
Abstract
Background:
India has almost 225 million adolescent girls and they seem to be at a disadvantage, both economically and by their lack of knowledge on human papilloma virus (HPV) vaccine, when compared to adolescent girls of other Asian countries.
Aim:
To assess the prevalence of HPV vaccination and to identify the impact of education in improving the knowledge and perception about the HPV infection and vaccination among the parents of adolescent girls.
Methodology:
The prospective interventional study was conducted in four schools within a South Indian City, Mysuru. The informed consent form and the questionnaire were sent home with the identified adolescent girls during the pre-interventional phase. Educational sessions were conducted for the students in their school and an education leaflet was distributed to their parents. Three weeks later, questionnaires were re-administered to the parents via the enrolled girls and their responses were collected.
Results:
The prevalence of HPV vaccination in the study population was 4.4%. There was a statistically significant improvement in knowledge in the post-interventional phase of the study (p = 0.001), but could not identify a significant change in their perception (p = 0.479). Parents belonging to the socioeconomic class of upper middle and upper lower showed better improvement at the end of the study, with a percentage improvement of 58.93% and 48.44%, respectively.
Conclusion:
The study proved that the healt care professional can target school children to communicate effectively to their parents on the importance of HPV vaccine as the study clearly observed a positive behavioral change among the study population.
Introduction
Immunization is one of the most cost-effective public health interventions and has been proved to reduce the mortality rate by over 15% in children younger than 5 years.1,2 Out of 27 million children born in India each year, only 44% complete the vaccinations as per the schedule. As per the vaccine coverage evaluation survey conducted by United Nations International Children’s Emergency Fund (UNICEF), the reasons for partial/non-immunization was, ‘did not feel the need’, ‘not knowing about the need’ and ‘not knowing where to go for vaccination’ in 28.2%, 26.3%, 10.8% cases, respectively, which shows that lack of awareness is the common barrier in achieving maximum immunization coverage. 2 Parental basic education and knowledge on the need and benefit of vaccination plays a major role in the vaccination coverage as they are the decision-makers on their child’s immunization. 3 Vaccines provided under the universal immunization program of India are bacillus Calmette–Guerin (BCG) vaccine, oral polio vaccine (OPV), hepatitis B vaccine, pentavalent vaccine (combination of diptheria, tetanus, pertusis, haemophilis influenza type B infection and hepatitis B), pneumococcal conjugate vaccine (PCV), fractional inactivated poliomylitis vaccine (fIPV), measles/measles and rubella (MR) vaccine, Japanese encephalitis (JE) vaccine, diphtheria, tetanus and pertussis (DPT) booster vaccine and tetanus toxoid (TT) vaccine. 4 The National Family Health Survey (NFHS) found that the national immunization rate has increased from 44% (assessment year 2005–2006) to 62% in the assessment year, 2015–2016. Currently, India has a gap of 38% for achieving universal vaccine coverage. In order to fulfil the required target, India has to ensure full immunization of about 27 million children per year to reach the target by the year 2030.5,6
Cervical cancer is the fifth most common cancer in the world and third most common cancer in India, which accounts for 26.5% of global cervical cancer cases. 7 Cervical cancer is the second leading cause of cancer-related deaths in women aged 15–44 years. 8 It is estimated that the incidence of cervical cancer is 122,844 with a death rate of 67,477 per year. 7 The major risk factor for cervical cancer is human papilloma virus (HPV) infection. Cervical cancer is ranked as the most frequent cancer in women in India, and they face a 2.5% cumulative lifetime risk and 1.4% cumulative death risk from cervical cancer.
There are over 150 serotypes of HPV, 40 affect the genital area and may not cause a serious risk to health, but of these 15–20 are oncogenic in nature. The most common strains which are associated with cervical cancer are HPV-16 and 18 and account for more than 75% of cervical cancer cases in India.7,8 The use of HPV vaccine has proved to reduce the incidence rate of cervical cancer by over 50%. 9 There are two HPV vaccines commercially available in India (Gardasil, a quadrivalent vaccine and Cervarix- a bivalent vaccine) since 2008 and are recommended for adolescent girls aged 9–14 years; however, vaccination can be extended up to the age of 26 years.8,10,11 The government of India has made initiatives to introduce HPV vaccines under the expanded program of India (EPI) in some states of India such as Delhi, Punjab, Gujarat, Andhra Pradesh and Telangana (Khammam district) from November 2016.6,12 The Indian Academy of Pediatrics Committee on Immunization (IAPOI) recommends HPV vaccine to all girls and women who can afford the vaccine. 11
HPV vaccination coverage is lower among the Indian population because of the lack of awareness about HPV, the absence of proper screening programs, lack of availability of vaccine and the high cost. Studies conducted in different part of the world show that education on HPV infection and vaccination plays a critical role in HPV vaccination uptake.13–15 India needs to take an initiative to be a part of 79 countries such as Hong Kong, Malaysia and Singapore, that have included HPV vaccine in their national immunization program so that the prevalence of this cancer can be reduced. 16 This study was planned to assess the knowledge and perception (KP) of HPV infection and vaccination among the parents of adolescent girls, to determine the prevalence of HPV vaccination among female children of the study population and to identify the impact of education on the knowledge of HPV vaccination among the parents.
Materials and methods
Study setting and sampling method
The study was a prospective interventional study conducted for 6 months, from October 2017 to March 2018 in Mysuru, a South Indian City. The study subjects were the parents of adolescent girls aged 11–16 years. Study sites were four schools within Mysuru City. Study sites were selected based on the availability of the adolescent girls of the age group 11–16 years and permission from the school authorities in the conduct of the study. Other criteria for the site selection were the syllabus of the school [Central Board of Secondary Education (CBSE), Indian Board of Secondary Education (ICSE), Kannada Medium State Syllabus and English medium State Syllabus] to ensure the participation of the population from all the different socioeconomic classes. A study-specific informed consent form (ICF) was prepared in English as per the Indian Council for Medical Research (ICMR) 17 guidelines and was translated into Kannada, which was then back-translated into English to ensure the readability of the consent form. Ethical clearance of the study was obtained from the localised institutional human ethical committee (ref no.: JSSCPM/IHEC/2017/024).
Development of study tools
Development and validation of KP questionnaire
The study team developed a questionnaire based on an extensive literature review using the following keywords: human papilloma virus, HPV questionnaire, HPV study, parents’ knowledge on HPV, validation of questionnaire, content validity index using search engines such as Google scholar, Science Direct, PubMed/Medline and Clinical Key. The questionnaire included questions that sought to gain information about the parents’ knowledge about HPV infection and also had questions to evaluate the subjects’ perception towards HPV vaccination. The finalised questionnaire had provisions to collect the following information: (a) demographic details of the subject such as parent enrolled, number of children, type of family, place of living, and socioeconomic background; (b) socioeconomic status using the revised Kuppuswamy socioeconomic scale 18 where the subjects were categorised into ‘upper’, ‘upper middle’, ‘lower middle’, and ‘lower’ class; (c) knowledge questions: which included questions about the mode of transmission of HPV infection, severity, complications, number of doses of vaccine, etc.; and (d) perception questions which included questions about the respondent’s attitude and willingness towards HPV vaccination. The questionnaire had 18 questions, of which five questions had yes/no answer options, four had yes/no/do not know answer options, and the remaining questions had different answer options (one question had three options, two had four options, three had five options and three had seven options) depending on the questions asked.
The questionnaire was then subjected for content validity, by a set of 20 experts in the related field (postgraduate students, lecturers, research scholars and clinical pharmacists). The experts were asked to rate the items based on relevance, clarity, simplicity and ambiguity on a scale ranging from 1 to 4. The content validity index (CVI) developed by Waltz and Bausell was used. Items CVI (I-CVI) was used to assess the average score of individual questions.19,20 The collected data were entered into an Excel spreadsheet for easy calculation and retrieval followed by the analysis using the statistical package for social studies (SPSS) software version 22. The reliability/internal consistency of each question in the questionnaire was estimated using Cronbach’s alpha. The final questionnaire was translated into Kannada and then back-translated into English by linguistic experts to ensure that the questionnaire maintained consistency in language and understanding. The test and retest reliability of the questionnaire was performed to assess the internal consistency among 10 adolescent girls’ parents. Spearman’s rank coefficient was then calculated to investigate the test–retest reliability of the developed questionnaire.
Development of information leaflet
A leaflet was developed based on guidelines published in previous literature,21–23 and suggestions were obtained from experts in the related field. The leaflet had information about the disease condition, risk factors, causes, management and prevention of HPV infection with required images and captions. Three experts in the related field performed the face validity of the leaflet. The final leaflet was translated into the local language, Kannada, and back-translated into English to ensure the consistency in language and understanding. The information leaflet was subjected for its readability using the Flesch readability ease formula and Flesch Kinkaid readability test.24,25 The quality of information in the leaflet was assessed using the ensuring quality information for leaflets (EQIP) tool, 26 and the layout and design were assessed using Baker able leaflet design (BALD) criteria. 27
Study procedure
Adolescent girls aged 11–16 years studying at the study sites were approached and informed about the purpose and procedure of the study. Students were requested to carry a copy of the informed consent form with them to their parents and were asked to bring back the signed ICF if the parent was willing to take part in the study. Kannada and English ICFs were used based on the language preference of the students approached.
The questionnaire was sent via the adolescent girls to the consented parents and they were requested to bring the questionnaire back after it was filled in by their parents. Subsequent visits were made to the respective schools on the third, sixth and ninth days, respectively, for the collection of the filled questionnaires. A convenient date was fixed as per the permission granted from the respective school authorities for conducting the awareness program for the students. Awareness programs were conducted for each school with the help of standardised educational material about HPV infection and vaccination. After the educational session, information leaflets were also distributed to the students (in both Kannada and English) and they were requested to give the to their parents. Three weeks after the educational session, the KP questionnaire was re-administered to the study population through the adolescent girls. Researchers made three more visits on the third, sixth and ninth days to collect the post-interventional questionnaire. The collected data were entered into an Excel spreadsheet for easy calculation and retrieval followed by the analysis using the statistical package for social studies (SPSS) software version 22. Comparison of pre and post-knowledge, attitude, practice and total KP were done using a paired sample t-test and Analysis of Variance (ANOVA). A p value of <0.005 was considered statistically significant, with a 95% confidence interval.
Results
Validation of study tools
Questionnaire
The validation experts had scored each question in the questionnaire for the relevance, clarity, simplicity and ambiguity. The overall content validity score and item content validity index (I-CVI) of the prepared questionnaire was 93.74% and 3.75, respectively. The internal consistency of the questionnaire was measured using Cronbach’s alpha and was found to be 0.84. The calculated Spearman’s rank correlation coefficient value was 0.957 (p < 0.001) for the test–retest reliability.
Information leaflet
Based on the scoring assessed in the initial round, the quality information in the EQIP questionnaire for the developed patient information leaflet was restructured and reassessed again, which was then found to be 62.5%.The final (Flesch Reading Ease) FRE score achieved was 70.8 and Flesch Kincaid – Grade Level (FK-GL) achieved was 5.2. According to BALD assessment the leaflet showed a total score of 25.
A total of eight schools were approached for the conduct of the study, of which four schools granted permission to conduct the study. The study identified a total of 809 potential subjects, of whom the parents of 403 adolescent girls showed their willingness to participate in the study, with a response rate of 49.81%. Mothers and fathers participated almost equally. The study participants mostly belonged to the socioeconomic class of upper middle (32.25%) and lower middle (31.36%). The majority of the participants (73.2%) were residing in urban areas. The demographic details of the study population are presented in Table 1.
The demographic details of the study population.
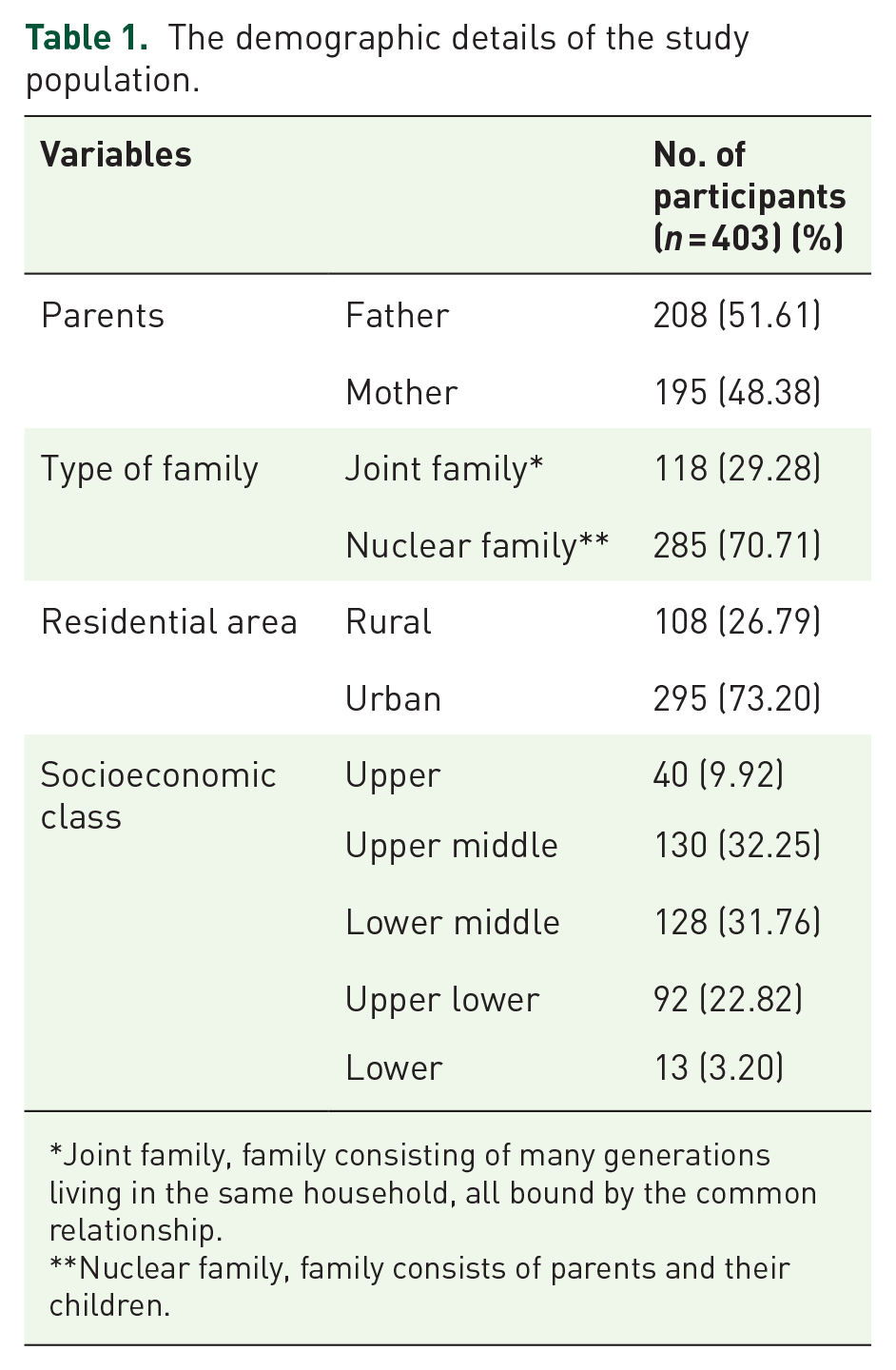
Joint family, family consisting of many generations living in the same household, all bound by the common relationship.
Nuclear family, family consists of parents and their children.
Out of the 403 enrolled participants, 44.6% of subjects had previously heard about HPV infection and 23.5% about HPV vaccine. However, after the educational session, the awareness about HPV infection and vaccination was increased to 77.5% and 66.2%, respectively. Among the study population, 0.4% of the study population were under the impression that HPV only infects boys and men, 11.4% of the population said that HPV affects only girls and women and 26.3% of the population said that the infection affects both male and female individuals. After the conduct of the educational session, the majority of the participants (56.8%) understood that HPV can infect both male and female individuals. The percentage of the population who ‘don’t know’ about the population infected by HPV decreased by approximately 36%. There was a significant improvement in the knowledge about the mode of transmission of HPV infection. The percentage of wrong answers (which included answers such as transmitted via insects, contaminated food and water, etc.) given after the educational session decreased by about 20%. While comparing the pre-intervention and post-intervention, participants’ response on cervical cancer being caused due to HPV infection increased from 24.56% to 63.43%. The knowledge of subjects on HPV-infected persons having symptoms was increased by 33.95% after the intervention. It was stated by 23% of the respondents that the vaccine does not cause harm. The majority of the subjects did not know the answer to this question before the educational session. The scores on the knowledge about HPV infection and vaccination is presented in Table 2.
Knowledge about HPV infection and vaccine.

HPV, human papillomavirus.
Among the enrolled subjects, the severity of HPV infection was not known by 74.68% of the study population in the pre-interventional phase and the same decreased to 40.62% after the completion of the educational session. The study observed an improvement in the knowledge about the prevention of HPV infection. There was an improvement of 26.54% in the awareness about the availability of HPV vaccine for the prevention of infection after the intervention. There was also a substantial decrease in the number of subjects who did not know about the prevention of HPV infection. Many of the subjects (n = 201) did not know about any of the preventive measures for the infection in the pre-interventional phase, whereas only 70 subjects did not know the answer to this question after the educational session. Only 16.3% of the study population answered 9–14 years is the recommended age for HPV vaccination in the initial phase of the study, whereas 61% of them did not know the answer to this question. Only 35 (8.68%) participants answered the correct schedule of HPV vaccination while the others answered incorrectly or did not know the answer; 318 (78.9%) said that they did not know about the number of doses of vaccine required. The knowledge regarding the HPV vaccination schedule increased from 8% to 35% in the enrolled subjects.
Perception about HPV vaccine
There was no statistically significant difference shown while evaluating the perception among the enrolled participants, of which only 4% of them have already vaccinated their child with HPV vaccine, whereas 95% of them have not vaccinated their child. Last but not the least, the parents’ opinion was also taken into consideration with respect to vaccinating their children, 39.7% of the parents agreed to vaccinate their wards, 56.25% of them agreed to recommend the need for HPV vaccine to others. After the education intervention, a positive behavioral change was seen towards the willingness to vaccinate their children and recommending the need for vaccinating their children by 57.18% and 42.81%, respectively.
Reasons for non-vaccination
To the research question regarding barriers to HPV vaccination, 17.8% of the study population stated that HPV vaccination prophylaxis is not necessary, 10.42% were concerned about the safety of the vaccine, 4.46% had socioeconomic issues, 2.72%were concerned about the high cost of the vaccine and 6.94% reported that they were not aware about the existence of a vaccine for HPV infection (in the pre-interventional phase of the study).
Prevalence of HPV vaccination
The prevalence of HPV vaccination identified during the pre-interventional phase of the study was 4.4%, while it increased to 7.1% in the post- interventional phase.
Impact of education on KP of HPV infection
Our study clearly pointed out that there was a statistically significant difference in the knowledge gained in the post-interventional phase of the study. Among the enrolled participants, fathers showed a higher improvement in knowledge, with over 30% showing a positive perception with regard to HPV vaccination. Nuclear families showed an improvement in knowledge of about 30% and an improvement in perception rates of about 10% when compared to joint families. However, families residing in rural areas had similar improvements in KP when compared to families residing in urban areas. The detail of the impact of education on KP of HPV vaccination is shown in Table 3. Statistically significant improvement in KP of parents was shown irrespective of the demographic details such as gender (p = 0.001), type of family (p = 0.001), place of living (p = 0.001) and socioeconomic status (p = 0.001).
Impact of education of knowledge and perception of HPV vaccination.
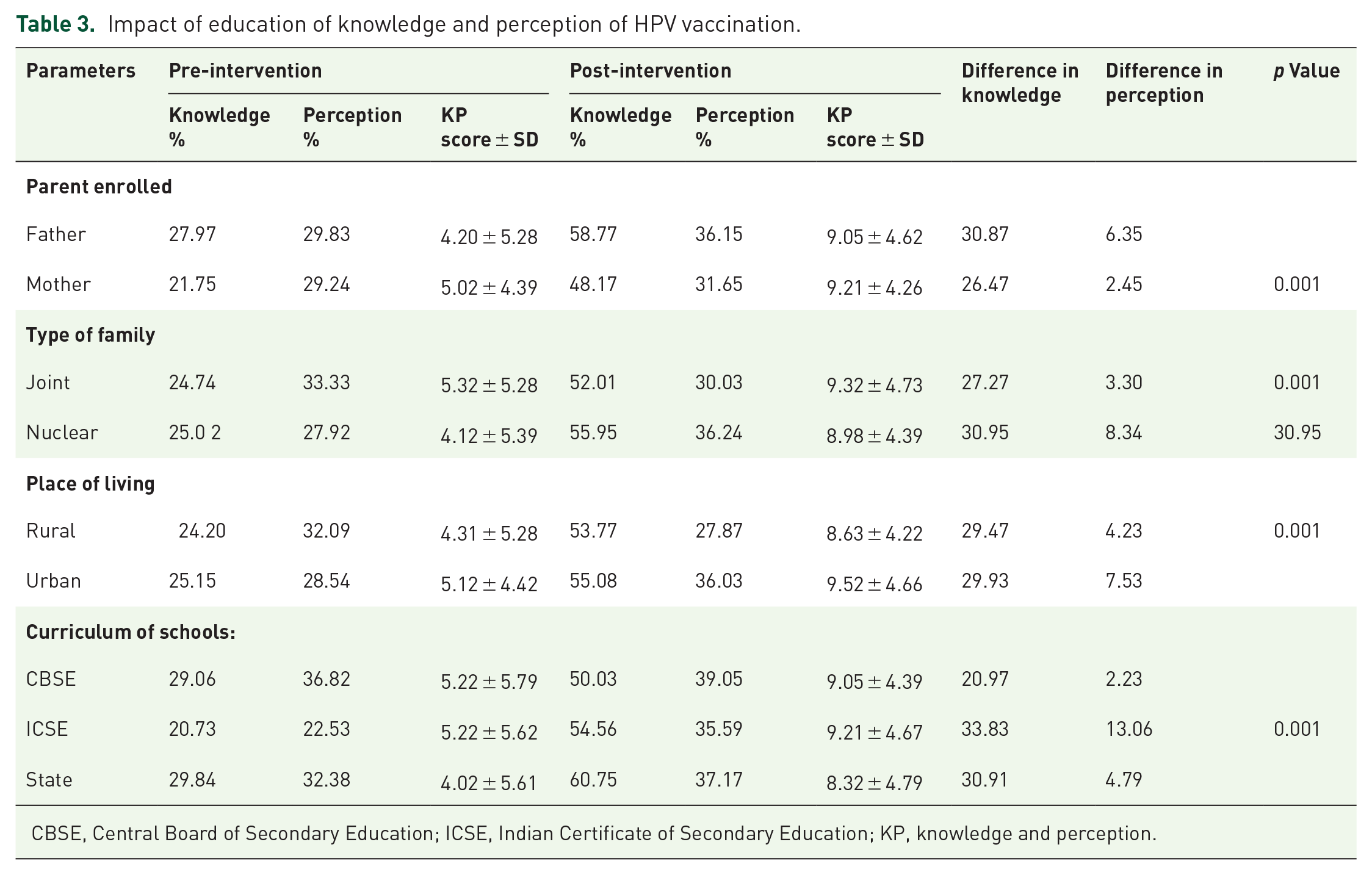
CBSE, Central Board of Secondary Education; ICSE, Indian Certificate of Secondary Education; KP, knowledge and perception.
Statistical analysis of KP
The study found a significant increase in knowledge and KP before and after the study. However, there was no statistically significant improvement in the perception alone. The statistical analysis of the KP is described in Tables 3 and 4.
Statistical analysis of knowledge and perception.

KP, knowledge and perception; SD, standard deviation.
Discussion
As the content validity score core was more than 80%, none of the questions were revised or deleted from the prepared questionnaire. Hence, the questionnaire could be used as a standard tool in further studies among the parents of adolescent girls having a moderate level of education and socioeconomic status. The FRE and FK-G scores suggest that the readability of the information leaflet is ‘standard’ and the grade level indicates that 11–13-year-old students easily understand the leaflet. The EQIP score of 62.5% means that the educational material can be used for 1–2 years without any revision. The BALD score of 25, which rates the design and layout of the information leaflet as ‘above standard’, and can be used as a standard tool to educate the study participants.
The study found a significant improvement in the KP of parents after the indirect education through their adolescent girls. The study described that the information leaflet also has significantly helped to improve the KP of parents on HPV infection and vaccination. Our study has also pointed to the importance of conducting awareness and outreach programs, which create awareness and vaccination impact of education of HPV infection and vaccination among the population of school-aged adolescent girls and their parents. In Indian settings the incidence of cervical cancer has increased to 141,566 million due to the lack of awareness and outreach programs. Therefore, our study has targeted adolescent girls and their parents for the study of HPV infection and vaccination. Our study also emphasized and guided them with necessary information, which would provide better knowledge for the future.
In the study, the study population enrolled for this study was divided based on their demographics such as their parents, type of family, place of living, socioeconomic class. This division among the population has provided us with a deep understanding of their KP of HPV infection and vaccination before and after education. Among the parents who enrolled for the study, fathers were shown to be high in number at 51.61% against mothers at 48.38%. There were also other similar studies showing that fathers were enrolled in a higher proportion among the enrolled population.28,29 Based on the Kuppuswamy classification for the socioeconomic class divided into upper, upper middle and lower middle, the upper middle, upper lower and lower and the socioeconomic background of upper middle class showed the highest response rates of 32.25%.
In this study, our method of assessing or understanding the KP of the population was given through the questionnaire. Our questionnaire consists of a set of questions for KP. The questionnaire was prepared in an effortless manner, which was understood by the parents. The questions focused on the source of information the population gained from such as the severity, modes of transmission, prevention of HPV and their reasons for non-vaccination, and positive behavior towards HPV vaccination. The response provided by the population showed a moderate range of knowledge before the education. The respondents showed that their source of gaining knowledge was newspapers(14.3%) and healthcare professionals (12%). There were also other similar studies which took up this questionnaire and showed that the textbooks and teachers showed higher response rates.8,30
People who enrolled for this study showed much less interest in vaccination of their children for HPV as they have financial barriers and they proved that HPV vaccine prophylaxis is not necessary, while on the other hand some had a fear of side effects of this HPV vaccine.
This study reflects viewpoints from both men and women, which allowed us to capture a more comprehensive picture of KP and for the HPV vaccine in the general population. However, we acknowledge several limitations. First, owing to the nature of the design, we cannot establish causal links for the HPV vaccine and its associated factors. Second, we recruited our sample by using the convenience sampling technique, which limits the capacity to generalize our results to other settings. Moreover, this study was carried out in the vaccination clinic, where people may have better KP and a greater willingness to pay for the HPV vaccine than those in the community. Finally, although some preventive procedures were followed, recall bias and social desirability bias may have occurred, which could affect the main findings of this study.
The results of the study (Table 3) clearly describe that there is a significant improvement in KP scores of different subgroups such as gender, type of family, place of living and curriculum followed by the school after the educational intervention. The leaflets provided were simple and easy to understand by any parent and also have influenced the results of the study along with the indirect education provided to the adolescent girls. Previous studies also showed a positive influence on education using leaflets on HPV.31,32
Similar results were seen in a study conducted by Turiho et al., which proved that, in order for an increase in perception among the population, it would be difficult due to misconceptions about the safety of the HPV vaccine which were largely based on the growing fear about adverse effects due to vaccination. 33 The parents enrolled in the study conducted by the same authors also believed that vaccinations in general cause illness of children and they initially feared that the HPV vaccination would be dangerous.
Conclusion
The results of our study revealed a poor understanding about health-related problems associated with HPV infection among parents, its prevention and modes of transmission. Nearly half of the subject population was unaware of the availability of the HPV vaccine, the importance of taking preventive measures and its importance in the prevention of cervical cancer. However, 43.75% of the respondents were willing to get vaccinated against HPV. The study observed that awareness programs conducted in schools were the right medium to reach the desired target groups who were otherwise unable to reach. The study results concluded that the gap filled between the knowledge gained before and after the intervention was significantly high, whereas results for the perception did not show any significant improvement. Even though there was no significant improvement in perception, there was a positive behavioural change towards vaccination which may later change the perception of the subject. Outreach programs like our study would play an important role in bringing down the global burden of cervical cancer. The study also implied that schools may be an effective setting to provide communication/education on HPV vaccination to adolescent girls.
Supplemental Material
sj-pdf-1-tav-10.1177_2515135521990268 – Supplemental material for Impact of indirect education on knowledge and perception on cervical cancer and its prevention among the parents of adolescent girls: an interventional school-based study
Supplemental material, sj-pdf-1-tav-10.1177_2515135521990268 for Impact of indirect education on knowledge and perception on cervical cancer and its prevention among the parents of adolescent girls: an interventional school-based study by Rony Abraham Jacob, Priya Srambical Abraham, Feba Rachel Thomas, Vytila Navya, Juny Sebastian, Mandyam Dhati Ravi and Parthasarathi Gurumurthy in Therapeutic Advances in Vaccines and Immunotherapy
Supplemental Material
sj-pdf-2-tav-10.1177_2515135521990268 – Supplemental material for Impact of indirect education on knowledge and perception on cervical cancer and its prevention among the parents of adolescent girls: an interventional school-based study
Supplemental material, sj-pdf-2-tav-10.1177_2515135521990268 for Impact of indirect education on knowledge and perception on cervical cancer and its prevention among the parents of adolescent girls: an interventional school-based study by Rony Abraham Jacob, Priya Srambical Abraham, Feba Rachel Thomas, Vytila Navya, Juny Sebastian, Mandyam Dhati Ravi and Parthasarathi Gurumurthy in Therapeutic Advances in Vaccines and Immunotherapy
Footnotes
Acknowledgements
The authors would like to thank the staff and students of the departments of pediatrics and clinical pharmacy, JSS Hospital, Mysuru for their encouragement and support. They also would like to thank the administrators of JSS College of Pharmacy, Mysuru and different schools for granting them permission and technical support to perform the study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.