
Abstract
Maputo, Mozambique’s capital city, is marked by clear socio-spatial divisions in access to sanitation services and distributions of environmental risks. Current development plans tend to reproduce these inequalities and suggest that some residents’ sanitary needs are more important than others. We contest this logic of differentiation underpinning current interventions in Maputo, revealing how the assumption of different sanitary needs has become normalized and naturalized in the urban environment. We use a genealogy of sanitation in Maputo and the former colonial city of Lourenço Marques to trace how colonial power relations worked to normatively distinguish urban spaces and the people who live in them, making some residents and places more deserving of public protection and investments than others. Drawing on Foucauldian theorizations of governmentality, we analyse colonial authorities’ sanitary plans and interventions to show how differences and separations between spaces and bodies were and are produced. Projects of drainage and land reclamation created clean, dry and sanitary habitats for the privileged white few, the existence of which simultaneously created the wet, unhealthy and muddy spaces deemed good enough for the non-white majority. Such manufactured spatial distinctions, in turn, worked to strengthen the perception of differences in cleanliness between people. These differences were consequently mobilized by the Lourenço Marques health service to further mark and legitimize racial segregation. This is how social and spatial inequalities became naturalized in the urban environment over time, culminating in the stark sanitary divides that continue to mark the contemporary city.
Introduction
In November 2017, the Maputo Metropolitan Area municipal authorities approved an ambitious new Sanitation and Drainage Master Plan. The Plan displays a distinctly uneven vision of urban development: it proposes infrastructural improvements and extensions for the emerging hotspots of luxurious urban development along the coast, while ignoring the city’s most deprived areas (MOPHRH, 2015). In response to this particular prioritization of some areas and people, a coalition of sanitation NGOs (in which the first author participated as an observer) mobilized to accuse government planners of ignoring the sanitation needs of the impoverished areas of the city. These are precisely the areas where state infrastructure has always been absent, yet it is also where most urban residents live. With only 10% of the population served by the centralized sewerage network (Rietveld et al., 2016), residents living in low-income settlements outside of the coverage of centralized sanitation infrastructure rely on their own ingenuity for meeting their sanitation needs (WSP, 2014) while they are also exposed to the highest environmental risks (Rietveld et al., 2016) because of frequent flooding caused by poor drainage.
In this paper, we take the controversies over the city’s sanitation Master Plan as our point of departure to explore the politics of sanitation in Maputo city. While the implementation of the 2017 Master Plan proceeds very slowly due to the economic crisis prevailing in the country (Conselho Municipal de Maputo (CMM), 2018) we remain concerned with the broader logic of urban development planning informing this Plan as well as other proposed sanitation interventions. The most intriguing is its differentiation between residents in terms of their sanitary needs. Hence, some spaces in the city, and the residents inhabiting them, are targeted for interventions and public investment, while others are not.
In an effort to open up and question this planning logic for societal debate, we set out to explore where the acceptance, and normalization, of different sanitary needs for different residents of Maputo comes from. We do this by showing how specific markers identifying people as un- or less deserving are socially and historically produced, and by tracing how distinct urban areas were created and naturalized as inherently dirty. We mobilize history as a means to understand the foundations of the sanitary divides of the contemporary city. Drawing on a Foucauldian framework of governmentality, we identify how sanitation was an essential tool for the operation of material and discursive relations of power, helping create and provide legitimacy for hierarchical and racialized distinctions and differences between people. We also build on urban political ecology to show how sanitary interventions also worked to re-organize socionatures, making constructed spatial orders and inequalities appear as the effect of naturally occurring differences between drier and wetter areas. Indeed, we show how the city’s uneven physical environment – containing different environmental risks and amenable to various infrastructural interventions and development imaginaries – has been produced through deeply unequal social relations (Kaika, 2005). Overall, our analysis serves the purpose of showing that the stark sanitary divides of the contemporary city result from particular historical processes and power relations.
Drawing from archival material and interviews with retired civil service staff, conducted by the first author in Lisbon and Maputo, we trace the different periods in Maputo’s sanitation history to show the sequential emergence of new problems, questions, discourses and modes of intervention. We structure the timeline and our narrative analysis according to our identification of key shifts in how sanitation operates in the exercise of power, and in how it produced the associated material, social and spatial effects of power. Thus our history spans 1887–2017, but the focus of our analysis is the longe durée of Portuguese colonial government (1887–1975). We summarize the sanitation interventions in the post-independence period to highlight the rationalities still shaping current interventions. We turn now to explain why, and how, we mobilize the framework of governmentality to analyse the relations between sanitation and power.
Sanitation, power and difference
The paper uses the theoretical framework of governmentality as a way of shedding light on the complex processes through which sanitation becomes a means through which power is exercised. We take inspiration from sanitation studies done across (western) Europe, revealing how the domain of sanitation emerged as a sphere of life to be governed and administrated. By conferring the authority to determine and assesses what and who was clean and hygienic on some privileged experts, sanitation became part of systems of governmental rule and power (Brown, 1989; Campkin and Cox, 2012; Gandy, 1999; Vigarello, 1988). Power, as defined within the framework of governmentality, is wholly relational and operates through both discursive and material practices (Li, 2007) which range from disciplinary techniques working upon individuals’ capacities and behaviours to the institution of norms for the detailed regulation of order and maintenance of a certain type of conduct (Kendall and Wickham, 1998, Scott, 1998). Using a similar analysis as the above scholars, we set out to show how the differences encoded in the current Maputo sanitation master plan are the cumulative and layered effect of a long historical sequence of contingent and sometimes contradictory rationalities of government rule. Efforts to improve sanitation in colonial Maputo encompassed and put into effect distinct practices of rule by articulating purposive elements of government (the wellbeing of populations), sovereignty (domination) and discipline (the supervision and confinement of certain groups) (Li, 2007). As this paper demonstrates, in the colonial city of Lourenço Marques (LM) sanitation rationalities overlapped with several other governmental rationalities and programs that happen(ed) in historical sequence or concurrently, sometimes exposing tensions between the will to improve and the right to rule. These tensions are played out through the always unstable, shifting and inconsistent categorizations and rankings of spaces and bodies.
Our analysis builds on and is inspired by a rich body of work – particularly by postcolonial scholars – documenting how governmentality works through sanitation. By showing how normative discourses around who and what is clean are linked to specific practices of hygienic and healthy behaviour, this work reveals how supposedly universal ideas of humanness work to protect the privileges of a few. Norms and practices about health and hygiene were and are anchored in and obtain legitimacy through scientific (often Western medical) knowledge. The assessment of people on the basis of their health and hygiene habits produced racial hierarchical rankings of subjects to (re)confirm the superiority of Europeans over local populations. Such rankings also served to subject different categories of people to differential disciplinary measures (Home, 2014; Kooy and Bakker, 2008b; McFarlane and Rutherford, 2008). In this way, colonial governmentalities proceeded in part to normalize and further entrench differences between European and colonial subjects, effectively constructing the latter as requiring both material and psychological ‘civilization’ (Arnold, 1993; Cooper and Stoler, 1989; Prakash, 1999; Stoler and Cooper, 1997). Binary identity categories – European/native, modern/primitive, civilized/uncivilized, sanitary/insalubrious, developed/backward – served as important discursive tools in these colonization and modernization efforts (Bickford‐Smith, 1995; Deacon, 1996; Goerg, 1998; Musemwa, 2008; Njoh, 2008; Swanson, 1977).
For critical studies of sanitation, governmentality is therefore an interesting theoretical lens to draw attention to how discursive techniques of power produce different subjectivities. Indeed, associations between cleanliness, civilization, health and development have always been and continue to be an important underlying moral matrix of sanitation policies and projects. Through this matrix, sanitation has brought and brings into being subjects who are differently positioned in terms of power (governors and governed) and with different sets of rights and claims. To highlight the inextricable associations between sanitation and the specifics of rule in colonial cities, Maynard Swanson (1977) speaks of the ‘sanitation syndrome’. It explains how, at the turn of the 20th century, racist ideas about Africans were reinforced by theories about the spread of infectious diseases. Events, such as the outbreak of the bubonic plague in the Cape colony where Chinese, African and Indian dockworkers were first to contract it, contributed to propagate fears and ideas that non-white populations were particularly volatile disease vectors. As a consequence, the reaction of municipal authorities was to isolate Europeans from African communities through a literal cordon sanitaire that portrayed Africans as terminally dirty and incapable of maintaining clean neighbourhoods. Thus, urban planners in South Africa started to advocate for spatial separation for different kind of colonial subjects (Miraftab, 2012; Swanson, 1977).
These analyses resonate with critical urban planning studies interested in how sanitation forms part of projects of subject- and place-making. For instance, Brownell (2014) shows how categories of citizenship map onto sanitary identities to produce spatial differences. In her analysis of Dar es Salaam, Tanzania, power relations and subject making through sanitation are productive of particular spatial divisions and sanitary infrastructural neglect. Her analysis demonstrates how colonial fears about contamination and race continued to inform measures to protect the public health of some people and urban environments in a post-independence context (Brownell, 2014). Similarly, for Indonesia, Putri (2019) uses governmentality to draw attention to how past regimes of sanitary rule co-shape the development of contemporary planning. Focusing on the peripheral spaces of kampungs, she shows how sanitary stereotypes were critical to the spatial separation of races, reinforcing cultural differences and unequal power relations: non-European and non-Chinese communities in and around the city of Jakarta were tagged as ‘undisciplined and insanitary’ settlements, ‘sources of insurgency’ and were equated with a public health menace (Putri, 2019).
Understanding the differentiation of spaces and people as a result of particular governmentalities continues to be a useful way to start making sense of the persistent uneven coverage of sanitation infrastructures and services in contemporary cities, even when colonial binaries are no longer explicitly used to legitimize these. As scholars who emphasize the materiality of social relations of power have shown, these differentiations and distinctions are importantly anchored in the lay-out and design of infrastructural systems (Kooy and Bakker, 2008a, 2008b; Nilsson, 2006). McFarlane (2008) uses the case of Bombay in India to reveal how infrastructure is far from a neutral technical means to improve sanitation conditions: the lay-out and design of sanitary infrastructural networks materialize and enact different categories of cleanliness, modernity and development, creating different sanitary spatial environments and producing huge differences between residents in terms of their access to water and sanitation services (McFarlane, 2008).
Our analysis also draws on the scholarship of political ecology, to show how relations of power are not just inscribed in and materialized through technology and infrastructure, but also become manifest through interventions in ecological and biophysical processes (Agrawal and Bauer, 2005; Gandy, 2008; Kaika, 2005). Within urban political ecology, the relationship between discourse (or knowledge) and the transformation of the environment is a key focus of scholarly attention: ‘the material production of environments is necessarily impregnated with the mobilization of particular discourses’ (Heynen et al., 2006). We draw on these theorizations of the relationships between nature and society in urban space as mutually constitutive (Gandy, 2014; Lawhon et al., 2014) to show how discourses distinguishing between civilized/uncivilized, modern/primitive, European/native are not just used to rank and govern populations, but also serve to guide and inform (and were in turn produced by) socionatural transformations. Hence, ‘unhealthy’ environments such as low-lying swampy areas were produced alongside sanitary, serviced, clean and dry modern spaces. Here we also acknowledge the foundational work within environmental justice scholarship, where the production of uneven urban geographies has always been linked to race (Pulido et al., 1996).
In the following section of this paper, we analyse how the Portuguese colonial government exercised power through sanitation in Maputo over a period of roughly 100 years: from the late 1870s up until the country’s independence in 1975. While the latter years of colonial government were less concerned with sanitation as a government problem, we consider this neglect of material conditions as itself representing a rationality of rule and a mode of governing that is productive of difference. We extend our history of the city’s sanitation into the postcolonial period (1975 onwards), to end our timeline with the construction of the city’s first centralized sewerage infrastructure between the 1980s and 1990s. Our primary focus is on the colonial city, a choice informed in part by the availability of archival material, but also stemming from the very limited attention of the postcolonial government on the material conditions of water and wastewater in the city (Rusca et al., 2018).
The history of sanitation we compose is structured according to our analytical aim of wanting to call attention to the different ways in which sanitation was used to exercise power by colonial authorities, and what this meant for the production of differences. Our categorization of distinct rationalities of rule makes them appear more clear-cut and distinguishable than they were in reality: problems, concerns and interventions in sanitation were often overlapping, partial and sometimes contradictory.
Sanitation as a domain of government: The production of an urban environment separate from ‘nature’ (1870s–1900s)
The history of sanitation in Maputo began prior to the elevation of what used to be just a military settlement to the category of a city, in 1887. Following pressure by European nations on Portugal to take a more significant role in governing the country they colonized, the administrative reclassification of the existing military garrison as a city signalled a change in the concerns of the Portuguese government (Sidaway, 1993; Sidaway and Power, 1995). The purpose of government shifted from just securing territory, to securing the welfare of the European population in place and the increase of its wealth and health (Foucault, 1991). It is therefore not a coincidence that it is in precisely this period that sanitation emerged as a concern of the Portuguese. Described as ‘a wretched, unhealthy and infected’ place, where ‘death penetrated’ from the ‘miasma of a large swamp’ (Rufino, 1929), LM’s reputation until then had been that of a ‘graveyard of white people’ (Rufino, 1929). This reputation had been earned over the previous centuries of military occupations, but it was when the government started engaging with the ‘right manner of disposing of things’ as part of its mandate that the environmental conditions of the city started being defined as unsanitary. Hence, the emergence of sanitation as a concern of the Portuguese government is a clear indication of the emergence of a distinct governmental rationality (governmentality).
Sanitation clearly appears as a distinct domain of government in the descriptions of the city of that time. Although long reputed to be ‘filthy and smelly’, the city was now labelled as unsanitary. This was problematic as it discouraged the right kind of colonial people to settle, those who could help make the city become ‘a utopia of colonial expansion’ (Noronha, 1895). The exploitation of labour and the shipping of the Transvaal mineral resources to Europe to secure the economic prosperity of the Portuguese was one of the major concerns of the colonial government. Indeed, the profitability of the colonial enterprise was directly threatened by LM’s reputation as a ‘filthy and smelly’ place, as it clashed with the sanitary desires, aspirations and beliefs of the European colonist population of that time. Its unsanitary condition thus prevented investment, development and security of the port and trading firms. After all, ‘shipping and forwarding firms were reluctant to establish staging areas, warehouses and offices in a town where unhealthful conditions added to their overhead’ (Penvenne, 1983). Becoming sanitary thus became a precondition for the colonization of LM, something that was needed to attract those individuals and companies expected to advance the commercial interests of the Portuguese colonial empire and other European economic centres (Jenkins, 2009; Penvenne, 1983).
Making the city sanitary was understood to require a re-ordering of the relationship between the emergent city and its environment. The imaginary of the sanitary city that informed re-ordering plans was shaped by the idea of disease as spreading through odorous clouds of air – miasmas. Although already largely discredited as a theory of disease transmission in Britain by 1870s (Halliday, 1999, as cited in McFarlane, 2008), it was still prevalent in the characterizations of LM of that time as a ‘swamp from which death emanated’ (see Rufino, 1929). Following the idea of miasma, the unhealthy conditions of LM were attributed to the muddy waters collecting in and around the city (Longle, 1887): it was the mixing of elements in a swamp – of air with standing water, and of soil with water – that was identified as the cause of its unsanitary state. The proposed solutions thus entailed efforts to increase the circulation of air as well as of that of currently stagnant water in the swamp. At heart, these solutions consisted of the separation of land from water. Similar to what McFarlane (2008) describes for colonial Bombay, in LM dealing with sanitation therefore meant dealing with ‘nature’. But unlike in colonial India, making the city sanitary for LM was not about integrating nature in the cleansing of a contaminated city, but about separating ‘nature’ from the city. The city had to be reclaimed from the swamps to create the clean and liveable environments that colonial investors and merchants would want for setting up homes and businesses.
Constituting sanitation as a specific domain for the administration of the relationship between the population and the environment set in motion the assembling of different agents, who were each attributed with different powers. Almost a decade prior to granting LM the category of city, a public works expedition was sent from Portugal to form a Department of Public Works in the colony, under the authority of the Minister of the Navy, Overseas and Foreign Affairs. The task of this new authority was to reorder the landscape in line with the requirements for a sanitary city: fill in the wetlands and dry the swamps, to ‘create the conditions that would produce a complete transformation in the economic and social conditions of the Portuguese overseas territories, and thereby compete to attract important national and foreign capitals, enable national emigration and ease fertile colonization’ (Costa, 1901). The works initiated to realize this continued until the end of the 19th century and included the drainage of wetlands (114 ha), the construction of a seawall to prevent tidal flooding of the drained areas and designs for the future spatial development of LM (Machado, 1879, 1881).
The operation of colonial power through the domain of sanitation by the agents and agencies charged with these projects thus physically transformed the city’s landscape, producing new socionatures by separating land from water, and by creating different elevations in the city to reroute the flows of water from drainage, rivers and rainfall. The social relations enrolled in the production of the new urban environment in LM are seen in how the business district was established by creating new land in the former marshes of the lower part of the city (Baixa), near the original military fort. The elevated areas in the eastern part of LM considered most sanitary were instead set aside for the future spatial development of an ‘aristocratic town’, a neighbourhood ‘solely for those who possessed more means of wealth’ (Longle, 1887). Situated with views over Maputo Bay, with the higher elevation ensuring exposure to sun and wind, these areas (the current neighbourhoods of Polana and Ponta Vermelha) were considered the healthiest and came to be earmarked as the most desirable for settlement by the colonial elite (Longle, 1887; Mendes, 1985).
Sanitation as a discursive technology of government: Differentiating the social
The exercise of colonial power through large sanitary works transforming LM’s environment was intimately linked to discursive relations of power for governing the colonial population. A similar binary categorization of ‘nature’ as (needing to be) separate from culture that shaped interventions to make a sanitary city was also used to define and distinguish people: the definition of sanitary and therefore civilized behaviour was to live separated from or outside of ‘nature’ – or in spaces where ‘nature’ was controlled. Through the creation of material distinctions between areas in and around LM, residents also came to be differentiated in terms of how healthy, sanitary and therefore civilized they were. Different populations were thus created through their placement in either sanitary or less sanitary environments, in the process also re-defining and confirming the distinction between colonial rulers, and those whom they ruled over.
The discursive association between sanitation and modernization, or civilization, first suggested in the public works program, and continuing throughout the 19th century, is very visible in the city’s first spatial plan of 1887. In the plan, the problem of sanitation is linked to the problem of developing a modern city for a modern population; sanitation is an intrinsic dimension of the larger project of progress and development. Although never realized, the plan pro-actively imagines a sanitary environment as consisting of formal, planned and regular spaces; spaces in which ‘nature’ is controlled. Roads were to be widened and straightened, while gardens and public squares were to be made more beautiful through a regulation and ordering of the ‘natural’ environment. An advocate of the plan describes its intended effort in this way: ‘LM will soon be the most regular city in South Africa and one of the best designed anywhere in the world’ (Noronha, 1895). The definition of sanitation evident in the plan once again clearly entails the distinct demarcation of the city from its ‘natural’ environment.
The spatial separations between sanitary and unsanitary spaces supported distinctions between colonial populations, each of which partly performed its (level of) civilization through distinct sanitary practices and habits. These in turn mapped onto existing socio-cultural hierarchies to become important markers of race and class. In the late 19th century, using sanitary practices as a basis for racial and class classifications was still far from straightforward. First, the sanitary and civilized population of colonial rulers needed to be brought into being. This is recorded in the sanitation study of 1891, led by engineers of the second public works expedition from Portugal, in which the behaviours of the city’s population were classified and problematized: The bath and kitchen waters are thrown on the ground near the dwellings, where they disappear by infiltration or by evaporation. The night soil, according to a determination of the city chamber, should be taken to the barge that leads them to the bay and is thrown into the water. Since, however, the barge is far from the dwellings, all people try to avoid as much as possible this service, to which the natives have great repugnance. It follows that a part of the population, Moors, Banyans and Indigenous servants, who constitute the largest number of inhabitants, they leave their houses, where they do not have toilets and go to the beach and the marsh improvising outdoors. Another part of the population establishes the system of fixed pits and dig holes in the ground, but they abandon them as soon as they are full. (Soeiro, 1893)
1
The findings of the sanitation report 2 led to the establishment of the overseas health service (1895), a new administrative authority in the colony under the Secretary of State of Navy and Overseas Affairs. This authority was established to reduce the high rate of mortality among the European civilian population and the colonial military forces by improving their hygiene conditions (Pereira, 2001). As documented in the monthly reports from the LM health service to Portugal, one of the first priorities of the health service was to improve water supply for those people earmarked to become the modernized, civilized European subjects of the colony (Azevedo, 1895). Health officers identified the collection and storage of rain- and river water, along with the use of water from the wetlands in low-lying areas, as unhygienic, agreeing with the earlier Sanitation Study on the role of water in spreading infectious diseases (Azevedo, 1895, 1901). What made water unhygienic was defined in terms of the presence of microbes, but also still relied on what could be perceived through the senses. Hence, turbidity, cloudiness and sediments in the water – i.e. mud and soil mixed with water – continued to be considered as problematic in the emerging sanitary discourse. Water ‘poisoned with the foreign matter’ was thought to be conducive to the development of microbes (Barreiros, 1897; Pacheco, 1947).
The health service chastised public works engineers for the neglect of the city’s water infrastructure: ‘The sanitary errors begin in the water lifting machine’ where ‘the water flows to the first reservoir in a small open ditch carrying some mud’ (Barreiros, 1897). Yet, plans for the city’s water supply system had already been drafted in 1892 (Soeiro, 1893). These plans envisioned the provision of 3000 m3 water for 2285 Europeans residents through a centralized distribution network supplied by two reservoirs. The upper zone (Zona Alta) on the slope was to be supplied by the reservoir of Maxaquene, whereas the lower zone (Baixa) was to be supplied by the reservoir of the Paiol. Engineers recommended water to be provided twice a day to all neighbourhoods, with the exception of the indigenous neighbourhoods, where providing it once a day was deemed sufficient (Soeiro, 1893). This plan was implemented by the Delagoa Bay development company, which held the concession for water supply in LM for the next 50 years (1895–1945). The calculation of different water needs according to racial categories continued over the following decades, visible in the frequent complaints made by the black elite and assimilated mestizos about the water restrictions in their urban neighbourhoods and the complete absence of state water supply in neighbourhoods occupied by the indigenous black people (Alburquerque, 1959).
Separating the social: Normalizing racial categories through sanitary classifications
At the beginning of the 20th century, the operation of power by colonial administrators through sanitation to govern the colonial population shifted in its application. In the previous 25 years, the purpose of colonial government had been to secure the health of European civilian residents and the colonial civil servants, bringing into being a civilized and modern population of colonial rulers to inhabit the sanitary spaces in the city. Now, at the turn of the century, the sanitary rationality shifted by marking and contrasting these people and places with others in the colony. Sanitation remained central in producing differences between populations – differences between rulers and ruled, and between more and less clean or healthy and hygienic people – in ways that supported and normalized European superiority, and legitimized the continued exercise of military force to ensure its control over land and labour (Zamparoni, 2000). Differences in sanitary practices that were partly produced through differences in access to water and sanitation services helped bring into being and normalize racial categories. Attitudes towards health, as well as practices around cleanliness of the body and the home became further entrenched as markers of racial distinction. Of course, colonial rulers were at the top of the hierarchy: their sanitary behaviours marked them as both European and civilized; ‘the degree of civilization of a nation is measured by the perfection of its hygiene’ (Pacheco, 1947) remarked one Portuguese colonial historian, while other racial groups were identified as responsible for contaminating the city and making the city unsanitary.
The categorization of individuals into different population groups according to their hygiene practices had already begun in the previous century: the first Sanitation study in 1887 already attributed unhygienic practices to particular races. This use of sanitation for racial classification continued in the first decade of the 20th century: the sanitation studies and health reports of the colonial government created and then problematized four racial groups that were distinguished on the basis of differences in hygiene and sanitation practices. First, there was the Asian population from British India, brought to the colony as labour. They were portrayed as filthy and messy people, and were described in colonial reports as a danger to hygiene and public health (Zamparoni, 2000). The health report of 1895 to Lisbon stated for instance that ‘the internal hygiene of the houses in the city was generally satisfactory, with the exception of the dwellings of Indian people, namely, Banyans and Moors which do not follow to the most rudimentary precepts of hygienic’ (Azevedo, 1895). The unsanitary status of Asians was seen as inherent to their race, naturalizing both the racial category and their place in the social hierarchy. Asian customs, religion and ways of life were identified as responsible for their inability to adopt the ‘regular conduct of cleanliness’ and living in the midst of filth was seen as a hereditary tendency of their race (Azevedo, 1895).
The second racial category were the Chinese, who supplied the city with fresh vegetables, then – as now – grown in the area surrounding the city, 3 and in the Maxaquene swamps. Hygiene practices of the Chinese were routinely problematized in health reports, as they were suspected of using human waste as fertilizer, relying on the night soil from the nearby compounds of black labourers. These practices were identified as inherently Chinese, which is why they were blamed for the regular outbreaks of typhoid, dysentery and other infectious diseases (Oliveira, 1909). The third racial category brought into being through sanitation occupied the lowest place in the hierarchy of development and civilization. This was also based, in part, on the sanitary practices of the people in this category. The group consisted of black native and indigenous people, who – not coincidentally –constituted the most important labour source for the colony (Zamparoni, 1998). The increasing importance of controlling this labour for the colonial project coincided with the increased use of sanitary discourses to establish their racial category and place in the colonial hierarchy. Other scholars have identified how for the colony ‘the whole matter of civilization comes down to a question of labour’, in so far as the ‘acquiring, distributing and overseeing cheap unskilled black labour was already a principal concern for the colonial state and the local bourgeoisie by the 1890s’ (Penvenne, 1989a). In the sanitary study of 1891, black people were problematized as open defecators, threatening the public health and the communal hygiene of the city. Black residents continued to be associated with unhygienic practices of defecating on the beaches and in the wetlands around the city, disobeying the new municipal health regulations ordering residents to collect and deposit night soil in particular places of the city (Soeiro, 1893).
A fourth category concerned the European or white population, whose sanitary practices go unmentioned in the sanitation reports of the 20th century, a notable change from the Sanitation study of the Health Service in the 1890s. The very absence of any description of sanitary practices suggests that the behaviour of Europeans figured as the civilizing norm in terms of sanitation. If hygiene practices of this population group fell short of expectations, this was not interpreted as stemming from inherent cultural habits, but was instead attributed to the unaffordability of good housing (Azevedo, 1901). This contradiction in the rationality of colonial rule did not go unnoticed by some LM residents. Newspapers in the first decade of 20th-century record objections of the black elite population to sanitary logics. Commenting on the lack of toilets for black labourers working in the harbour, writers to the newspaper argued open defecation did not indicate the uncivilized, racialized, subject, but was rather the result of an absence of infrastructure and services. They recommended that instead of policing the use of the beach by the indigenous people, the administration should construct toilets (Africano, 1911). This commentary by black residents reveals both resistance to and limitations of colonial authority; discursive relations of power exercised by the colonial health services and administrators were not wholly successful in getting black residents to internalize an identity as inherently uncivilized and unhygienic.
These limitations of colonial authority in generating new technologies of self by colonial populations were partly addressed by the Policy of Assimilation (1904–1961). This Policy made clear links between sanitary practices and levels of civilization. According the rights and privileges of citizenship on the basis of one’s civilized practices motivated some of the elite black residents to internalize these categorizations. Under this policy, Africans and other non-white people were divided into two categories: indigenous (indigenas) and assimilated (assimilados). Holding the status of assimilated was significant, as it granted individuals the same legal rights as Portuguese citizens (Penvenne, 1989a), but attaining this status depended on one’s ability to adopt attitudes and practices culturally coded as European, ergo civilized. This status was formally indicated by one’s level of education, adoption of the Catholic religion, and monogamy, but the classification of people by colonial authorities also required the daily performance of a range of cultural habits, of which hygiene – with food, one’s home, one’s body – constituted an important part (Lachartre, 2000; Sidaway and Power, 1995).
Like in other colonies at the turn of the century, the development and advancement of colonial subjects (assimilados) revealed contradictions in the racialized logic of colonial authority (Wilder, 2003). For LM, the colonial government’s allowance for individuals to change their classification, becoming civilized/European, also raised the possibility that race, and the hierarchy within which races stood, was not fixed, not biological, but something that was socially constructed, through the exercise of power. This in turn, made it potentially possible for the entire population of black labour on which the colonial enterprise rested to demand citizenship rights. Coinciding with the increasing questioning of the colonial project across Europe at the turn of the century (Domingos, 2013; Lachartre, 2000), the threat of race’s social construction to colonial authority coincided with the adoption of new means of governing. The social differentiation of the population by racial categories now became the basis of increasing spatial segregation, achieved through new technologies of zoning, planning and infrastructure.
Socio-spatial segregation: cement city, suburbs and reed city (1907–1940s)
After the turn of the century, a wave of public health concerns about the spread of infectious disease in the colony heightened anxieties of European colonial authorities over keeping ‘black bodies’ in place – both in the racial hierarchy, but also by policing their actual physical occupation and movements in and out of the city. This is how threats of contamination were racialized. The colonial authorities exercised power through new technologies of zoning, planning and infrastructure to fix the segregation of racial groups in and out of the city. Measures put in place by the colonial government to manage the outbreak of the bubonic plague in 1907 mark the introduction of these new techniques. Although the spread of infectious diseases – cholera, dysentery, typhoid – had been a concern of the health service since its inauguration in 1895 (Roque, 2016), it was only now that particular spaces in the city became classified as either sanitary or unclean. Unsurprisingly, the spatial classification of unsanitary zones corresponded with the classification of the populations who inhabited these areas, who had already been identified as diseased and unhealthy through their racial categorization. The downtown business district zone, with a high concentration of stores and warehouses, was described in the colonial health report of 1909 (Oliveira, 1909) as being in poor sanitary condition and inhabited by ‘filthy Asian people’. The central area of the city, with houses made of wood and zinc, was considered unfit for habitation and a menace to public health; residents in this area were ‘blacks and Chinese of low social scale’ (Oliveira, 1909). The lower areas of the city on the periphery of the centre, the Mahé and Malanga neighbourhoods housing black labourers were also seen as unhealthy (Oliveira, 1909). In contrast, the areas inhabited by colonial elites (Polana and Ponta Vermelha) were defined by their cleanliness, their good health, and their generally clean and exemplary dwellings (Oliveira, 1909).
Following the differentiation of spaces according to levels of sanitation, different regulations for managing public health in each of these spaces were applied by the colonial government. In the efforts of the public health service to deal with the plague, dwellings of black and Asian residents, identified as unsanitary, were demolished, and the residents were not allowed to rebuild in the city centre. The sanitation police disinfected spaces by burning the contents of these houses and fencing off vacant plots of land; they also established new regulations for cleanliness of the physical environment (solid waste), and behaviours (how many people could sleep in one room) (Oliveira, 1909).
Efforts of the colonial government to control what were classified as contaminated indigenous bodies in the city were supported by a system of increased surveillance, and by regulations to control the movement of different populations. The policy on ‘Indigenous Servants and Workers in the District of Lourenço Marques’, applied between 1904 and 1961, regulated the movement and presence of indigenous people within the city. Residents classified as ‘native’ required a pass, issued by the administrators of the districts, to enter and move through the city (Zamparoni, 1998). Without such a pass they could be subjected to physical punishment or fined. Here we see colonial authority exercising different modes of power on the colonial population: there is disciplinary power, governmental power, and biopower – regulating the sanitary conditions of life for different social groups by subjecting their bodies to precise controls and comprehensive regulations.
As in other African colonial cities at the turn of the century, the distinctions made between urban spaces and populations through sanitation legitimized efforts to create stricter socio-spatial demarcations (Brownell, 2014; Swanson, 1977). In LM, from 1907 to 1909, the separation between the city (Cidade) and suburbs (Subúrbios) as zones for European versus indigenous people was enacted through administrative measures to improve the health of the city. Indigenous residents who had their homes destroyed by the sanitary police were relocated outside the city (Oliveira, 1909), and following a 1907 sanitary regulation banning most indigenous residents from housing in the city there was a proposal to create distinctly indigenous neighbourhoods (Bairros Indígenas) in the periphery (Roque, 2016) cut off from the city by a ring road (Estrada da Circunvalação) (Simão Gonçalves, 2016). Providing a border around the European city, the ring road effectuated a clear socio-spatial demarcation between the ‘Cement city’ and the ‘Reed city’ (Penvenne, 1989b). This demarcation was prompted by the recommendations of an LM Health Service report on the problem of indigenous housing, prepared in June of 1909. This report repeated the identification of black natives, Chinese and Indians settlements as unsanitary, and then recommended that: ‘It would be a great convenience for the hygiene of Lourenço Marques that in the suburbs of the city a convenient place was chosen for the establishment of one settlement for Indigenous and another for Asians’ (Simão Gonçalves, 2016). 4
The colonial government’s response to the epidemic was thus to segregate racial groups and urban spaces. Separating the city from the non-city and dividing these spaces between European and others, also seemed to mean the colonial government could concentrate its scarce resources for infrastructure and public health on European residents, isolating them from populations who had to continue living without access to clean water or sanitation services. In 1918, the first indigenous neighbourhood Bairro Indígena do Xipamanine lacked water, light, adequate sanitation – with only one cesspool for a 100 residents (Vales, 2014). A second neighbourhood was built in 1940 for the emerging indigenous elite (Bairro Indígena da Munhuana), exposed residents to malaria and other waterborne diseases, as flood water regularly drained from the cement city to indigenous neighbourhoods, where water collected because of the topographical conditions and lack of drainage infrastructure (Penvenne, 2015).
Socio-spatial segregation and sanitation infrastructure (1950s–1970s)
In the period between the late 1940s and 1970s, the city’s socio-spatial segregation predicated on racialized sanitary discourses, continued to inform where, and for whom, the colonial government would allocate scarce resources for sanitation infrastructure. Up until this era, the physical sanitary interventions in the city consisted of drainage and infill works, leaving residents of the Cement city to build their own septic tanks. In the 1930s, the municipal government issued a decree forcing owners of buildings in the Cement city to install septic tanks, which were eventually to be connected to the networked drainage system. But although European residents had pushed colonial authorities for the installation of sewerage already in the 1920s, the municipality still delayed the construction, attributing this to financial shortfalls (Africano, 1929; Notícias, 1929a, 1929b).
By the 1950s, with still no sewerage system installed, the city’s sanitary conditions were problematized by urban authorities for failing to meet with prevailing modern urban aesthetics required for the consolidation of the ‘Estado Novo’ (Rusca et al., 2018). This time, sanitation concerns stemmed from a desire to attract new flows of money and investment through tourism, as white tourism from Southern Africa and Europe had significantly increased (Penvenne, 2015). Now, sanitation infrastructure became framed as an important tool to enable aesthetic modernization and improve the tourism value of the city. Septic tanks were increasingly considered unacceptable, since many of them were broken, or overflowing into open drains (Aguiar, 1955). More than just being a health risk, this was considered unsightly. Alongside health concerns of untreated wastewater, the drainage of stormwater also was an important priority, as regular flooding impeded economic activities in the downtown business district (Aguiar, 1955).
Throughout this period, the municipal council drew up several master plans for sanitation: the General Sanitation Project (1955), the General Sanitation Scheme (1961) and the General Sanitation Plan (1968). None of these were ever executed, at least not immediately, again due to a lack of funding (Almeida, 1968), although electricity and water services were prioritized (Rusca et al., 2018). Municipal authorities then – as now – sequenced the implementation of sanitation improvements, prioritizing drainage improvements and an underground sewerage network in the elite residential areas and the business district. The rest of the city continued to rely on septic tanks, although they were promised future incremental extensions of sewerage lines. Such extensions were partially achieved, but remained limited to the so-called xilungwine (White city) (Almeida, 1968).
Post-independence sanitation (1975s–1990s)
In the socialist government following Mozambique’s independence (1975) the city of LM was identified as a symbol of the injustices of colonial rule, the site of racial discrimination and the capitalist exploitation of the labour of the colonized population (Sidaway and Power, 1995). There were few sanitation interventions in Maputo until the 1980s, despite dire living conditions of residents (Forjaz et al., 2006; Pinsky, 1982). While some residents took over the abandoned, and nationalized, housing stock of European colonial areas, and benefitted from sanitation infrastructure in these areas (Roque et al., 2016), the vast majority were expected to provide for themselves, building their own latrines and landfills (RPM, 1979). A National Sanitation Programme of Low-Cost Sanitation was minimally successful in enabling access to sanitation from 1985 to 1990, but suffered from abrupt policy changes later in 1990s, dependence on external funds and disruptions in the supply of feedstocks (Colin, 2002; Forjaz et al., 2006).
The sanitation interventions which were carried out did little to redress the existing socio-spatial inequalities in access to sanitation, or challenge the logic rendering some residents more deserving than others. The city’s current wastewater treatment plant was built in 1986, but it only served those areas of the city that were already connected to the sewerage network, making only small extensions of the network to spatially proximate areas (Alburquerque, 1986; RPM, 1984). Low-income settlements continued to be neglected, with the exceptions of Malhangalene and adjacent parts of Alto Maé, Coop, and Central neighbourhoods (RPM, 1984). Despite the inclusion of subúrbios within the city administration, the postcolonial authorities remained primarily concerned with the former colonial spaces of the cement city, ‘replacing a racially-based stratification system with one based on proximity of power and patronage controlled by the party’ (Grest, 1995). Little public investment was made in sanitation, despite the efforts of the socialist independence government (1975–1990) and attention to education and health care. Access to adequate, safe sanitation continues to be determined by the socio-spatial divisions put in place during colonial rule; the majority of Maputo’s residents live outside the cement city, where sanitary needs are the greatest. The legacy we identify as even more concerning is how citizens living in these spaces are – once again – seen as socially different, having different rights and claims for their sanitary needs.
Conclusion: The power of sanitation
We presented the history of sanitation in colonial Maputo as a history of producing differences and distinctions in bodies, spaces and environments. Through a genealogy that traces sanitary interventions and plans from Maputo’s origins as a colonial outpost (1870) to the present day, we have documented the ways in which today’s sanitary divides are the product of historical processes and power relations. We did this to show how the contemporary city’s uneven sanitary environments are not the ‘natural’ qualities of the urban form. They have historical foundations and are the outcome of the mobilization of discursive and material techniques used to distinguish areas and people and thereby making some residents more deserving of public support and protection than others.
In Maputo, what makes these processes so deeply entrenched and inextricable is that the production of nature/city happened alongside the production of bodies/races: the separation of bodies reinforced and mapped onto the separation of spaces. Because of this, these separations and hierarchies have become so naturalized in the urban environment that it becomes easy to either overlook them or to simply accept them as givens, as for instance happens in the current strategic planning aimed at improving and re-developing urban sanitation infrastructures. Through explaining how these distinctions were created, and legitimized, through the imbrication of these two sets of binaries, our history of sanitation in Maputo contributes to analyses of governmentality and urban planning. Specifically, our analysis broadens Foucault’s conception of governmentality as presumably happening within a fixed territory, whose ‘natural’ properties were also taken as self-evident. Drawing from UPE’s concept of socionature we show how situated discourses and material practices gave shape and substance to particular types of sanitary rationalities, which intertwined with the transformation of biophysical environments, spatial relationships and racialized projects. Draining wetlands, separating land from water and then relocating the African residents to more ‘natural’ and risky environments (marshlands, the breeding grounds for disease), while making the white city clean and orderly changed produced territory, including its ‘natural’ or biophysical properties.
Sadly, the 2017 master plan takes these historically produced socio-spatial demarcations as the foundation on which to plan contemporary sanitation investment and determine priorities. These plans designate low-income residents to environmentally risky areas, without sanitation infrastructures or services. While planners may not explicitly see low-income resident as ‘less than’ the residents in other areas of the city, they take the existing differences as seemingly ‘natural’, and therefore a-political, and not justifying societal intervention. Rather, technical criteria of proximity to centralized infrastructure, topography, cost recovery and land use planning are used to assess the feasibility of sanitary interventions. This policy approach continues to privilege those spaces in the city, and the residents who live in them, already designated as sanitary, versus the unimproved and low-lying neighbourhoods in which the majority of the city’s residents live without access to state infrastructure or services.
Neighbourhoods of colonial Maputo and their sanitary status.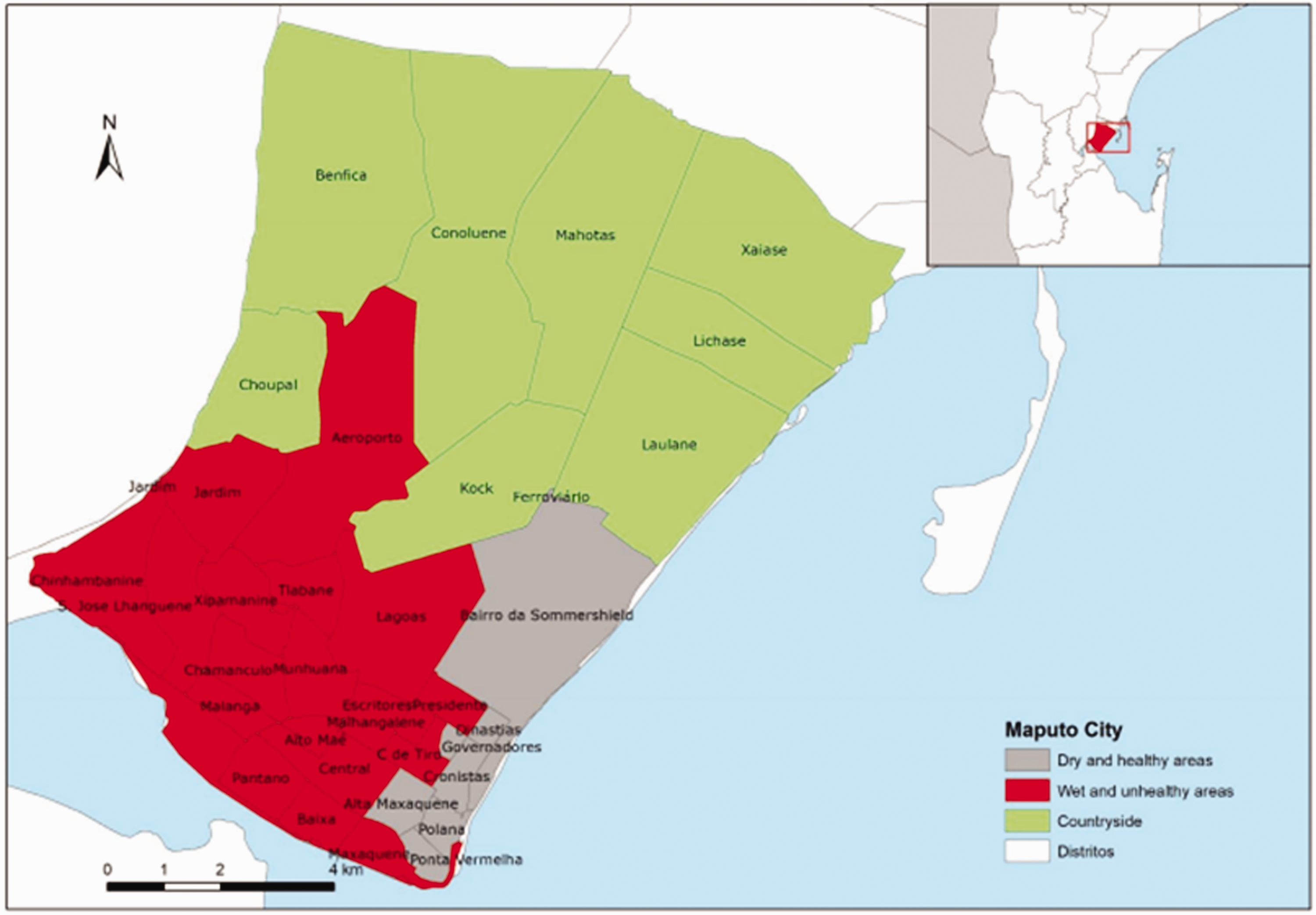
Highlights
Contemporary sanitary inequalities in Maputo city were historically produced and are the product of power relations. In colonial Maputo, sanitation was a technology of colonial rule to enable social classifications, hierarchies and socio-spatial differentiation. Differences between people and spaces in terms of cleanliness and hygiene were mapped upon and used to produce a deeply racialized society. Contemporary sanitary masterplans overlook historical differences to propose improvements for some urban spaces and segments of populations while neglecting others.
Footnotes
Acknowledgements
The authors would like to thank the staff working in Sociedade de Geografia de Lisboa and Arquivo Histórico Ultramarino, and Arquivo Histórico de Moçambique, for their invaluable assistance. Special thanks to Aníbal Chauque for his assistance during the archive research in Maputo. Our gratitude also goes to the Academy for African Urban Diversity (AAUD) team, 2017 and 2018 cohorts for their contributions. Finally, we thank the anonymous reviewers of this journal for their insightful and constructive remarks that have helped to further improve the content of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research on which this article is based was funded by the Netherlands Organisation for Scientific Research (NWO) under the project ‘Sustainable freshwater supply in urbanizing Maputo, Mozambique’ (W 07.69.109) from 1 February 2014 to 15 May 2021.