
Abstract
Background:
The global COVID-19 pandemic, declared in January 2020, necessitated urgent preventive measures, with vaccination as a key strategy. Despite progress in vaccine development and distribution, widespread hesitancy persists, impeding global disease control efforts. This study specifically explores COVID-19 vaccine hesitancy and acceptance among Iranian children with asthma, aiming to understand factors unique to this subgroup.
Method:
A cross-sectional investigation was carried out in an allergy clinic in Iran, including a total of 522 asthmatic children between the ages of 5 and 18 years. A comprehensive questionnaire, built upon previous studies, investigated the factors that influence vaccine hesitation and acceptance. Data pertaining to demographics, vaccination status, and factors influencing hesitancy or acceptance were collected.
Results:
Among the participants, 27.5% were administered the COVID-19 vaccine. Decisions were greatly influenced by family dynamics, with a notable association between parent and child vaccination. Children’s vaccination rates were associated with their age and the frequency of COVID-19 diagnosis among their parents. The primary factors motivating individuals to get vaccinated were safety concerns (67.1%) and a strong belief in the severity of COVID-19 (43.4%). On the other hand, vaccine hesitancy resulted from concerns about potential adverse effects (77%), lack of confidence (28.3%), and a belief that children who had already contracted COVID-19 did not require vaccination (22.5%).
Conclusion:
The study highlights COVID-19 vaccine hesitancy and acceptance among asthmatic children in Iran, emphasizing parental decision-making factors. Tailored interventions are required due to the lower vaccination rate in this specific group. Healthcare providers play a vital role in influencing opinions, urging actions against misinformation, enhancing vaccine understanding, and promoting positive attitudes.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) was first reported in China, and its outbreak was announced as a pandemic in January 2020. It has caused clinical features in more than 770 million cases and roughly 7 million deaths worldwide until September 2023.1,2 This fast-spreading viral disease usually presents with a spectrum of clinical features and can lead to severe respiratory distress and death. 3 Even though World Health Organization (WHO) stated the end of the pandemic in May 2023, 4 it is still considered a global health threat. As for any other infectious disease, vaccination has been regarded as a practical and trustworthy approach for preventing and controlling the pandemic. 5 Since no effective and curative treatment has been introduced for the management of COVID-19, the only strategy taken at the very first time of the virus’s emergence was prevention through social distance and self-protection, which was practically impossible to continue for a long time. This highlights the importance of vaccination as a more rational method of prophylaxis. 6 COVID-19 vaccines set an exceptional record in terms of shrinking the time of production and approval processes. 7 The first COVID-19 vaccine successfully got official permission from the FDA for urgent use in the late weeks of 2020, followed by the introduction of several vaccines safely applied to millions of people worldwide. According to the WHO, the total count of COVID-19 vaccines administered until September 4th, 2023, amounted to 13,500,135,157. Nonetheless, there is still a pretty large number of people who have remained reluctant to be vaccinated against SARS-CoV-2.2,8 WHO regarded this as a health disaster that placed a significant obstacle in the way to stop the pandemic, and the relevant predisposing factors were evaluated in several studies. 9 These surveys addressed some contributing factors to the growing number of people who have been unwilling to be vaccinated, including age, gender, education, socioeconomic status, insurance coverage, ethnic group, place of living, and their assessment of vaccine safety and effectiveness, in addition to the cost of the vaccine. 10 Interestingly, age was found to be the most constant influential factor in people’s disinclination to be vaccinated. In other words, the younger the people were, the more hesitant they were. Consequently, unvaccinated children and adolescents can keep the transmission chain active and prevent it from breaking. Unless almost all adults are immunized, an acceptable proportion of the immune population is impossible to achieve. 9 Vaccine hesitancy has also been reported in allergic patients, which has largely been attributed to being worried about allergic or other adverse reactions to the vaccine. 11 According to WHO, vaccine-hesitant individuals put all community health at risk, underscoring the importance of addressing the issue of vaccination reluctance more seriously. 12 Considering the critical role of culture and beliefs, among many other elements, in people’s approach toward vaccination, this survey was designed to evaluate the reasons behind vaccination hesitancy in Iranian asthmatic children.
Materials and methods
A cross-sectional study was designed, and the sample size was calculated using the Cochrane formula. The previous publications reported that approximately 60% of parents were unwilling to vaccinate their children, 3 and with an error margin of 0.05, the optimum sample size was estimated to be 385. To cover the design effects, it was finally calculated to be 500. Data for this study were collected over a 1-year period at two highly specialized asthma and allergy centers in Tehran and Karaj. Asthmatic 5- to 18-year-old patients referred to these centers for follow-up visits were enrolled. Their parents were asked to fill in the questionnaire if they signed the informed consent to participate in the survey. Patient selection was made regardless of gender, the level of parental education, the level of asthma control, ethnic group, or living place. Patients who were suffering from other chronic disorders, including diabetes mellitus, chronic renal failure, chronic heart diseases, epilepsy, rheumatologic disorders, and any other chronic diseases requiring continuous medical therapy, were excluded from the study. The questionnaire was designed based on the author’s thorough research of the existing database, focusing on the previously published papers addressing the factors behind COVID-19 vaccine hesitancy in other communities. The variables included gender, age, the education level of the parents, living place, their point of view about the treatability of COVID-19, history of receiving the COVID-19 vaccine, history of COVID-19 infection, history of hospital admission for COVID-19, and history of death due to COVID-19 in relatives. Regarding the specific questions to find out the reasons behind the willingness or hesitation of vaccination against COVID-19, a total of 21 questions were designed and then reviewed by a group of experts to confirm the face and content validity. The reliability of the investigations was assessed by calculating Cronbach’s alpha value, which yielded a score of 0.75 for both questionnaires, signifying a satisfactory level of reliability. All participants enrolled entirely voluntarily and were assured that the data would be treated strictly confidential. Parents who took their children to the clinic answered the questions. Although it was a self-administered questionnaire, one of the research team members was always there to clarify any confusion while filling in the questionnaire.
Statistical analysis
The SPSS Statistics, version 26, was applied to analyze the data. Descriptive and analytic statistics were used to present the data distribution and assess the association between different variables and vaccination. Simple one-way T-test analysis and chi-squared test were performed to evaluate the correlation between sociodemographic elements and factors contributing to vaccine hesitancy. Logistic regression analysis was conducted to test a model predicting vaccination. A statistically significant relationship between variables was defined as a p-value less than 0.05.
Results
The demographic characteristics of the study participants are outlined in Table 1. Among the 522 individuals included, 144 (27.5%) had received the COVID-19 vaccination. The median age of participants was 8.8 years, with a predominant representation of males (63.1%). A total of 196 participants (38.7%) reported a history of previous COVID-19 diagnosis, and 361 participants (73.2%) indicated a previous COVID-19 diagnosis among their family members. Furthermore, 459 participants (87.9%) reported that both parents had been vaccinated against COVID-19.
Baseline demographic information in vaccinated and unvaccinated populations.

The percentage of illiterate mothers and fathers was comparable, with 1.7% for mothers and 1.9% for fathers. Regarding undergraduate or higher degrees, the majority of mothers (61.1%) and fathers (59.5%) possessed education beyond the undergraduate level. Notably, a higher percentage of fathers (23.4%) held a Master’s degree or higher than mothers (16.7%).
The chi-squared test revealed a significant association (p-value: 0.004) between the intention to vaccinate both parents and their children, indicating a cohesive pattern in parental vaccination decisions. Furthermore, children’s vaccination status demonstrated correlations with their age (p < 0.001) and a previous COVID-19 diagnosis in parents (p-value: 0.039). Nevertheless, there was no statistically significant effect on the child’s vaccination status when considering other demographic factors, such as a previous COVID-19 diagnosis in family members (p-value: 0.087), hospitalization history of family members due to COVID-19 (p-value: 0.093), death of relatives due to COVID-19 (p-value: 0.600), and the father’s level of education (p-value: 0.066; Table 1).
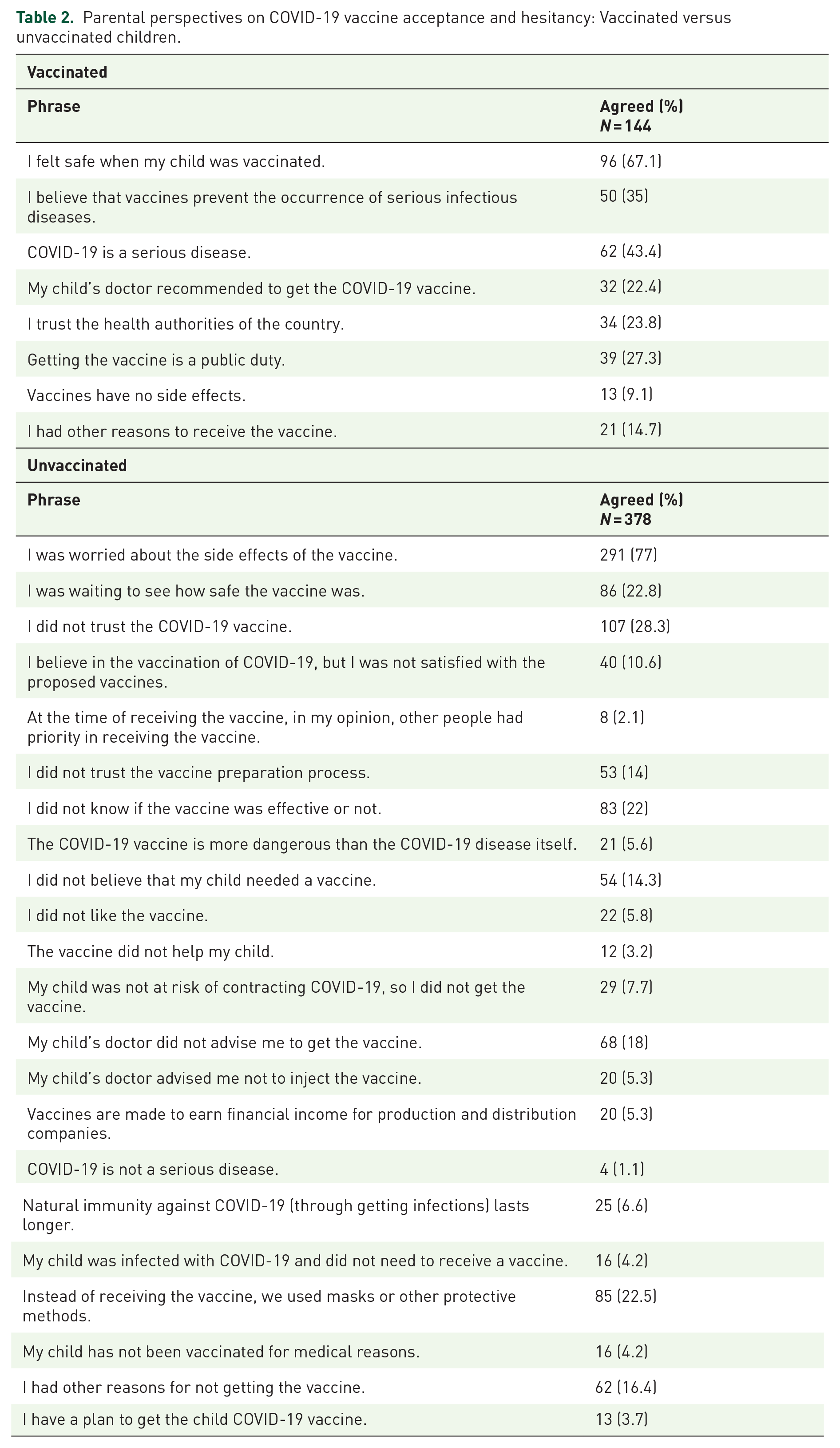
Based on the data collected from the questionnaire, Table 2 presents the reasons why parents choose to vaccinate their children and why some parents opt not to vaccinate their children. The main factors mentioned were the perception of child immunization as a means of ensuring safety (67.1%) and the conviction of the seriousness of COVID-19 as an illness (43.4%). On the other hand, significant reasons that contributed to vaccine reluctance were worries about the adverse effects of the vaccine (77%), a lack of confidence in the COVID-19 vaccine (28.3%), and the belief that their child had already been infected with COVID-19, thereby making immunization unnecessary (22.5%). Respectively, a mere 3.7% of parents had intentions to vaccinate their child (Table 2).
Parental perspectives on COVID-19 vaccine acceptance and hesitancy: Vaccinated versus unvaccinated children.
A logistic regression analysis was performed (95% confidence interval) to determine the predictability of significant factors such as age, parents’ vaccination against COVID-19, parents’ education, and previous diagnosis of COVID-19 in the vaccination of participants. In this multivariate analysis for vaccination (dependent variable), just age, parents’ vaccination against COVID-19, and father’s education were considered in the model as predictors (Table 3).
Logistic regression analysis of vaccination predictors COVID-19.

Discussion
The results of our study demonstrated a strong correlation between the vaccination of parents and their children against COVID-19, highlighting the interdependence of their decision-making process. Notable associations were found between vaccination status and both the age of the child and whether the child had previously been diagnosed with COVID-19. Although there were changes in family-related characteristics, they did not achieve statistical significance. Our study, involving 522 participants, revealed that 144 individuals (27.5%) had received the COVID-19 vaccination. This amount is significantly below the stated immunization rate among adults in Iran, which ranges from 64.2% to 83.6%. 13 Also, the proportion appears notably to be lower than the average proportions reported in other studies. A recent systematic review and meta-analysis highlighted that the overall proportion of parents intending to vaccinate their children against COVID-19 is moderate at 60.1%, showcasing considerable variability across studies, ranging from 25.6% to 92.2%. 3 This observed value was notably lower than the intentions reported among parents of healthy children in various countries. For instance, intentions in other studies stood at 77.2% in Australia, 14 73% in Brazil, 15 51.5% in the United States, 16 50.6% in Ireland, 17 45.1% in Thailand, 18 and ranged from 41.9% to 45.4% in Canada. 19
In a study in Italy, it was found that almost one-third (29.9%) of participants expressed a willingness to vaccinate their vulnerable children against COVID-19. Meanwhile, 21.3% remained uncertain, and 48.8% indicated no intention to vaccinate. Notably, parents exhibiting a heightened perception of the vaccine’s utility and safety, particularly those who received information from pediatricians, were more inclined to express a willingness to vaccinate their children. 20 In another study conducted in China, the COVID-19 vaccination rate among asthmatic patients was 73.6%, lower than the general population rate of 87.64%. Individuals influenced by the vaccination decisions of family members and colleagues were more likely to get vaccinated. Notably, patients with poorly monitored asthma and those using biologic therapies had lower vaccination rates. The adverse effects of COVID-19 vaccines in asthmatic patients mirrored those in the general population. 21 In another study performed in Iran, parents of children with asthma exhibited significant anxiety regarding the potential impact of COVID-19 on their asthmatic children. This concern appears to extend to their views on the COVID-19 vaccine as well. 22 Both patients and physicians may exhibit hesitancy regarding vaccination in individuals with asthma, potentially leading to reduced vaccine uptake. However, it is crucial to highlight that numerous studies have demonstrated the effectiveness of vaccines in preventing hospitalization for COVID-19 and respiratory failure associated with COVID-19 among patients with chronic respiratory diseases, including asthma.21,23,24 Therefore, a clear and compelling rationale exists to encourage and promote COVID-19 vaccination in individuals with chronic respiratory diseases, such as asthma.
Several studies emphasize physicians’ pivotal role in vaccine decision-making.25–29 This is particularly crucial in patients with chronic conditions like asthma. Parents who receive information from their physicians are more likely to express a willingness to vaccinate their children compared to those who obtain information from other sources or have not acquired information. This preference may stem from parents’ established trust and longer-term relationship with their physicians, fostering confidence in their recommendations. As the information source correlates with vaccination intent, physicians and healthcare workers must be utilized to address parental concerns and effectively communicate accurate and pertinent information about the COVID-19 vaccine. It is noteworthy that many parents acquire information through social networks and the internet, sources that may negatively impact their understanding and decision-making regarding vaccination for their children. This is concerning, as prior literature on vaccines has identified social networks and the internet as potential sources of misinformation, leading to unwillingness, hesitancy, and reduced uptake.30–32 Furthermore, simply 22.4% of children received vaccinations based on their doctor’s advice, which does not seem excessively impressive.
Our study uncovered several factors that significantly predicted parents’ willingness and hesitancy toward vaccinating their children against SARS-CoV-2. Notably, alongside the previously reported association with the source of information, respondents’ attitudes emerged as crucial determinants. Specifically, our findings highlight that parental positive attitudes toward the utility and safety of this vaccination strongly influence their willingness to vaccinate their child against COVID-19. This discovery aligns with the results of several recently conducted studies, underscoring that parents’ perspectives on the overall efficacy of vaccines play a pivotal role in determining vaccine acceptance.17,18,20,33–36 Hence, implementing public health education programs targeting parents with a negative attitude toward the utility of the COVID-19 vaccine could lead to increased vaccine acceptance and uptake.
Our study revealed two primary factors contributing to parents’ decisions against vaccinating their children: apprehension regarding potential vaccine side effects and a pervasive lack of trust in the COVID-19 vaccine. In addition, these findings underscore the significance of addressing these concerns to foster a better understanding of vaccine safety and efficacy, ultimately contributing to improved vaccination rates among children. Moreover, parents in the United States expressed hesitancy toward the COVID-19 vaccine, highlighting the need for more reliable information to boost their confidence in vaccination.37–39
The finding that the vaccination status of children correlates with their age, with older children having a higher vaccination rate than younger children, suggests a potential trend of increased vaccine acceptance or uptake as children grow older. This could be attributed to several factors, such as changes in parental attitudes, increased awareness of vaccine importance, or evolving vaccination schedules that prioritize certain age groups. Understanding this age-related correlation is crucial for tailoring vaccination outreach and education strategies to address the needs and concerns of different age groups effectively. Perhaps this is because parents express greater concern regarding the potential adverse effects of vaccines while their children are young, as opposed to when they are older. Moreover, the prevalence of COVID-19 among young children during the pandemic was comparatively lower than that observed among older children. This may reduce parental concern regarding the susceptibility of their young children to getting infected with COVID-19 and its associated consequences, thereby diminishing their willingness to be vaccinated.
Several limitations should be acknowledged in our study. First, reliance on self-reported data introduces potential bias, as respondents may provide information based on their perceptions or experiences. Moreover, the cross-sectional design employed in this study restricts our ability to establish causation or discern temporal trends. Although the sample size is substantial, it is imperative to scrutinize the representativeness of the population and potential generalizability issues. It is noteworthy that the questionnaire was voluntarily completed by subjects interested in the study, introducing a potential response bias. Furthermore, the staggered vaccination rollout, where adults received vaccines earlier than children for health policy reasons, adds complexity to our findings. During the study, the promotion of booster doses in adults and initial doses in children was ongoing. This temporal aspect underscores the dynamic nature of vaccination intentions, which may evolve over time and not necessarily align with actual vaccination behavior in the future. These factors may contribute to the observed low rate of vaccine hesitancy in children and the contrastingly high rate in adults. 40
Conclusion
Our research reveals the intricate situation of COVID-19 vaccine hesitancy among parents of asthmatic children in Iran, highlighting a lower immunization rate compared to the whole population. The main variables that contribute to vaccine hesitancy include parental attitudes, concerns about possible side effects, and a lack of confidence in the COVID-19 vaccine. Healthcare practitioners have a considerable influence on vaccination choices, underscoring the need for targeted interventions to promote positive attitudes. To increase the acceptance of vaccinations, it is essential to address safety concerns, give trustworthy information, and implement tailored public health education. Despite the study’s shortcomings, such as relying on self-reported data, these findings underscore the importance of ongoing efforts to decrease vaccine hesitancy. Ensuring the well-being of asthmatic children and the wider community is crucial in the ongoing fight against COVID-19.
Footnotes
Acknowledgements
The authors would like to acknowledge the patients and their families for participating in the study and permitting the report of their relative conditions.