
Abstract
Background:
Respiratory syncytial virus (RSV) poses a significant respiratory health risk to senior citizens, contributing substantially to hospitalizations and mortality. With the recent approval of three RSV vaccines for the elderly, it is critical to understand the factors that can shape the RSV vaccination attitudes to inform public health strategies that can enhance uptake among this vulnerable population.
Objectives:
This study aimed to investigate the potential factors that could influence the attitudes toward RSV vaccination among senior citizens in Arab countries.
Design:
A multinational cross-sectional study, adhering to STROBE guidelines, was conducted using a survey instrument previously validated through exploratory factor analysis to assess attitudes toward the newly approved RSV vaccine.
Methods:
A self-administered online survey was distributed conveniently among senior citizens mainly across five Arab countries. The survey collected data on demographics, vaccination history, and key constructs related to RSV vaccine attitude, including “Fear,” “Information,” “Accessibility,” “Benefits,” and “Conspiracy.”
Results:
A total of 483 participants were included in the study, with the majority from five Arab countries: Jordan (n = 239, 49.5%), Kuwait (n = 74, 15.3%), Egypt (n = 68, 14.1%), Saudi Arabia (n = 51, 10.6%), and the UAE (n = 23, 4.8%), alongside participants from other Arab nations (n = 28, 5.8%). Among the respondents, 51.1% (n = 247) expressed acceptance of the RSV vaccine, 22.4% (n = 108) were hesitant, and 26.5% (n = 128) exhibited refusal. Multivariate analysis identified perceived benefits (β = 0.484, p < 0.001), information needs (β = 0.229, p < 0.001), and previous vaccination history (β = 0.087, p = 0.016) as significant positive predictors of vaccine acceptance. Conversely, stronger conspiracy beliefs (β = −0.083, p = 0.035) were associated with vaccine resistance. Fear and accessibility were not significant predictors of vaccine attitudes.
Conclusion:
The findings showed that perceived benefits, access to reliable information, previous vaccination history, and conspiracy beliefs are essential to promote RSV vaccine acceptance among Arab seniors. These factors are recommended to improve RSV vaccine uptake in this vulnerable population.
Plain language summary
Respiratory syncytial virus (RSV) is an important health risk to older adults, and newly approved RSV vaccines could help prevent severe illness. This study looked at what influences seniors citizens views on the RSV vaccine in Arab countries. Among 483 participants, more than half were willing to get vaccinated, while others were either hesitant or resistant. The main reasons for RSV vaccine acceptance included trust in its benefits, a history of getting other vaccines, and a desire for more information. However, belief in conspiracy theories was linked to vaccine resistance. These findings suggest that highlighting the vaccine benefits and addressing misinformation could boost RSV vaccination rates among the elderly.
Introduction
Respiratory syncytial virus (RSV) is a leading cause of severe respiratory infections among vulnerable populations such as infants, immunocompromised individuals, and the elderly.1–4 While the global burden of RSV as a cause of lower respiratory tract infections (LRTIs) has long been recognized in pediatric populations, it has recently been identified as a significant cause of respiratory infections among the elderly.5–7
For example, a systematic review and meta-analysis in 2023 by Nguyen-Van-Tam et al. reported that 4.7% of symptomatic respiratory infections in elderly adults were related to RSV, with a case fatality rate (CFR) of 8.2%. 8 Another systematic review and meta-analysis by Shi et al. estimated that acute RSV infections resulted in about 336,000 hospitalizations and 14,000 deaths globally in 2015 among adults aged 65 and older. 9 In addition, a review by RESCEU (REspiratory Syncytial virus Consortium in EUrope) investigators demonstrated that adults with comorbidities experience a higher RSV burden, with an incidence rate of 37.6 per 1000 individuals annually and a hospital CFR of 11.7%. 10
On the other hand, the scarcity of RSV burden data from low- and middle-income countries (LMICs) highlights the need for increased RSV research and surveillance in these regions.1,6 A recent review by Günen et al. highlighted the significant challenges in understanding the burden of RSV among older adults in LMICs, particularly in Southeast Asia (SEA) and the Middle East and North Africa (MENA) region. 11 Limited awareness among healthcare workers (HCWs), policymakers, and the public, coupled with underdiagnosis and inadequate surveillance systems, obscures the real-world impact of RSV disease especially among the elderly in LMICs.11–14
The increased recognition of RSV disease impact on aging populations necessitates effective prevention strategies such as vaccination. 15 The recent approval of effective and safe RSV vaccines for older adults represented a significant public health breakthrough to reduce the burden of RSV disease in this vulnerable population.16,17 In May 2023, the U.S. Food and Drug Administration (FDA) approved Arexvy by GlaxoSmithKline, the first vaccine for RSV prevention in adults aged 60 and older. 18 Arexvy showed 82.6% efficacy against RSV-related LRTIs, 94.1% against severe disease, and 71.7% against acute respiratory infection, with an acceptable safety profile.19–21
Soon after, Abrysvo by Pfizer was approved for RSV prevention in adults aged 60 and older, with an expert panel recommending its use in pregnant women to protect newborns through maternal immunization. 22 In a phase 2b trial in adults aged 65 and older, Abrysvo showed efficacy of 80.0%, 75.0%, and 69.8% against RSV LRTIs based on varying case definitions. 23 In 2024, the Mresvia RSV vaccine by Moderna—an mRNA-based RSV vaccine—was approved, 24 with 68.4% efficacy against acute respiratory disease. 25 In 2024, the FDA expanded Arexvy approval to adults aged 50–59 at increased RSV risk with the Centers for Disease Control and Prevention (CDC) recommendation of a single dose of any FDA-approved RSV vaccine for adults 75+ and those 60–74 at high risk.24,26
Despite these remarkable breakthroughs in RSV vaccination, its success is not merely dependent on vaccine availability. An expected challenge would be the phenomenon of vaccine hesitancy or outright vaccine refusal among older adults, who often have complex health needs and unique concerns about vaccines.27–33 As defined by Heidi J. Larson—a pioneering expert in vaccine hesitancy research—vaccine hesitancy/refusal reflects indecision regarding vaccination, influenced by factors such as safety, efficacy, and cost concerns. 34 On the other hand, the World Health Organization (WHO) Strategic Advisory Group of Experts (SAGE) Working Group defines vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite availability of vaccine services.”35–38 Among elderly individuals, vaccine hesitancy or refusal can be heightened by more intense fears of side effects, compounded by the prevalence of comorbidities and age-related immune decline.27,39–41
In the Arab world, life expectancy at birth rose from 70.18 years in 2012 to 71.23 years in 2022, leading to an increase in the elderly population and a heightened vulnerability to RSV-related disease. 42 Vaccine hesitancy/refusal, a phenomenon influenced by place-specific factors, 35 poses additional challenges in this context. Elderly individuals in the Arab world face distinct sociocultural, economic, and logistical challenges that shape their attitudes toward RSV vaccination. 43 This challenge is expected in light of the high prevalence of vaccine hesitancy observed during the coronavirus disease 2019 (COVID-19) pandemic across Arab countries.44–46 Thus, it is important to understand the factors that would drive the attitude to the newly approved RSV vaccines to effectively address RSV vaccine hesitancy/refusal among the senior citizens in Arab countries.
A recent exploratory study in Jordan among individuals aged 50 and older identified key factors that would shape RSV vaccine attitudes. 47 These factors included fear of side effects, the need for more information, perceived benefits, accessibility, and conspiracy beliefs. 47 Building on this novel survey instrument, the current study aimed to assess how these factors, along with demographics and vaccination history, would influence RSV vaccine acceptance among elderly individuals in Arab countries. By utilizing a validated survey tool tailored to older adults, this study aimed to elucidate the psychological, social, and practical barriers to RSV vaccine acceptance, which can help design targeted public health strategies to enhance RSV vaccine acceptance and improve health outcomes in this vulnerable population.11,48,49
Methods
Study design, setting, and ethics
This cross-sectional study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental File S1).50,51 A previously validated survey tool through exploratory factor analysis (EFA) was utilized, 47 distributed online mainly across five Arab nations: Jordan, Egypt, Saudi Arabia, Kuwait, and the United Arab Emirates (UAE). The survey was self-administered and disseminated through a non-random, convenience-based snowball sampling method. 52 Initiated by the authors, who collaborated from the five target countries, the survey link was shared via social media platforms (Facebook, WhatsApp, and Messenger). This approach was chosen to expedite the process of reaching a diverse group of senior citizens across the region. The survey link was open during August 1–September 30, 2024. The process began with the authors’ social contacts in the five target countries, who were then encouraged to distribute the survey further within their networks, to broaden the reach to additional eligible participants. Eligibility criteria as outlined in the introductory section of the survey required participants to be aged 50 years or older and residing in any Arab country. To ensure accessibility and comprehension for this demographic, the survey was administered in Arabic language.
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. 53 Participants were informed about the purpose and nature of the study, and their informed consent was obtained electronically before they could proceed with the survey. The collected data were then anonymized to ensure confidentiality, and participation was entirely voluntary without incentives and no personal identifiers were collected.
Sample size calculation
For this study, we assumed a conservative estimate of 50% prevalence for RSV vaccine acceptance to ensure the sample size was sufficient, given the lack of existing data on RSV vaccine attitudes in this population. 54 Using a 95% confidence level and a margin of error of ±5%, we calculated a minimum sample size of 385 participants of a large population to estimate RSV vaccine acceptance prevalence. 55
In addition, the study aimed to conduct a confirmatory factor analysis (CFA) to validate the constructs of Fear, Information, Accessibility, Benefit, and Conspiracy related to RSV vaccine attitude previously explored by Abu-Ghosh et al. 47 For CFA, a minimum sample size of 5–10 participants per survey item is recommended.56,57 With 15 items in the initial RSV vaccine attitude scale, this necessitated a sample size of 75 to 150 participants. To enhance the robustness of the CFA, we sought a larger sample size of close to 500 participants.
Survey tool
The survey tool used in this study was administered via Google Forms and comprised several sections as follows. Before beginning the survey, participants were presented with an informed consent form, followed by an electronic consent item “Do you agree to participate in this study?”, to ensure that they understood the purpose of the study and the voluntary nature of their participation.
The first part of the survey focused on demographic information, where participants were asked about their age (as a scale variable), sex (male vs female), marital status (married vs single vs divorced vs widow/widower), educational level (high school or less vs undergraduate vs postgraduate), self-reported financial status (low vs average vs high), occupation (retired/unemployed vs. employed as HCW vs employed as non-HCW), and country of residence. In addition, survey items were included to record the number of chronic diseases the participant had, their smoking history (non-smoker vs ex-smoker vs current smoker), the number of COVID-19 vaccine doses they had received (0–4 or more), whether they had received an influenza vaccine in the past, and their awareness of RSV before the study.
The second part of the survey comprised 15 items of the RSV vaccine attitudes scale organized into five key constructs each with three items: Fear, Information, Accessibility, Benefit, and Conspiracy. Responses were measured on a five-point Likert scale ranging from “strongly agree” to “strongly disagree.”
First, the “Fear” construct items were as follows: (1) “I am concerned that RSV vaccination may have negative effects on my health”; (2) “I have concerns about the long-term side effects of RSV vaccination”; and (3) “I am concerned about possible side effects of RSV vaccination.”
Second, the “Information” construct items were as follows: (1) “I would like to discuss the benefits of RSV vaccination with my healthcare provider”; (2) “I would like to receive educational materials about RSV vaccination for the elderly”; and (3) “I need more information about possible side effects of RSV vaccination.”
Third, the “Accessibility” construct items were as follows: (1) “I think vaccination is easily accessible for seniors in the country where I live”; (2) “I have enough information about where to get vaccinated in the country I live in”; and (3) “I am concerned about the potentially high cost of RSV vaccination”. The last item was excluded from the final analysis based on the results of CFA.
Fourth, the “Benefit” construct items were as follows: (1) “I trust the safety and effectiveness of vaccination for the elderly”; (2) “I think vaccination is necessary to protect myself from acute respiratory diseases”; and (3) “I believe vaccination is a responsible choice to keep me healthy.”
Finally, the “Conspiracy” construct items were as follows: (1) “I believe that the increased use of vaccines serves a hidden political agenda”; (2) “I believe that the increased use of vaccines aims at reducing the size of the world population”; and (3) “I believe that the increased use of vaccines serves a hidden economic agenda.”
The primary outcome measure of this study, participants’ acceptance of RSV vaccination, was assessed using a five-point Likert scale (strongly agree to strongly disagree). The exact wording of the item was as follows: “If RSV vaccination for the elderly is safe, effective, and freely available, I would be willing to get vaccinated.”
Statistical analysis
Data analyses were conducted using IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp and JASP (Version 0.19.0.0) software, with structural equation modeling (SEM) employed for model evaluation. 58 Univariate analyses, including chi-square and Kruskal–Wallis tests (K-W), were used to examine associations between demographic factors and attitudes toward RSV vaccination divided into three categories (acceptance vs hesitancy vs refusal groups). The Kolmogorov–Smirnov test confirmed the non-normality of the scale variables, justifying the use of non-parametric methods (p < 0.001 for all). Variables with a p value <0.100 in univariate analyses were included in the multivariate logistic regression to identify independent predictors of RSV vaccine acceptance while controlling for confounding factors. Analysis of variance (ANOVA) was used to validate the linear regression model, and multicollinearity diagnostics were conducted using the variance inflation factor (VIF) to ensure model robustness with VIF > 5 to flag potential multicollinearity issues. 59 A p value of <0.050 was considered statistically significant.
The Kaiser–Meyer–Olkin (KMO) test and Bartlett’s test of sphericity were used to confirm sampling adequacy and factorability of the data. CFA was performed to validate the measurement model and assess the factor structure of the Fear, Information, Accessibility, Benefit, and Conspiracy constructs. Model fit was evaluated using multiple indices, including the root mean square error of approximation (RMSEA), Tucker–Lewis index (TLI), comparative fit index (CFI), standardized root mean square residual (SRMR), and goodness-of-fit index (GFI) were calculated with thresholds of RMSEA < 0.06, TLI > 0.90, CFI > 0.90, and GFI > 0.90 indicating a good fit. 60 Internal consistency of the RSV vaccine attitude scale constructs was assessed using Cronbach’s α and McDonald’s ω with acceptable values considered for α and ω exceeding 0.700. 61 Each construct comprising three items, except for Accessibility (two items), was divided into three categories based on item responses: agreement (3–6), neutral (7–11), and disagreement (12–15), while for the “Accessibility” construct the stratification was as follows: agreement (2–4), neutral (5–7), and disagreement (8–10).
The RSV vaccine attitude was categorized into three distinct groups based on participants’ responses to the item: “If RSV vaccination for the elderly is safe, effective, and freely available, I would be willing to get vaccinated” with responses of “strongly agree” and “agree” classified as the “RSV vaccine acceptance” group, while “neutral” responses indicated “RSV vaccine hesitancy”, and those who selected “strongly disagree” or “disagree” were categorized as the “RSV vaccine refusal” group.
Finally, the “vaccine uptake score” was calculated by summing the number of COVID-19 vaccine doses received and the influenza vaccine uptake status, where influenza vaccine uptake was assigned a score of 1, and a lack of influenza vaccination was assigned a score of 0. This cumulative score was then dichotomized into two groups: low uptake (0–2) and high uptake (3–5), to provide a surrogate measure of participants’ history of vaccination behavior.
Results
Description of the final study sample
The final study sample comprised a total of 483 participants, a vast majority of whom were from five Arab countries: Jordan (n = 239, 49.5%), Kuwait (n = 74, 15.3%), Egypt (n = 68, 14.1%), Saudi Arabia (n = 51, 10.6%), the UAE (n = 23, 4.8%), and other Arab countries (n = 28, 5.8%).
The mean age of the participants was 55.89 ± 6.49 years with a median of 54 years (range: 50–81 years). The majority were married (75.8%), while 24.2% were single, divorced, or widowed. In terms of education, 27.1% had completed high school or less, 55.9% held an undergraduate degree, and 17.0% had a postgraduate degree. Most participants reported an average financial status (68.3%), with 20.5% reporting low financial status and 11.2% reporting high financial status. Occupational status varied, with 55.9% being retired or unemployed, 29.0% employed as non-HCWs, and 15.1% employed as HCWs. Regarding smoking history, 71.4% were non-smokers, 10.1% were ex-smokers, and 18.4% were current smokers. COVID-19 vaccine uptake was widespread, with 50.7% having received two doses, 26.3% three doses, and 1.9% four doses or more, while 14.3% had not received any COVID-19 vaccine doses. Influenza vaccine uptake was lower, with 41.4% reporting they had received it, while 58.6% either had not received influenza vaccines or were unsure. Furthermore, only 34.2% of participants had heard of RSV before the study, with 65.8% reporting no prior knowledge of the virus (Table 1).
General features of the study sample (N = 483).
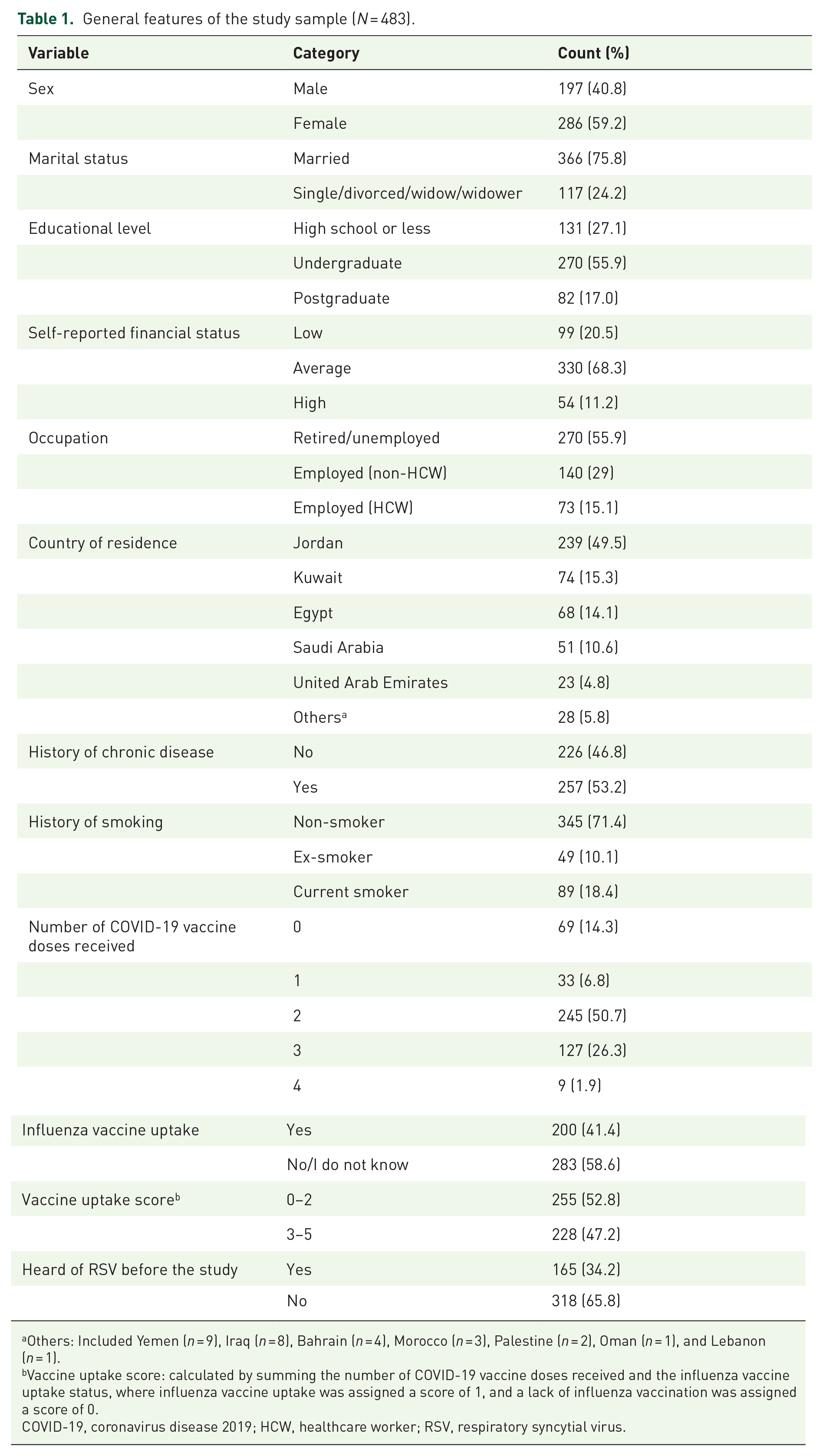
Others: Included Yemen (n = 9), Iraq (n = 8), Bahrain (n = 4), Morocco (n = 3), Palestine (n = 2), Oman (n = 1), and Lebanon (n = 1).
Vaccine uptake score: calculated by summing the number of COVID-19 vaccine doses received and the influenza vaccine uptake status, where influenza vaccine uptake was assigned a score of 1, and a lack of influenza vaccination was assigned a score of 0.
COVID-19, coronavirus disease 2019; HCW, healthcare worker; RSV, respiratory syncytial virus.
Overall attitude to RSV vaccination
Overall, attitudes toward RSV vaccination in the study population were as follows: 26.5% of participants showed refusal to RSV vaccination (n = 128), 22.4% exhibited hesitancy to RSV vaccination (n = 108), and 51.1% indicated acceptance of the vaccine (n = 247). Stratified per country, RSV vaccine refusal was most prominent in Kuwait (35.1%) and Jordan (31.8%), while hesitancy ranged from 16.2% in Egypt to 26.1% in the UAE. RSV vaccine acceptance was the highest in Saudi Arabia (70.6%) and the UAE (69.6%), followed by Egypt (57.4%). In Jordan and Kuwait, RSV vaccine acceptance was lower, at 46.0% and 41.9%, respectively (Figure 1).

The rates of RSV vaccine acceptance per country.
In univariate analysis, significant associations were observed between attitudes toward RSV vaccination and both country of residence and vaccine uptake score. Participants from Saudi Arabia (70.6%) and the UAE (69.6%) had the highest rates of RSV vaccine acceptance, while those from Kuwait (35.1%) and Jordan (31.8%) showed the highest refusal of the vaccine (p < 0.001). In addition, individuals with higher vaccine uptake scores (3–5) demonstrated significantly greater acceptance of the RSV vaccine (58.3%) compared to those with lower uptake scores (0–2), who had a higher rate of refusal (34.1%; p < 0.001). Although other variables, such as sex, educational level, and financial status, did not reach statistical significance, there were notable trends. Males tended to have higher RSV vaccine acceptance rates (54.3%) compared to females (49.0%, Table 2).
Univariate analysis for the factors associated with RSV vaccine attitude.
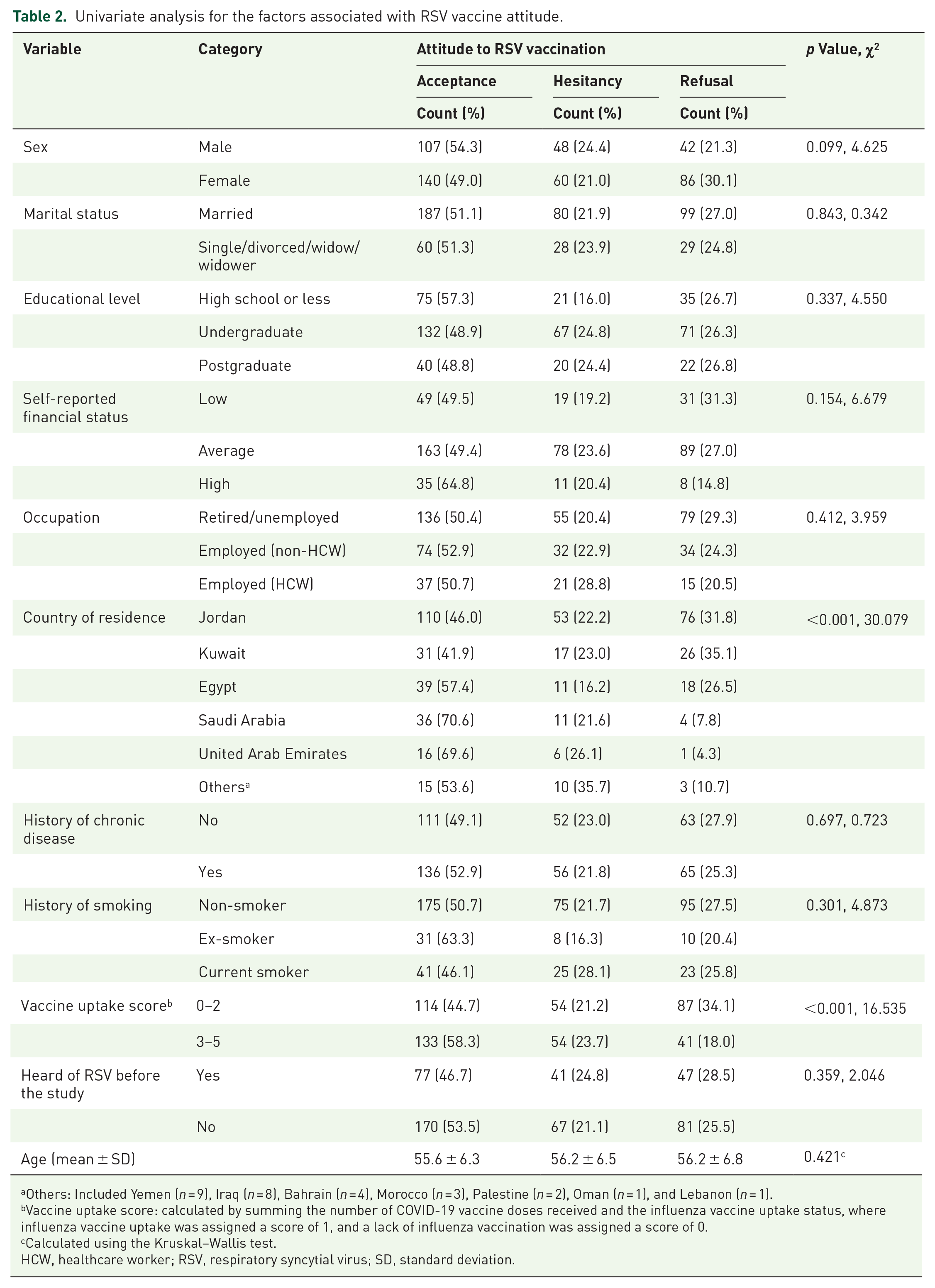
Others: Included Yemen (n = 9), Iraq (n = 8), Bahrain (n = 4), Morocco (n = 3), Palestine (n = 2), Oman (n = 1), and Lebanon (n = 1).
Vaccine uptake score: calculated by summing the number of COVID-19 vaccine doses received and the influenza vaccine uptake status, where influenza vaccine uptake was assigned a score of 1, and a lack of influenza vaccination was assigned a score of 0.
Calculated using the Kruskal–Wallis test.
HCW, healthcare worker; RSV, respiratory syncytial virus; SD, standard deviation.
Confirmatory factor analysis of the RSV attitude scale
The KMO test showed an overall measure of sampling adequacy of 0.785, with individual Measure of Sampling Adequacy (MSA) values ranging from 0.688 to 0.875, while Bartlett’s test of sphericity was significant (χ2 = 4366.138, df = 91, p < 0.001), indicating that the underlying data were suitable for factor analysis.
In SEM, the CFA demonstrated a significantly better fit for the factor model (χ2 = 199.274, df = 67, p < 0.001) compared to the baseline model (χ2 = 4425.697, df = 91), supporting the validity of the proposed constructs for assessing RSV vaccination attitude. The CFA analysis also demonstrated a strong fit, as indicated by a CFI of 0.969 and a TLI of 0.959, suggesting the model’s suitability to capture the underlying factor structure. Additional fit measures indicated a good model fit, with RMSEA = 0.064 (p = 0.013), SRMR = 0.038, GFI = 0.992, and Hoelter’s Critical N exceeding 212, suggesting that the model provided an acceptable representation of the data and would generalize well to other samples.
The reliability analysis showed strong internal consistency across all constructs, with McDonald’s ω values of 0.922 for the “Fear” construct, 0.865 for the “Information” construct, 0.751 for the “Accessibility” construct after excluding the third item, 0.886 for the “Benefit” construct, and 0.916 for the “Conspiracy” construct, while Cronbach’s α values were 0.917, 0.861, 0.742, 0.875, and 0.916, respectively.
The factor loadings ranged from 0.72 to 1.03 across the constructs, with particularly high loadings for the “Fear” (0.84–0.97), “Benefit” (0.81–1.03), and “Conspiracy” (0.99–1.04) constructs (Figure 2).

Confirmatory factor analysis for the RSV vaccine attitude scale among the elderly. The SEM shows the relationships between five latent constructs: Fear (Fer), Information (Inf), Accessibility (Acc), Benefit (Bnf), and Conspiracy (Cns) and their respective observed variables. Factor loadings are indicated on the paths, with higher values representing stronger associations.
Association between attitude to RSV vaccination and the RSV attitude scale constructs
The univariate analysis demonstrated significant associations between attitude to RSV vaccination and the constructs: Fear, Information, Accessibility, Benefit, and Conspiracy (p < 0.001 for all constructs, Table 3).
Association between RSV vaccine attitude scale constructs and willingness to receive the RSV vaccine.

RSV, respiratory syncytial virus.
As scale variables, the five RSV vaccine attitude scale constructs showed statistically significant differences stratified per the three RSV attitude categories as follows. For the Fear construct, the mean score was 11.2 ± 2.9 in the acceptance group, 11.3 ± 2.3 in the hesitancy group, while it was 12.3 ± 3.1 in the refusal group indicating the higher agreement with Fear in the refusal group (p < 0.001). For the Conspiracy construct, the mean score was 10.2 ± 3.3 in the acceptance group, 9.8 ± 2.7 in the hesitancy group, while it was 11.5 ± 3.3 in the refusal group indicating the higher agreement with Conspiracy in the refusal group (p < 0.001). For the Information construct, the mean score was 12.8 ± 2.1 in the acceptance group, 11.7 ± 2.3 in the hesitancy group, while it was 10.6 ± 3.2 in the refusal group indicating the higher agreement with Information in the acceptance group (p < 0.001). For the Benefit construct, the mean score was 11.9 ± 2.3 in the acceptance group, 9.3 ± 1.7 in the hesitancy group, while it was 7.4 ± 2.8 in the refusal group indicating the higher agreement with Benefit in the acceptance group (p < 0.001). Finally, for the Accessibility construct, the mean score was 7.2 ± 1.9 in the acceptance group, 6.5 ± 1.5 in the hesitancy group, while it was 6.1 ± 2.2 in the refusal group indicating the higher agreement with Benefit in the acceptance group (p < 0.001, Figure 3).

Error bars depicting the mean score for RSV vaccine attitude scale constructs.
Factors associated with RSV vaccine attitude using multivariate linear regression analysis
The ANOVA confirmed that the overall regression model was highly significant (F = 48.514, p < 0.001). The multivariate linear regression model explained 41.7% of the variance in attitudes (R 2 = 0.417, p < 0.001), with several predictors significantly influencing RSV vaccination attitudes as follows. The Benefit construct emerged as the strongest positive predictor (β = 0.484, p < 0.001), which indicated that participants who perceived greater benefits of the RSV vaccine were more likely to accept RSV vaccination. Similarly, the Information construct (β = 0.229, p < 0.001) and the vaccine uptake score (β = 0.087, p = 0.016) were significant positive predictors, suggesting that greater aspiration for information on the RSV vaccine and previous vaccination experience positively influenced the acceptance of the RSV vaccine. Conversely, the Conspiracy construct was a significant negative predictor (β = −0.083, p = 0.035), suggesting that individuals with stronger conspiracy beliefs were more likely to refuse RSV vaccination. Other factors, such as Sex (β = −0.048, p = 0.180), Fear construct (β = −0.061, p = 0.121), and Accessibility construct (β = 0.028, p = 0.475), did not show statistically significant associations with attitudes toward the RSV vaccine (Table 4).
Multivariate analysis using linear regression analysis for the factors associated with RSV vaccine acceptance among the participants in Arab countries.

Vaccine uptake score: calculated by summing the number of COVID-19 vaccine doses received and the influenza vaccine uptake status, where influenza vaccine uptake was assigned a score of 1, and a lack of influenza vaccination was assigned a score of 0.
Statistically significant p values are highlighted in bold style.
VIF, variance inflation factor.
Discussion
The current study represents one of the first comprehensive initial assessments of RSV vaccine acceptance among senior citizens following the recent approval of three RSV vaccines. The study also aimed to enhance rigor through the multi-national scope to assess a wide range of attitudes and sociocultural factors that could influence RSV vaccine uptake among a demographic vulnerable to RSV risks. The current study validated the key constructs previously explored in a single country and ensured the reliability of a novel survey tool specifically designed to provide insights into the factors that could shape the RSV vaccine attitude among the elderly. Given the high susceptibility of elderly individuals to severe respiratory complications from RSV, the study findings can be critical to guide public health interventions aimed at improving RSV vaccine uptake.
In our study, 51% of the participants expressed acceptance toward RSV vaccination, 22% were hesitant, and 27% showed refusal to RSV vaccination. While comparative data remain limited due to the RSV vaccines’ recent approval, studies on maternal attitudes can offer useful comparative insights. In Nepal, 72% of mothers were willing to receive the RSV vaccine during pregnancy, according to Adhikari et al. 62 In Ireland, McCormack et al. found that 49% of pregnant women accepted RSV vaccination despite limited prior awareness of RSV. 63 In Jordan, 78% expressed RSV vaccine acceptance if the vaccine was free, safe, and effective. 64 Collectively, these findings highlight the variability in RSV vaccine acceptance both across different populations and within varying contextual settings.
A key finding of this study was the strong positive correlation between perceived benefits and favorable attitudes toward RSV vaccination, as reflected in the “Benefit” construct. This result points to the critical role that perceptions of vaccine efficacy and safety play in shaping RSV vaccine acceptance among older adults. According to established health behavior models, including the Health Belief Model (HBM), individuals are more likely to engage in preventive health actions (e.g., vaccination) when they perceive benefits in disease prevention and health protection.65–68 In the context of RSV disease, where older adults face heightened risks of severe respiratory illness with hospitalizations and mortality, recognizing the protective value of RSV vaccines can become a useful motivator for its acceptance as demonstrated in this study. Thus, public health messaging that emphasizes the discernible benefits of vaccination such as reducing the risk of severe illness, hospitalization, or death could significantly increase RSV vaccine uptake in this vulnerable population.
The finding of perceived benefits as a major driving factor for RSV vaccine acceptance among senior citizens aligns with existing literature on vaccine acceptance across various vaccine types, where trust in the protective effects of the vaccine consistently emerges as a critical determinant of willingness to vaccinate, especially among older populations.69,70 Similar trends have been observed in studies on influenza and COVID-19 vaccines. For example, in the context of COVID-19 vaccination, Ibrahim et al. found that among older adults in Mansoura, Egypt, high perceptions of COVID-19 vaccine benefits were associated with increased acceptance. 71 Comparable results were also noted outside the Arab world, including a qualitative study in New South Wales, Australia, where older adults reported that their motivation to receive the COVID-19 vaccine was strongly influenced by its perceived benefits. 72 In addition, in China, older adults with a heightened perception of vaccine benefits were more likely to accept the booster dose of COVID-19 vaccination. 73
In the context of influenza vaccination, previous studies support the central role of perceived benefits in driving vaccine acceptance and uptake. 74 For example, an early study by Madhavan et al. reported that in rural West Virginia, the U.S., the belief in the benefits of influenza vaccination significantly predicted vaccine acceptance among senior adults. 75 Similarly, Lau et al. reported that among elderly populations in Hong Kong, perceived efficacy in preventing illness was a strong predictor of influenza vaccine uptake. 76 Collectively, these findings together with our findings reinforce the idea that emphasizing the benefits of vaccination can be a critical strategy for increasing RSV vaccine acceptance among older adults.
In this study, the significance of the “Information” construct as a driver of positive attitudes toward RSV vaccination was clear. Participants who were considered keen to seek more information about RSV vaccination, particularly from HCWs, were more inclined to view the RSV vaccination favorably. This highlights the essential role of reliable and accessible information in shaping RSV vaccine acceptance, especially in the face of widespread misinformation. This has been shown in the context of young females’ attitudes to maternal RSV immunization in Jordan. 77
The role of media and information sources in shaping vaccine attitudes has been extensively studied, with Recio-Román et al. recently demonstrating that vaccine hesitancy fully mediates the relationship between media exposure and vaccine uptake. 78 Recio-Román et al. showed that to effectively boost vaccine uptake, it is essential to address the root causes of vaccine hesitancy directly via clear, evidence-based information about vaccines, correcting widespread misconceptions, and enforcing trust in healthcare systems and providers. 78 The results of our study further support this conclusion, highlighting the central role of accurate, accessible information in shaping positive attitudes toward RSV vaccination. The HCWs group can play a central role as trusted sources of RSV vaccine information, as individuals who receive guidance from HCWs were shown to be significantly more likely to get vaccinated. 79 Thus, public health initiatives should prioritize providing HCWs with clear, evidence-based communication strategies to effectively address concerns surrounding RSV vaccination. 80
A history of previous vaccine uptake also emerged as a significant predictor of positive attitudes toward RSV vaccination among senior citizens in this study. Specifically, older individuals who had previously received vaccines, such as influenza or COVID-19 vaccines, were more likely to accept the RSV vaccine. This finding is consistent with previous studies which demonstrated that past vaccination behavior is a strong indicator of future vaccine acceptance. For example, Mahameed et al. found that HCWs in Jordan who had a higher history of vaccine uptake were four times more likely to intend to receive the monkeypox vaccine. 81 This suggests that reinforcing vaccination as a routine health behavior can further enhance trust in vaccines and improve uptake in this vulnerable population.
Conversely, in this study, the “Conspiracy” construct was a significant negative predictor of RSV vaccine attitudes with individuals who held stronger conspiracy beliefs were less likely to accept the vaccine. This finding aligns with trends observed in broader vaccine hesitancy research, where the embrace of specific vaccine conspiracy theories was reported to undermine trust in vaccines with a subsequent refusal of vaccination efforts.82–85
The role of misinformation and conspiracy theories has been well documented in contributing to lower vaccine uptake.86–89 This issue is particularly relevant in Arab countries, where the endorsement of conspiracy beliefs has been reported at high levels especially during the COVID-19 pandemic.90,91 Studies in Jordan, Kuwait, and Iraq have shown that conspiracy beliefs negatively impact attitudes toward various vaccines, including those for COVID-19, human papillomavirus (HPV), and influenza.46,88,92,93
Alarmingly, even well-informed individuals, such as healthcare workers (HCWs) in Arab countries, are not immune to the influence of conspiracy beliefs. These beliefs extend beyond simple vaccine hesitancy, contributing to heightened perceptions of side effects following COVID-19 vaccination.94,95 In addition, the negative impact of conspiracy beliefs has been linked to an increased reporting of long COVID symptoms among adults in Arab countries. 96 This concerning trend shows the prevalent existence of these false notions, which can undermine vaccine confidence. Addressing this issue requires a concerted effort to provide clear, evidence-based information that dispels myths and reassures individuals about RSV vaccine safety and efficacy to counteract the detrimental impact of these unfounded beliefs.
Interestingly, in this study, the “Fear” and “Accessibility” constructs were not significant predictors of RSV vaccine attitudes among seniors. While fear is often a driver of vaccine hesitancy, the perception that the RSV vaccine offers significant protection against severe disease may have outweighed concerns about side effects in this high-risk population. The non-significant role of accessibility in this study suggests that logistical barriers to RSV vaccination were not a primary concern for participants, but this may not be generalizable to all populations, particularly those in LMICs.
In light of our study findings, several public health strategies can be recommended to improve RSV vaccine uptake in elderly populations. First, educational campaigns should focus on communicating the personal and public health benefits of RSV vaccination, particularly how it can prevent severe respiratory diseases among the elderly. Therefore, promoting the benefits of RSV vaccination such as its ability to prevent serious respiratory infections in seniors should be a cornerstone of public health campaigns aimed at increasing RSV vaccine coverage. Educational interventions should clearly communicate how vaccination can reduce hospitalizations and mortality in elderly populations. Given that perceived benefit was the strongest predictor of positive vaccine attitudes, such vaccine promotion campaigns are likely to resonate with this population. Recently, Michelin et al. emphasized the critical need for educational initiatives and awareness campaigns to enhance understanding of the clinical impact of RSV in older adults. 97 With the introduction of effective RSV vaccines, these efforts become even more important, as they provide a key opportunity to improve RSV vaccine uptake by addressing knowledge gaps and highlighting the serious health risks posed by RSV in this vulnerable population. 97
Second, HCWs should be central to RSV vaccine promotion efforts, as individuals who sought more information from their providers were more likely to accept the RSV vaccine. Ensuring that HCWs are well-equipped to provide clear, evidence-based recommendations for seniors is essential. Finally, addressing conspiracy beliefs through targeted, trust-building initiatives and counteracting misinformation would be critical to reaching those who refuse RSV vaccination.
Finally, this study’s findings must be interpreted within the context of the following limitations. The reliance on a cross-sectional design restricted causal inference, and self-reported data inherently carry risks of recall and social desirability biases. Our decision to employ an online snowball sampling strategy, while pragmatic in expediting data collection across multiple countries, introduced the limitations of a convenience sample. The elderly population’s lower technological proficiency likely constrained participation, contributing to a modest sample size and potentially limiting respondent diversity. Furthermore, the use of Google Forms precluded tracking incomplete responses or calculating a precise response rate, while the unequal distribution of responses across countries reflects disparate levels of survey engagement. Consequently, this study captures general sentiment among participants rather than being representative of broader populations. While cross-group comparisons are presented descriptively, they should be interpreted with caution given the potential for differential survey uptake across countries. Finally, the study did not fully explore other sociocultural factors, such as religious beliefs and political trust, that could impact RSV vaccine attitudes which should be considered in future studies inside and outside the Arab world. Despite these limitations, the study findings can provide valuable initial insights into RSV vaccine attitudes among the elderly in the Arab world, offering a foundation for further inquiry with robust methodology.
Conclusion
In summary, this study provided valuable insights into the possible factors that would influence RSV vaccine acceptance among elderly populations in Arab countries. Our findings highlighted the critical role of perceived benefits, access to accurate information, conspiracy beliefs, and prior vaccination behavior in shaping positive attitudes toward the newly approved RSV vaccines. The significant association between belief in vaccine efficacy and safety highlights the importance of public health campaigns that emphasize these aspects to enhance RSV vaccine acceptance. Moreover, the strong influence of HCWs as trusted sources of information further emphasizes the need for equipping these professionals with clear, evidence-based communication strategies to address RSV vaccine concerns effectively. Conversely, conspiracy beliefs were a significant barrier to RSV vaccine acceptance, reflecting broader trends in vaccine hesitancy. Given the high burden of RSV-related morbidity and mortality in the elderly, especially in the context of recent vaccine approval, it is crucial to prioritize interventions that address the identified barriers to vaccination. Tailored educational materials, community outreach, and trust-building initiatives are likely to be effective strategies for improving RSV vaccine uptake.
Supplemental Material
sj-docx-1-tav-10.1177_25151355251324384 – Supplemental material for Perceived benefits, information, vaccination history, and conspiracy beliefs as significant determinants of RSV vaccine acceptance among Arab seniors
Supplemental material, sj-docx-1-tav-10.1177_25151355251324384 for Perceived benefits, information, vaccination history, and conspiracy beliefs as significant determinants of RSV vaccine acceptance among Arab seniors by Malik Sallam, Kholoud Al-Mahzoum, Zainab Mansour Yousef, Jeelan Saleh Alfouzan, Maryam Jamal Alharbi, Mohammad Khaled Alsubaiei, Mohammed Yahya M. Albalwah, Mohammad W. Shehadeh, Rawan J. Obeidat, Khaled O. Yaseen, Doaa H. Abdelaziz, Nesreen A. Salim, Mohammed Sallam and Muna Barakat in Therapeutic Advances in Vaccines and Immunotherapy
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.