
Abstract
Background:
Human papillomaviruses are the most common sexually transmitted infections, and persistent infection can lead to cervical cancer. In line with WHO recommendations to prevent cervical cancer, human papillomavirus vaccination is considered mandatory. Despite various challenges influencing decision-making for HPV vaccination, including HPV vaccine hesitancy, efforts are made to promote its uptake.
Methods:
A community-based cross-sectional study was conducted from March 1 to April 30 among 400 parents of adolescents. A simple random sampling technique was used to select study participants. A structured questionnaire was employed for data collection, and the data were gathered through interviews. Subsequently, the data were entered into EPI data 3.1 statistical software and analyzed using SPSS version 25. The association between variables was analyzed using bivariate and multivariable logistic regression models, and a p-value <0.05 at 95% confidence interval was considered statistically significant.
Results:
A total of 400 participants were included with a response rate of 99.3%. The prevalence of HPV vaccine hesitancy among parents of daughters was 54%. Multivariable logistic regression showed that educational status (Adjusted Odds Ratio (AOR) = 0.8, 95% CI: (0.69–0.93)), effectiveness of HPV vaccine (AOR = 1.9, 95% CI: (1.14–3.17)), knowledge (AOR = 0.5, 95% CI: (0.13–0.75)), and obtained information (AOR = 3.1, 95% CI: (2.24–4.29)) were significantly associated with human papillomavirus vaccine hesitancy.
Conclusion:
This study demonstrates that parents’ hesitance to vaccinate their daughters with the human papillomavirus vaccine was high. Parents’ hesitance to vaccinate their daughters with the human papillomavirus vaccine was strongly associated with the effectiveness of the HPV vaccine, obtained information about the HPV vaccine, knowledge, and educational status.
Plain language summary
This study demonstrates that parents’ hesitance to vaccinate their daughters with the Human Papillomavirus (HPV) vaccine was high. Parents’ hesitance to vaccinate their daughters with the HPV vaccine was strongly associated with the effectiveness of the HPV vaccine, obtained information about the HPV vaccine, knowledge, and educational status.
Introduction
Human papillomavirus (HPV) is a widespread sexually transmitted infection, with certain strains causing cervical cancer, one of the leading causes of cancer-related deaths among women globally. According to the World Health Organization (WHO), cervical cancer is the fourth most common cancer in women worldwide, with approximately 570,000 new cases annually. In Ethiopia, the burden of cervical cancer remains high, contributing to a significant number of cancer-related deaths among women. The prevalence of HPV infection in Ethiopia is also a major public health concern, with studies indicating that HPV is the leading cause of cervical cancer in the country. Specifically, HPV is a vital factor in the development of cervical cancer, with types 16 and 18 being responsible for the majority of cases. 1
Each year, over 311,000 women succumb to cervical cancer, with 91% of fatalities concentrated in low- and middle-income regions. Without intervention, projected deaths annually could rise to 460,000 by 2040 due to demographic shifts and insufficient action. Sub-Saharan Africa, Central and South America, East Africa, South and Southeast Asia, and the Western Pacific bear the heaviest burden of the disease. 2
Prophylactic HPV vaccination, along with screening and treating precancerous lesions, represents a highly cost-effective strategy in preventing cervical cancer. Early detection and prompt treatment can lead to the successful cure of cervical cancer. Globally, efforts are underway to expedite the elimination of cervical cancer by 2030, with agreed-upon targets guiding this collective endeavor. 3
To combat vaccine hesitancy effectively, a comprehensive approach is essential, involving global awareness, targeted strategies, and evidence-based actions. The WHO underscores the importance of grasping the issue’s breadth, addressing root causes, and deploying context-specific interventions. This approach involves ongoing monitoring, evaluation, and acknowledgment of various determinants, spanning contextual, individual, and group factors, including concerns specific to vaccine. 4
The evidence supporting immunization’s benefits is substantial, marking it as a highly successful and cost-effective health intervention globally. Vaccines have played a pivotal role in saving lives and enhancing well-being worldwide. However, achieving high uptake rates is crucial to prevent the morbidity and mortality linked with vaccine-preventable diseases and to optimize disease control within communities. SAGE, in 2011, acknowledged the increasing recognition of hesitancy’s adverse effects on vaccine uptake rates and program effectiveness. 5
Cervical cancer is the most common cancer in women globally, with approximately 604,127 new cases and 341,831 deaths reported in 2020. 6
The highest rates of cervical cancer incidence and mortality occur in low- and middle-income countries, revealing significant inequities stemming from limited access to national HPV vaccination, cervical screening, and treatment services, alongside social and economic determinants. 3
Vaccine hesitancy, varying in prevalence across WHO regions, notably impacted the African region and lower income countries in 2016. Recognizing the impact of misinformation on disease transmission is pivotal for public health, particularly as recent studies suggest its role in exacerbating vaccine hesitancy and hindering vaccine uptake. 7
As vaccine hesitancy trends endure and associated risks potentially escalate, this supplement offers a timely addition to the existing knowledge on “vaccine hesitancy,” arriving midway through the Decade of Vaccines. 8
WHO advocates integrating HPV vaccines into a comprehensive strategy to prevent cervical cancer. Three licensed vaccines target types 16 and 18, administered before initial sexual activity in two- or three-dose schedules. Girls aged 9–14 are WHO’s primary target group for vaccination, enhancing cervical cancer prevention efforts. 1
Ethiopia, with 36.9 million women aged 15 and above, grapples with substantial cervical cancer risk, witnessing 7445 new cases and 5338 deaths yearly. While precise HPV data is lacking, Eastern Africa, including Ethiopia, shows a 4.7% prevalence of cervical HPV16/18 infection, with these HPV types contributing to 67.9% of invasive cervical cancers. 6
Vaccine hesitancy is multifaceted and varies based on time, location, and specific vaccines, influenced by factors like complacency, convenience, and confidence. 4 In 2018 and 2019, 17.6% of parents expressed hesitancy toward adolescent vaccines, often due to concerns about simultaneous administration or fears of serious, long-term side effects, source of information, educational status, economic status, attitude, and knowledge, and these factors influenced parents’ hesitance toward HPV vaccine. 9
In Ethiopia, a study revealed that 75.5% of 966 unvaccinated individuals hesitated to receive the vaccine, while 37.5% of vaccinated individuals expressed regret postvaccination. Vaccine hesitancy rates varied regionally, with the Afar region reporting the highest frequency at 78.5%, and the Sidama region the lowest at 47.82%. 10
Even though WHO advocates integrating HPV vaccines into a comprehensive strategy to prevent cervical cancer, vaccine hesitancy in Ethiopia often goes unnoticed despite its existence. 1 A study done in Jimma among female school students, the prevalence of HPV vaccine hesitance was 39.02%. 11 Efforts to prevent cervical cancer in Ethiopia have focused on early detection through screening programs and the introduction of the HPV vaccine. While cervical cancer screening programs have been implemented in some areas, their coverage is limited, and the effectiveness of such programs has been hindered by factors such as low awareness and limited access to healthcare. On the other hand, the introduction of the HPV vaccine offers significant potential for preventing HPV-related cervical cancer. Although the vaccine has been approved for use in Ethiopia, challenges related to vaccine acceptance and access persist. In Ethiopia, there is a lack of studies on parents’ hesitancy toward vaccinating their daughters with the human papillomavirus (HPV) vaccine. Many studies in Ethiopia have overlooked parents’ perspectives, focusing instead on school-based research.
This study aims to explore parental hesitance toward HPV vaccination in Dangila, Amhara Region and to identify the factors contributing to this hesitance. Understanding these factors is crucial for improving vaccine uptake and reducing the incidence of HPV-related cervical cancer in Ethiopia.
Methods and materials
Study design and period
A community-based cross-sectional study design was conducted from March 1, 2022 to April 30, 2023.
Study setting
This study was conducted in Dangila City Administration, Awi Zone, Amhara Region, Northwest Ethiopia. It is located 78 km away from Bahir Dar, the capital city of the Amhara Regional State, on the main road from Bahir Dar to Addis Ababa. Its altitude varies from 1800 to 2500 meters above sea level, with a latitude of 11.420061 and a longitude of 37.16. Based on the 2023 population projection, the total population is 15,504, with 6712 males and 8792 females. Dangila City Administration comprises five kebeles. Additionally, there is one governmental health center and one governmental primary hospital.
Source population
All parents of adolescent girls (9–14) in the Dangila City Administration.
Study population
All parents of adolescent girls selected (9–14 years) during the study period in the Dangila City Administration
Inclusion criteria
Parents of adolescent girls (from 9–14 years) in Dangila City Administration were included in the study.
Exclusion criteria
Parents of adolescent girls (from 9 to 14 years) who were critically ill (unconscious and in need of emergency treatment) were excluded from the study.
Study sample
The study was conducted among parents residing in Dangila City Administration, Amhara Region, Northwest Ethiopia. The target population included parents of girls aged 9–14 years, as this age group is recommended for HPV vaccination. A total of 403 parents were selected using a simple sampling technique.
Eligible participants were parents who had at least one daughter within the target age range and were willing to participate in the study. Parents who were unable to communicate due to illness or other impairments were excluded.
Sample size justification
The sample size was calculated using a single-population proportion formula with 95% confidence intervals (CIs), a 5% margin of error, and a 39.02% proportion of hesitancy in human papillomavirus (HPV) vaccine uptake among school girls in Jimma Town, Ethiopia. 11 With the incorporation of a 10% nonresponse rate, the total sample size is 403.


By adding 10% for the nonresponse rate, the total sample size was adjusted to 403.
The study encompassed all five kebeles within Dangila City Administration. A total of 4887 households and 2142 parents of adolescent girls resided in the town. The household served as the basic sampling unit in each kebele, with samples allocated proportionally based on the total number of households in each kebele. The count of households with parents of adolescent girls in each kebele was obtained from the kebele registration book. Household selection from each kebele was conducted using a simple random sampling technique. One parent of an adolescent girl per household was interviewed. Study participants were chosen using a simple random sampling technique, with samples proportionally allocated to each household based on the total number of households in Dangila City Administration (4887 households). In kebele one (988 households), kebele two (875 households), kebele three (762 households), kebele four (992 households), and kebele five (1270 households), the allocated samples for each kebele’s households were as follows: kebele one (81), kebele two (72), kebele three (63), kebele four (82), and kebele five (105). A simple random sampling technique was utilized to select 403 parents of adolescent girls for the study.
Study variables
Dependent variable
Human papillomavirus hesitance
Independent variables
✓ Sociodemographic characteristics
✓ Perception of HPV vaccine hesitance and effectiveness of the vaccine
✓ Knowledge
✓ Attitude
✓ Sociocultural characteristics
Operational definition of variables
Vaccine hesitation: Considered if there is a delay in the acceptance or refusal of vaccines despite the availability of vaccination services 5 and addressed by Do you intend to vaccinate your daughter with the HPV vaccine when it becomes available?” by answering Yes or No.
HPV vaccine: A vaccine that prevents infection by certain types of human papillomavirus.
Knowledge: Respondents who answer ⩾ 50% of the questions correctly will be categorized as having good knowledge of HPV, while those who answer < 50% of the questions correctly will be categorized as having low knowledge about HPV. 12
Attitude: Respondents’ attitudes toward HPV infection and vaccines were categorized as follows: negative if they obtained less than 50%, and positive if they obtained more than 50% of the total attitude score. 12
Data collection tools and procedure measurements
A standard questionnaire was used during interviews as a part of an organized quantitative data-gathering technique.11,13,14 The questionnaire included sections on sociodemographic characteristics, attitude, knowledge, perception of HPV vaccine hesitancy, and sociocultural characteristics. To ensure consistency, the questionnaire was initially written in English, then translated into Amharic, and back-translated into English by language specialists. Data collection was conducted by five midwives with diplomas, while supervision was provided by five midwives with bachelor’s degrees when distributing the structured questionnaire.
Data quality control
Pretesting of the questionnaire was conducted at the Chara kebele, which was not included in the study, using 5% of the sample population. This was done to ensure that the questions were uniform in terms of their organization, coherence, thoroughness, and ease of understanding. Following the pretest, the questionnaire was updated appropriately.
Before beginning the actual data-gathering process, data collectors received training on sampling and data collection techniques. Every day, supervisors and investigators checked and reviewed the completed questionnaires to make sure the data were accurate and consistent
Data processing and analysis
After being coded, cleaned, and imported into EPI-Data version 3.1, the data were exported to SPSS version 25 for further examination. Descriptive analysis, including frequency tables and bar graphs, was used to summarize the data.
To observe the relationship between each explanatory variable and the dependent variable, bivariable analysis was performed. Confounding variables were limited to those significantly correlated with the outcome variable in bivariate regression.
Multivariable logistic regression analysis was then conducted. Variables with a (p < 20%) relationship with the dependent variable, as determined by bivariate analysis, were added to the multivariate logistic regression analysis to identify correlations with the outcome variable.
The adjusted odds ratio and a p-value of <0.05, with a 95% confidence interval, were used to indicate a statistically significant relationship between the independent predictors and the outcome variable. The final model was checked using the Hosmer–Lemeshow Goodness of Fit test
Results
Sociodemographic characteristics of the respondents
A total of 400 parents of adolescents participated in this study, yielding a response rate of 99.3%. One hundred and sixty-nine participants (42.2%) belonged to the age group of 20–29, with a mean age of 29.29 and a standard deviation of ±4.44 years. Out of the total respondents, 298 (74.5%) were married, and 278 (69.5%) were educated (Table 1).
Sociodemographic characteristics of the respondents in Dangila City Administration, Amhara Region, Northwest Ethiopia, March 1–April 30, 2023 (N = 400).

Attitude of the respondents on HPV vaccine hesitance
Out of the total respondents, 278 (69.5%) had a positive attitude, while 122 (30.5%) had a negative attitude (Figure 1).

Attitude of the respondents on HPV vaccine hesitancy and in Dangila City Administration, Amhara Region, Northeast Ethiopia, March 1–April 30, 2023 (N = 400).
Perception of the respondents on HPV vaccine hesitance
Out of the total respondents, 158 (39.5%) believed that their daughters were susceptible to HPV infection. In this study, 216 (54%) of the participants hesitated toward the HPV vaccine, while 184 (66%) did not hesitate toward the HPV vaccine (Figure 2).

Perception of the respondents on HPV vaccine hesitance in Dangila City Administration, Amhara Region, Northeast Ethiopia, March 1–April 30, 2023 (N = 400).
Knowledge of the respondents regarding to HPV vaccine hesitance
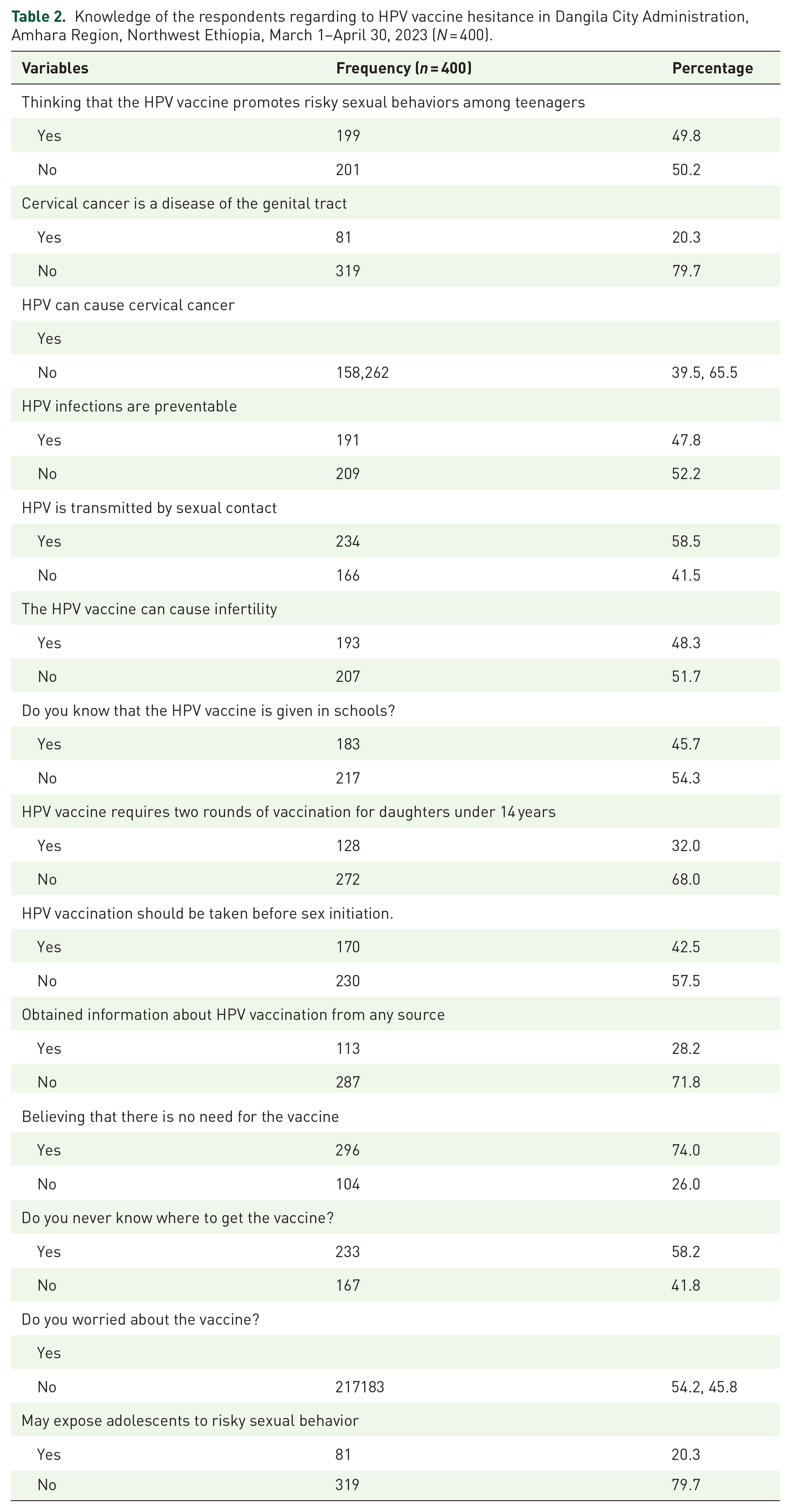
The majority of the respondents (71.8%) did not obtain information about the HPV vaccination from any source. Regarding knowledge of the HPV vaccine, the majority of them, specifically 174 (43.5%), had poor knowledge (Table 2).
Knowledge of the respondents regarding to HPV vaccine hesitance in Dangila City Administration, Amhara Region, Northwest Ethiopia, March 1–April 30, 2023 (N = 400).
Sociocultural characteristics of the respondents
Out of the total respondents, 260 (65.0%) reported that their religion did not allow HPV vaccination. Additionally, the majority of respondents, specifically 235 (58.8%), agreed that the HPV vaccine was in the government’s interest (Table 3).
Sociocultural characteristics of the respondents in Dangila City Administration, Amhara Region, Northwest Ethiopia, March 1–April 30, 2023 (N = 400).

Factors associated with HPV vaccine hesitancy
In bivariate logistic regression analysis, significant relationships were found between the respondents’ educational status, religion’s allowance for vaccination, occupational status, attitude toward the HPV vaccine, perceived effectiveness of the HPV vaccine, knowledge of the HPV vaccine, obtained information about the HPV vaccine, and belief that the HPV vaccine is risky for sexual behavior, all of which were significantly associated with HPV vaccine hesitancy. However, in multivariable logistic regression analysis, only educational status, knowledge of the HPV vaccine, obtained information about the HPV vaccine, and perceived effectiveness of the HPV vaccine were shown to be significantly associated with HPV vaccine hesitancy.
In comparison to those who are uneducated, participants who are educated were 20% less likely to hesitate on the HPV vaccine (Adjusted Odds Ratio (AOR) = 0.8, 95% CI: 0.69–0.93).
Individuals with good knowledge of the HPV vaccine were 50% less likely to hesitate on the HPV vaccine than those with poor knowledge (Adjusted Odds Ratio (AOR) = 0.5, 95% CI: 0.13–0.75).
Participants who did not believe in the effectiveness of the HPV vaccine were 1.9 times more likely to hesitate on the HPV vaccine compared to those who believed in its effectiveness (Adjusted Odds Ratio (AOR) = 1.9, 95% CI: 1.14–3.17).
Participants in this study who did not obtain information were shown to be 3.1 times more likely than those who did obtain information to hesitate on the HPV vaccine (Adjusted Odds Ratio (AOR) = 3.1, 95% CI: 2.24–4.29; Table 4).
Bivariate and multivariate logistic regression analyses for factors associated with HPV vaccine hesitancy among the parents of adolescents in Dangila City Administration, Amhara Region, Northwest Ethiopia, March 1–April 30, 2023 (N = 400).

Discussion
This study examined parental hesitancy toward HPV vaccination and its associated factors among parents in Dangila City Administration, Northwest Ethiopia. The key findings are as follows: Prevalence of Parental Hesitancy: A significant proportion (54%) of parents exhibited hesitancy toward vaccinating their daughters against HPV (95% CI: 48%–61%), highlighting the need for targeted interventions to improve vaccine acceptance.
This finding is consistence with a study conducted in Sidama, 10 which reported that 47.82% of respondents were hesitant toward the HPV vaccine. This similarity in sociodemographic characteristics, such as marital and educational status, between studies might contribute to the observed trends. For example, in the Sidama study, a majority of participants were married (44.5%) and educated (74.4%)), 10 aligning closely with the findings of this current study.
However, parents’ HPV vaccine hesitance in this finding was higher than studies conducted in America (17.6%) 14 and Logs Angeles (19.3%) 15 and Jimma (39.02%). 11 Variations in findings may stem from differences in study design, educational status, study population, and data collection methods. Previous studies, often school based, involved educated participants, whereas the current study focused on parents of daughters aged 9–14 years in a community-based cross-sectional design. For instance, the study from Los Angeles, USA, exclusively included educated participants, while data collection via phone in the U.S. study might yield lower response rates compared to face-to-face interviews, as in the current study’s approach. Additionally, the study in Jimma employed an institutional cross-sectional design with a qualitative component, contrasting with the broader community-based approach of the current study. which also found that higher awareness and understanding of the HPV vaccine were associated with lower hesitancy rates. The consistency across different settings suggests that educational interventions play a crucial role in improving vaccine acceptance globally.
The study’s findings indicated that individuals with good knowledge of the HPV vaccine were 50% less likely to exhibit hesitancy compared to those with poor knowledge. This result aligns with research conducted in the United States 16 and Italy 17 which also found that higher awareness and understanding of the HPV vaccine were associated with lower hesitancy rates. The consistency across different settings suggests that educational interventions play a crucial role in improving vaccine acceptance globally.
Participants in this study who did not obtain information about the HPV vaccine were 3.1 times more likely to exhibit hesitancy compared to those who had received information. This finding is supported by a study conducted in the South Gondar Zone, which also reported a strong association between the lack of information and increased HPV vaccine hesitancy. These results highlight the critical role of accessible and accurate health information in improving vaccine acceptance. 18 This may occur when parents receive misinformation or biased information about the HPV vaccine from unreliable sources, leading to increased hesitancy and concerns about its safety and efficacy.
Participants who did not believe in the effectiveness of the HPV vaccine were 1.9 times more likely to exhibit hesitancy compared to those who trusted its effectiveness. This study is supported by studies conducted in the United States 16 and Kenya. 19 This may be due to participants questioning the vaccine’s ability to prevent HPV infection and related cancers, leading to doubts about its overall benefits. Additionally, skepticism about the vaccine’s effectiveness could stem from misinformation or a lack of understanding about how vaccines work. Participants who were educated were 20% less likely to exhibit hesitancy toward the HPV vaccine compared to those who were not educated. This finding aligns with research from the United States, which also reported that higher education levels were associated with greater acceptance of the HPV vaccine, likely due to increased awareness and understanding of its benefits. 9 Suggesting that individuals with higher levels of education may have better access to reliable information and a greater understanding of the benefits and safety of vaccines. As a result, they are less likely to exhibit vaccine hesitancy.
Limitation of the study
This study was conducted in a single urban setting, which may not fully capture variations in HPV vaccine hesitancy across Ethiopia, particularly in rural or more socioeconomically diverse areas. Future studies should consider multisite investigations to enhance the generalizability of the findings
Owing to logistical and time restrictions, this study solely employed a quantitative methodology, which made it unable to thoroughly answer “why” questions.
Social desirability bias might be present in the study, but efforts were made to mitigate it. Participants were informed about the study’s purpose, confidentiality measures, and the importance of their honest participation, which could impact the study’s outcomes.
Conclusion and recommendation
This study highlights a high level of parental hesitancy toward vaccinating their daughters with the HPV vaccine. The findings indicate that perceived vaccine effectiveness, access to information, knowledge about the vaccine, and educational status are key factors influencing hesitancy.
To reduce vaccine hesitancy, targeted interventions should focus on improving health education, enhancing access to reliable vaccine information, and addressing misconceptions about the HPV vaccination. Strengthening public awareness campaigns and integrating vaccine education into healthcare services can help increase acceptance and uptake of the HPV vaccine, ultimately contributing to the prevention of HPV-related cancers.
☐ Community Health Worker Programs: Training local health workers to provide accurate vaccine information and dispel common misconceptions, particularly in areas with low HPV awareness.
☐ School-based Education Campaigns: Implementing HPV awareness sessions in schools and community centers, targeting parents and adolescents with culturally relevant, science-based information.
☐ Media and Social Media Engagement: Collaborating with trusted healthcare professionals and community leaders to promote pro-vaccine messages through radio, television, and social media platforms.
☐ Health System Strengthening: Ensuring consistent vaccine availability and reducing logistical barriers to increase access and confidence in the HPV vaccination program.
Supplemental Material
sj-docx-1-tav-10.1177_25151355251337622 – Supplemental material for Parents’ hesitance to vaccinate their daughters with the human papillomavirus vaccine and its associated factors in Northwest Ethiopia
Supplemental material, sj-docx-1-tav-10.1177_25151355251337622 for Parents’ hesitance to vaccinate their daughters with the human papillomavirus vaccine and its associated factors in Northwest Ethiopia by Tegegne Wale Belachew, Begizew Yimenu Mekuriaw, Wassie Yazie Ferede, Dagnaw Mersha Tegegne, Temesgen Dessie Mengistu, Selamawit Girma Tadesse, Yaregal Dessalew Tariku, Fillorenes Ayalew Sisay and Assefa Kebie Mitiku in Therapeutic Advances in Vaccines and Immunotherapy
Footnotes
Acknowledgements
The authors would like to thank Debre Tabor University College of Health Sciences for their support and valuable contributions to this study.
Declarations
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.