse events following immunization (AEFI) monitoring, and pharmacovigilance frameworks, could play a central role in guaranteeing the safety of vaccines and providing evidence-based reassurance to the general public. 11 However, the underdeveloped data systems, inadequate infrastructure, and cultural resistance to external interventions pose significant challenges when implementing such systems in resource-limited and politically unstable regions.
To draw a deep understanding of the complex dynamics surrounding vaccine hesitancy and monitoring of immunization safety, this narrative review examines three different case studies: Lebanon, Ukraine, and Sudan. These nations, while they vary in their social-political landscape, present a particular context in which political instability, economic difficulties, war-related displacement, and cultural disparity have influenced perceptions about vaccines and the effectiveness of immunization programs.
By examining and reflecting on these case studies, this narrative review highlights the complex relationship between vaccine hesitancy and immunization safety monitoring in crisis-affected regions. This review also seeks to highlight the importance of including rigorous safety monitoring systems in vaccination programs, particularly in fragile and conflict-affected areas.
Methodology, approach, and literature basis
This narrative review was informed by a structured and integrative synthesis of relevant global evidence and context-specific challenges of vaccine hesitancy and AEFI monitoring, using a non-systematic approach. Findings were obtained from a total of 89 sources, including peer-reviewed articles, systematic and narrative reviews, gray literature, and reports from international and humanitarian organizations. These sources were identified through targeted searches of relevant databases based on keywords such as “vaccine hesitancy,” “immunization safety,” “AEFI monitoring,” “fragile health systems,” and country-specific terms such as “Lebanon,” “Ukraine,” and “Sudan.” Literature searches were conducted in PubMed, Scopus, and Google Scholar, supplemented by hand-searching reference lists and targeted searches of the official websites of the WHO, UNICEF, and the Center for Strategic and International Studies (CSIS).
Across these searches, approximately 220 records were initially identified. The selection of sources was based on their relevance to the topic and target regions, as well as being published in English. No restrictions were applied to publication year, but studies published after 2020 were emphasized due to the significant shift in vaccine attitudes during COVID-19. Exclusion criteria included publications unrelated to vaccines, immunization safety, or public health crises, editorials, letters, or opinion pieces, and non-English publications. Following screening for relevance, a total of 89 sources were included, classified into four categories based on document type and origin. Specifically, 41 were peer-reviewed original research articles; 12 were systematic or narrative reviews; 21 were reports and technical documents from humanitarian and international organizations; and 15 were gray literature (including conference proceedings, policy briefs, regional health bulletins) (Figure 1).
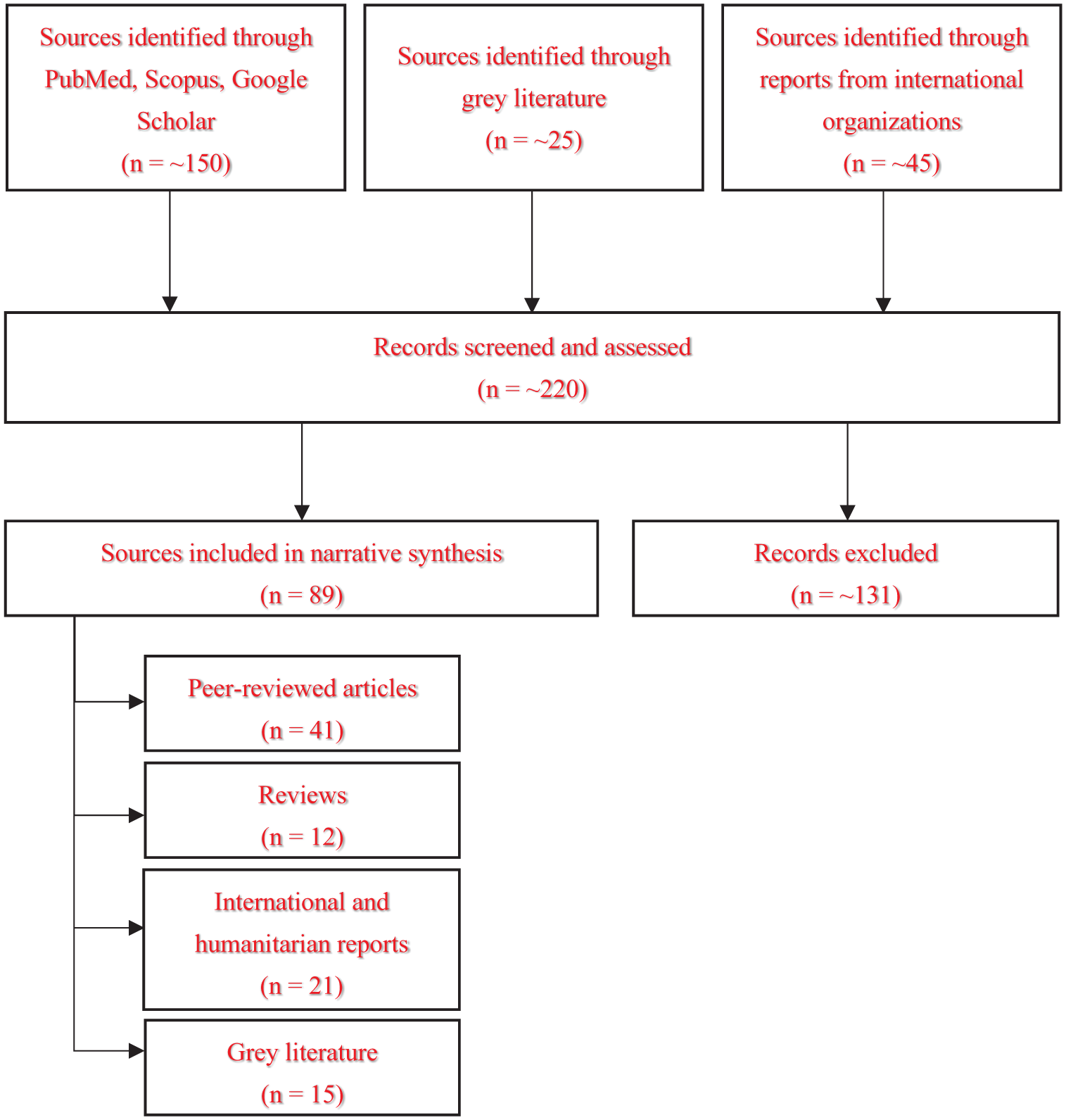
Schematic illustrating an overview of sources informing this narrative review.
Due to the narrative nature of this review, formal bias assessment or systematic quality appraisal tools were not applied, but efforts were made to rely primarily on peer-reviewed and credible evidence. 12 Our main objective was to generate practical insights into context-specific challenges and solutions by examining the major factors contributing to vaccine hesitancy in fragile and conflict-affected settings, how immunization safety and AEFI monitoring systems are structured, and what context-specific strategies have been effective in these regions, and what roles do global frameworks and digital innovations play in improving immunization trust.
Global overview of vaccine hesitancy as an obstacle to coverage
Vaccine hesitancy: Definition and primary drivers
The World Health Organization defines vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite availability of vaccination services.”13,14 It has become a crucial public health concern with potential medical, social, and economic consequences for global immunization efforts. 15 This complex phenomenon is shaped by several factors, ranging from individual beliefs to broader societal dynamics, making it a multifaceted problem requiring a comprehensive understanding and tailored interventions. 16 Several key factors characterize the global landscape of vaccine hesitancy. A recent study by Goje and Kapoor 17 mentioned that safety concerns are one of the primary reasons for vaccine hesitancy. As highlighted in the study, many individuals express their doubts about the potential side effects or long-term consequences of vaccination, especially newer vaccines such as those developed for COVID-19. These concerns are intensified by the rapid dissemination of false and misleading information through social media platforms that influence public opinion. 18 Furthermore, the growing distrust in medical and governmental authorities has undermined confidence in vaccination programs.16,19
To better understand vaccine hesitancy, several theoretical models provide valuable insights into its psychological and social dimensions. 20 For instance, the “3Cs model” identified three main factors: Confidence, Complacency, and Convenience. 14 Confidence is the belief in the safety and efficacy of vaccines, the dependability of medical systems, and the motivations of policymakers. Complacency arises when individuals perceive a low risk of contracting diseases that can be prevented by vaccination, reducing the urgency for vaccination. Convenience includes the accessibility, affordability, and availability of vaccines, with barriers including cost, complicated procedures, and distance to vaccination centers. 14
Other models, including the Health Belief Model (HBM) 21 and the Theory of Planned Behavior (TPB),22,23 delve deeper into behavioral and cognitive influences on vaccine decisions.
The HBM focuses on factors that impact decisions about health behavior. 21 It suggests that individuals’ perceived susceptibility and severity of a disease, and perceived benefits and barriers of the action, influence their likelihood of engaging in health-related behaviors, including the decision to vaccinate. On the other hand, the TPB focuses on factors including attitudes toward behavior (e.g., perceived value of vaccination), subjective standards (e.g., perceived social pressure to vaccinate), and perceived behavioral control (e.g., confidence in the ability to get vaccinated) that collectively affect behavior intention, and consequently, the health behavior. 22 Unlike the HBM, the TPB combines the impact of social and environmental factors on decision-making. Insights from these frameworks are crucial for crafting targeted strategies to enhance vaccination acceptance and uptake, as they shed light on how cognitive styles, perceptions of public health organizations, and information-processing skills affect vaccine hesitancy.
Trends in vaccination hesitancy varied markedly between low- and middle-income countries (LMICs) and high-income countries, as well as across various geographic and cultural contexts. In LMICs, vaccine hesitancy is caused by a multitude of factors, often aggravated by political unrest, economic instability, and cultural practices. 24 In addition to these structural and cultural factors, socioeconomic difficulties in LMICs, such as low income and education levels, restrict access to resources and accurate information. Gender-related barriers further limit women’s accessibility to healthcare information, while religious concerns regarding vaccine ingredients exacerbate hesitancy. 25 Regions undergoing political unrest or armed conflict face unique barriers, including safety concerns and interrupted healthcare systems.26,27
Conversely, in high-income countries, the advanced healthcare infrastructure improves the efficacy of vaccine administration and distribution. Higher education levels are generally correlated with increased acceptance of vaccines. 28 However, in some communities, vaccine hesitancy persists due to concerns about vaccine safety and side effects more than access or cultural barriers, as information accessibility, which can encourage vaccine acceptance, can also lead to the spread of misinformation, complicating the public health efforts.7,29
These frameworks highlight the significance of context-specific strategies and the complicated interactions among variables affecting vaccination hesitancy. To remove the barriers and increase vaccine uptake worldwide, it is crucial to develop tailored strategies that consider the distinct cultural, economic, and social circumstances of every region.
COVID-19’s role in amplifying preexisting vaccine reluctance
Although the main causes of hesitancy have remained relatively consistent over time, the dissemination of this information and its impact on public opinion have remarkably changed, mainly during the spread of the COVID-19 pandemic, which has significantly amplified preexisting vaccine hesitancy and risk perception, and catalyzed shifts in media narratives and public trust. 30 While the rapid development of COVID-19 vaccines was a remarkable scientific achievement, it also raised concerns about safety and efficacy, particularly among those already predisposed to doubt vaccines. 31
The evolving landscape of digital communication has generated what has been described as an “infodemic” characterized by an overabundance of information—both accurate and inaccurate—that fuels hesitancy.32,33
One major driver of this hesitancy has been the politicization of COVID-19 and vaccination efforts, which has deepened skepticism and distrust toward governments, health authorities, and pharmaceutical companies. Researchers in Iran, for example, found that one of the main causes of vaccine reluctance and refusal is mistrust of national media, pharmaceutical firms, and policymakers. 34 Similarly, in the United States, the politicization of the COVID-19 vaccine has not only shaped attitudes toward COVID-19 vaccines but also influenced skepticism about other vaccines, often aligning with political affiliations. 35 Comparative data from the United Kingdom and Australia also show that trust in governmental procedures is strongly linked to increased vaccine hesitancy. 36 Accordingly, this trend of mistrust, despite the nature of its causes, is a global phenomenon that affects vaccine confidence across diverse contexts.
In addition to these challenges, the shifting guidelines issued by health organizations during the COVID-19 crisis, combined with an overwhelming influx of information, deteriorated their trust in authorities and led to vaccine hesitancy. 37 This effect was observed across diverse societal groups and significantly impacted public health initiatives. The evolving framework of public health policies and practices created widespread confusion and uncertainty about the virus, vaccination, and the pandemic itself. Capacity problems, politics, lack of confidence, and conflicting news sources all contributed to this confusion and created a culture of skepticism regarding public health information. 38 In addition, some individuals were hesitant to receive the COVID-19 vaccine due to a perceived low risk of contracting the virus, particularly if they were younger or had no underlying medical conditions. 39
Globally, a comprehensive analysis of systematic reviews and meta-analyses on COVID-19 vaccine hesitancy highlights the complex interplay of factors influencing public health acceptance. Multiple studies have identified several psychosocial variables contributing to vaccine hesitancy, such as worries about vaccine safety and efficacy, the spread of misinformation, conspiracy theories, demographic variables, and socioeconomic conditions.40–42 A systematic review by Davey and Gaffiero 43 examined parental barriers to COVID-19 vaccination for children aged 5–11 in Western countries, highlighting the key impacts of safety concerns, misinformation, and lack of trust in government. Likewise, Chang et al. 44 found that familiarity and trust in vaccine producers, and perceived severity of disease, significantly affected decisions on newly developed vaccines in China.
The challenges of vaccine hesitancy highlight the intricate interplay of societal, psychological, and systemic influences. Addressing these issues requires a comprehensive and evidence-based approach that prioritizes trust, transparent communication, and culturally tailored strategies. By understanding and tackling these multifaceted challenges, public health efforts can pave the way for stronger vaccination campaigns and enhanced community resilience in the face of future pandemics.
Vaccine hesitancy and safety monitoring in crisis-affected regions: Lebanon, Ukraine, and Sudan
Vaccine hesitancy in crisis-affected regions such as Lebanon, Ukraine, and Sudan is shaped by intersecting factors, including economic hardship, misinformation, cultural resistance, and logistical constraints. Addressing these challenges highlights the importance of safety monitoring mechanisms tailored to each region’s unique context.
Transparency in vaccine safety monitoring is critical in addressing hesitancy and building confidence in immunization programs. Real-time safety data sharing through global systems like VigiBase have proven effective in addressing public safety concerns and holding health authorities accountable. 45
These efforts have been further strengthened by the efforts of NGOs and reliable institutions, which play a pivotal role in reinforcing safety monitoring frameworks and promoting vaccine trust.46,47 Below is a close examination of these contexts.
Lebanon: Economic instability and distrust in the authorities
In Lebanon, safety concerns, persistent economic instability, communication barriers, and the lack of trust in governmental institutions have eroded public trust in the public health system, fostering widespread vaccine skepticism. 48 Al Halabi et al. 49 investigated the willingness of Lebanese adults to receive the COVID-19 vaccine and the factors contributing to vaccine hesitancy. Among 579 participants, only 21.4% were willing to be vaccinated, while 40.9% refused. Findings revealed that key factors associated with vaccine hesitancy included negative attitudes toward vaccination, increased reluctance, and lower acceptance among females and married individuals.
Similarly, Zakhour et al. studied the hesitancy of 306 parents of children aged 3–18 regarding the HPV vaccine in Lebanon, highlighting a different but related aspect of the problem. 50 Their findings pointed to misconceptions about vaccine safety and the absence of robust public health campaigns, which contributed to lower-than-expected vaccine coverage. Notably, 60% of parents aware of the HPV vaccine chose not to vaccinate, citing lack of pediatrician recommendation and uncertainty about the vaccine’s safety as major reasons. The authors suggested targeted measures, including culturally sensitive messaging and improving public education, as effective solutions.
While vaccine hesitancy is prevalent among the general population, refugees in Lebanon, making up a significant portion of Lebanon’s population, face additional barriers, including limited access to health services and credible vaccine information. 51 According to IMPACT Open Data, the Lebanese eGovernance and COVID-19 tracking platform, only 2.86% of those vaccinated in Lebanon were not Lebanese nationals, though this category makes up at least 30% of the total population. 52 Factors influencing acceptance included perceived benefits, susceptibility to COVID-19, and barriers to vaccination. These challenges mirror, but also intensify, the systemic issues observed in the broader population.
To address these widespread challenges, Lebanon has implemented its first step for safety monitoring to restore public confidence in vaccines. The implementation faced initial setbacks due to political interference and widespread mistrust in government systems. To address these issues, the IFRC, through the World Bank, is upholding the implementation of third-party monitoring mechanisms and, thus, transparency. 46 Sharing the results of adverse events data and removing fears of vaccine safety have helped, in turn, to rebuild trust in public health systems. 53 These, combined with focused outreach programs, have helped to make vaccines more accessible and acceptable to those who are prey to diseases or refugees or migrant workers.
Ukraine: Disruption from conflict and misinformation
The ongoing war in Ukraine has affected the healthcare system of the country leading to the disruption of critical services and a significant rise in vaccine hesitancy and skepticism. 54 Even before the conflict, Ukraine had low vaccination rates, with only 20% of children fully vaccinated against measles and 13% against poliovirus. 55 The dual impact of the war and the COVID-19 pandemic has worsened the situation, causing population displacement, logistical barriers, and a breakdown of immunization services, further undermining the public trust in vaccines and health authorities.54,56 Research by Osborne et al. 57 investigated vaccine perceptions and uptake challenges in Ukraine, focusing on interviews with parents of young children, health practitioners, and local experts. Findings showed that mistrust in the health system and inadequate access to reliable information are key factors contributing to vaccine hesitancy in Ukraine. Internally displaced persons further faced multiple challenges, including limited access to healthcare services and exposure to false information. 58
Politically driven misinformation has fueled doubts about vaccine efficacy and adverse effects, significantly increasing vaccine hesitancy and highlighting the urgent need for robust safety monitoring systems to rebuild public trust. For example, research showed that many political figures in Brazil and the United States publicly questioned the vaccination safety or necessity during COVID-19, which contributed to widespread public skepticism along with partisan media and social platforms.59,60
During the COVID-19 crisis, the incorporation of real-time safety monitoring systems into the framework of humanitarian operations enabled timely responses to misinformation and demonstrated accountability. 61 By including these systems in health emergencies, Ukraine has followed procedures ensuring that safety data are captured and disseminated transparently despite the conflict.
Humanitarian organizations and local NGOs in Ukraine have also played a crucial role in addressing vaccine hesitancy. Joint projects with representatives of international organizations have helped disseminate accurate information on vaccine safety measures, emphasizing access to healthcare services in limited-access regions. 62 Such initiatives explain how real-time safety monitoring helps fix current safety issues in conflict areas while dealing with existing reluctance.
Sudan: Cultural resistance and fragile infrastructure
Overcoming vaccine hesitancy is a much greater challenge for Sudan, given its dire economic situation, internal conflict, and fragile healthcare system. 63 In fact, Sudan is among the countries with the highest numbers of zero-dose children, indicating a severe impact of conflict and weak infrastructure on vaccination-related programs. 3
Research by Raja et al. 64 revealed that 44.2% of surveyed medical students expressed reluctance to get vaccinated due to safety and efficacy concerns. Concerns about vaccine safety and effectiveness were prevalent among those hesitant to vaccinate. This directly aligns with international trends of vaccine mistrust, particularly for newer vaccines, where misconceptions and misinformation are regularly spread in rapid succession. 65 Similar trends were observed among healthcare workers, with 16% outright refusing vaccination due to perceived harm and distrust in vaccine sources and overseeing organizations. 66
Cultural norms and religious beliefs present additional barriers, particularly in rural areas. Sabahelzain et al. 67 explored the views of healthcare professionals and vaccine providers in Khartoum regarding the factors influencing measles vaccine hesitancy. Key findings highlight the presence of anti-vaccination perceptions among specific religious and ethnic groups, parental beliefs about alternative approaches to measles prevention and treatment, and concerns about the attitudes of vaccine providers and the effectiveness of the vaccine delivery system. Moreover, logistical challenges, including limited access to remote and conflict-affected regions, exacerbate these issues, leaving vulnerable populations without adequate vaccination services.63,68
To combat vaccine hesitancy, Sudan has implemented community-led initiatives that include local leaders in promoting vaccine safety and reporting adverse events to counteract vaccine hesitancy. 64 Furthermore, by enabling community health workers to respond quickly to events, safety monitoring systems have alleviated public concerns and promoted trust in vaccination campaigns. This approach has also served to ensure that the reliability of vaccine programs is perceived well while increasing vaccine distribution in hard-to-reach areas.
Furthermore, culturally sensitive vaccine communication efforts have demonstrated significant effectiveness in Sudan. While mobilization programs have aggressively sought to dispel misconceptions and encourage vaccine adoption, Sudanese authorities have collaborated with international groups to develop tailored messaging to meet cultural and religious barriers. 69 These methods highlight the need for localized strategies and sustained efforts in tackling the complex challenges of vaccine hesitancy across the nation.
Strategies for enhancing vaccine coverage in crisis-affected regions
Best practices from global success stories
Global immunization programs have relied heavily on monitoring AEFI, especially in the fight against diseases like polio. Authorized by the WHO in 2020, the introduction of novel oral poliovirus vaccine type 2 showed reduced neurovirulence and genetic stability, addressing the problems caused by circulating vaccine-derived polioviruses in areas with low immunization coverage.70–72
As demonstrated by successful campaigns in countries like Afghanistan and Nigeria, safety monitoring mechanisms like environmental surveillance and acute flaccid paralysis (AFP) surveillance have been essential in identifying and addressing polio cases.73,74 A review published in 2017 underscored the vital role of AFP inspection in following the progress toward global polio eradication by diligently detecting children with prompt-onset paralysis, followed by laboratory testing of stool samples to confirm the presence of the virus.74,75
These approaches were critical in documenting the elimination of wild poliovirus in Egypt and India and detecting poliovirus in polio-free countries such as Brazil, Israel, and Mexico. 74 Furthermore, Jorgensen et al. emphasized the role of genetic sequencing in improving virus detection, mapping transmission patterns, and guiding targeted vaccination plans. 76 The reviews highlight genetic testing’s capacity to identify the source of viruses and enhance vaccination programs, especially in regions where vaccine reluctance and logistical challenges are prevalent. 76 These resources work together to create an integrated framework that supports international polio eradication efforts.
Technological innovations and AI: Transforming vaccine distribution and hesitancy mitigation
Technological advancements have significantly improved immunization efforts in rural and resource-limited areas, overcoming obstacles such as limited healthcare infrastructure, geographic barriers, and staffing shortages. 77 Innovations in vaccine administration methods have improved accessibility and reduced reliance on traditional intramuscular injections by including nasal and oral immunizations using particulate delivery systems, microneedles, and thermostable vaccines. These technologies ensure regulated antigen release, eliminating the need for booster doses and reducing vaccine deterioration in difficult-to-reach areas. 78
In addition to delivery innovations, education and system-level investments have played a critical role. A meta-analysis of 120 studies revealed that vaccination education led to a 19% increase in overall vaccination coverage, provider interventions enhanced coverage by 13% and the most significant rise was achieved by financial incentives resulting in a 67% increase in vaccination coverage. 79 The WHO recommended the necessary investments to improve national vaccination programs through enhanced data systems for tracking vaccination status, planning for under-vaccinated groups, and advancing supply chains. 80
Mobile platforms and artificial intelligence (AI) have revolutionized vaccine distribution and tracking. Natural language processing (NLP) and AI-driven predictive analytics have proven crucial in detecting high-risk groups, dispelling misinformation on social media, and improving the quality of documentation.81–83 Drones have demonstrated efficacy in transporting medical supplies to remote areas, and automated sensors guarantee the integrity of cold chain systems by offering real-time data on storage conditions.84,85
Furthermore, AI-powered chatbots and culturally tailored communication strategies, especially in underprivileged areas, have addressed vaccine hesitancy by offering counseling, scheduling reminders, and providing accurate information.86,87 These tools can improve psychological capability (through information provision) and reflective motivation (through reminders) to support behavior change, as illustrated by the COM-B model, stating that behaviors (B) occur due to the interaction between capabilities (C), opportunities (O), and motivation (M). 88 However, the limited digital access and user trust in underserved contexts may hinder their effectiveness, where users may rely on familiar platforms (e.g., WhatsApp, Facebook) rather than AI interfaces to access information. Moreover, if not properly regulated, AI chatbots can spread misinformation and thus pose risks to these populations. 89
Together, these technological innovations, combined with WHO-recommended investments in immunization systems and education programs, have significantly increased vaccination coverage and reduced disparities globally.79,80
By making vaccination distribution and healthcare delivery more efficient, AI-powered solutions might lessen the impediments to predicting epidemics, allocating resources ideally, and enhancing supply chain effectiveness. However, the deployment of these tools must be associated with robust oversight, trusted communication channels, and community engagement.
Discussion
As the above sections reflect, addressing vaccine hesitancy and ensuring immunization safety, specifically in crisis-affected regions, is a multifaceted challenge that requires local and global coordination. This narrative highlights the crucial role played by AEFI monitoring systems in contributing to reduced vaccine reluctance and better public trust. However, these systems in conflict-affected regions often face a lack of resources, sociopolitical instability, and disrupted healthcare infrastructure. Key challenges include logistical, financial, and human resource limitations, public mistrust, and disrupted healthcare infrastructure.
Accordingly, overcoming these barriers and ensuring vaccine safety and acceptance requires prioritizing investments in vulnerable health systems, shifting to proactive strategies, designing context-specific communication strategies for conflict settings, and identifying sustainable financing mechanisms. 90 Public–private partnerships with humanitarian agencies and the community are also crucial in ensuring monitoring frameworks are suited to these dynamic, unforgiving environments. 91 Importantly, addressing these challenges must also include a focus on disrupted supply chains, inhospitable facilities, human migration, and mistrust in authorities in conflict settings. 92
Successful initiatives such as Gavi, the Vaccine Alliance, and the Global Polio Eradication Initiative have demonstrated the power of combined resources in enhancing vaccine surveillance and distribution networks within resource-constrained areas.93,94 This calls for exploring new financing approaches and international funding arrangements to ensure the sustainability of AEFI monitoring systems in resource-poor settings. 45
Moreover, technological advancements such as AI and mobile platforms offer promising opportunities for real-time data collection, visualization, and communication, particularly in low-resource regions. These tools can help improve transparency and acceptance of vaccines, as evidenced by their growing adoption in geographically and economically disadvantaged regions.95,96
The harmonization and standardization of practices in immunization also require strengthening the international policy frameworks and fostering global collaboration. Standardization of AEFI reporting forms, terminologies, and investigation frameworks across countries can enhance the comparability of data and strengthen international surveillance efforts. 90 Moreover, training programs for health professionals in crisis and conflict areas are integral to effectively identifying, reporting, and investigating AEFIs and overcoming hesitancy.
Implications for policy and practice
This narrative review implies that the resilience of immunization systems widely depends on sustainable global investment and cooperation. The findings discussed also provide multiple implications.
Global frameworks, such as safety strategies offered by WHO and UNICEF, require localization and adaptation to region-specific cultural, political, and logistical contexts. In addition, AEFI monitoring and surveillance systems, often overlooked in emergencies, must be prioritized in fragile settings for their key role in sustaining vaccine acceptance. Digital innovations can also bridge gaps in these settings, but should be scaled with proper infrastructure and policy support. However, the priority remains on community engagement, which causes even the best-designed systems to risk failure when public trust is lacking.
Recommendations and future directions
Below are key recommendations for strengthening AEFI monitoring frameworks, particularly in fragile and conflict-affected regions.
Prioritizing investments in healthcare infrastructure and ensuring that healthcare workers are well-trained helps guarantee the effectiveness of AEFI surveillance and monitoring. Strategies must also be developed with a focus on culturally sensitive communication and context-specific conditions and challenges, including population displacement and disrupted supply chains.
Developing user-friendly data visualization tools is also recommended to help policymakers and healthcare professionals disseminate reliable information, thus ensuring transparency and increasing public awareness and vaccine acceptance. In addition, there is an urgent need to promote efficient communication, international cooperation, and data sharing, particularly concerning transnational outbreaks and the introduction of new vaccines, for early identification and rapid responses to potential safety alerts. This also includes the active involvement and collaborative efforts of local communities, NGOs, and humanitarian agencies in conflict-affected areas, as well as designing research-informed, tailored interventions to address vaccine hesitancy.
Limitations
Despite the in-depth examination that this review provides, it is important to acknowledge several limitations. The challenges outlined in this review are not universal and can thus drastically vary among different regions and contexts. Further research should highlight region-specific case studies to develop contextualized solutions for different conflict and crisis-affected regions.
Data availability and comprehensive AEFI reporting systems are also limited and lacking in many crisis-affected areas, including Lebanon, Ukraine, and Sudan, which call for more robust data collection efforts in evaluating the effectiveness of current safety monitoring systems and identifying possible areas for improvement.
In addition, while the technological advancements discussed are effective, their implementation in conflict and crisis-affected areas can be challenged by the limited infrastructure and lack of technical expertise. Addressing these challenges is essential to guaranteeing the scalability and sustainability of these solutions. Future efforts must focus on developing operational frameworks for implementing digital AEFI systems and evaluating the real-world impacts of contextualized strategies in low-resource settings.
Conclusion
In conclusion, addressing vaccine hesitancy and improving immunization safety in crisis-affected areas requires global cooperation and frameworks, technological innovations, and context-specific approaches. The context of Lebanon, Ukraine, and Sudan reflects the unique vaccine hesitancy challenges in conflict settings, emphasizing the necessity of robust safety monitoring systems and increased public awareness. Mobile technologies and AI for real-time monitoring hold great promise for improving the efficiency of vaccination programs in conflict areas, in addition to tailoring culture-specific and context-relevant solutions that consider religious and cultural norms of the targeted population. These solutions, when coupled with global collaboration and standardized frameworks, can contribute to more resilient immunization programs and ensure that vaccines reach those who need them most.