
Abstract
In acute ischemic stroke, intravenous thrombolysis (IVT) and acute endovascular therapy (EVT) have been shown to reduce long-term disability in randomized trials. International guidelines are partially not up to date and may not address situations for which there is limited scientific evidence. The goals of the present guidelines are to summarize the current scientific data for acute revascularization treatments to make sure that all Swiss Centers apply a similar, evidence, or consensus-based treatment standard. A multidisciplinary working group of the Swiss Stroke Society (SSS) searched and reviewed the literature on new randomized controlled trials (RCTs), large case series, meta-analyses, and other guidelines since the previous recommendations in 2009 to elaborate the consensus guidelines. The new RCTs have confirmed the effectiveness of IVT in various populations up to 4.5 h and proven the benefit of acute EVT up to approximately 8 h. For patients with unknown onset (including wake-up stroke), IVT and EVT can be effective up to 24 h after last proof of good health if patients are selected with advanced neuroimaging. Multiple case series and meta-analyses allow narrowing down the indications and relative and absolute contraindications to optimize the benefit–risk ratio of acute revascularization.
Background and methods
Randomized controlled trials (RCTs) have shown long-term benefit for acute acetylsalicylic acid, intravenous thrombolysis (IVT), acute endovascular therapy (EVT), neurorehabilitation, and decompressive craniectomy in selected ischemic stroke patients if they are treated in Stroke Units or Stroke Centers. Most of these treatments can be used in combination.
Treatment in Stroke Units and Stroke Centers is effective for all stroke patients, but IVT can only be offered to approximately 20–30% and EVT to 10–20% of patients arriving at the hospital within 24 h. 1 This restricted treatment rate for acute revascularization stems from the need to select patients with specific clinical and radiological criteria to obtain the treatment benefit.
The multidisciplinary working group “Acute Stroke Treatment” of the Swiss Stroke Society (SSS) has now updated the previous guidelines from 2009 2 in face-to-face reunions and by email. Representatives of the Swiss Neurological Society, the Swiss Society of Neuroradiology, the Swiss Society of Neurosurgery, the Swiss Society for Anesthesiology and Intensive Care, and the Swiss Society of Intensive Care Medicine participated actively in their elaboration. The working group performed a literature review in Pubmed/MEDLINE (2008–2020) for the combination of “stroke” and “randomised” or “meta-analysis” with any one of the following: “thrombolysis,” “thrombectomy,” “endovascular treatment,” “endovascular therapy,” and “anesthesia.” In addition to retrieved phase III studies, we also considered large case series combining the latter five search terms with “minor stroke,” “pediatric,” “preexisting disability,” “pregnancy,” “mismatch,” “antithrombotics,” “anticoagulation,” “platelet inhibitor,” “blood pressure,” “hemorrhage,” “bleeding,” and “craniectomy.” Retrieved articles and other national and international guidelines were also scanned to identify further case series, in particular dealing with conditions potentially including the bleeding risk with IVT. The working group then reviewed these new publications to develop the consensus guidelines. The strength of our recommendations was expressed by the wording rather than a classification system.
Since 2014, the SSS maintains the Swiss Stroke Registry 3 for quality improvement and research purposes. The registry follows international recommendations for quality control of acute revascularization treatments. 4
The goals of the present guidelines are to summarize the current scientific data for acute revascularization treatments in acute ischemic stroke. This should allow all Swiss Stroke Centers to apply a similar, evidence or consensus-based treatment to optimize the benefit–risk ratio for such patients. The author affiliations and potential conflicts of interest are listed in Appendix I, Table IA.
New scientific data
Since the third Swiss guidelines for acute treatment of ischemic stroke in 2009, 2 RCTs have
– confirmed the effectiveness of IVT with recombinant tissue plasminogen activator (rtPA) (alteplase, Actilyse®) within the 4.5 h window (up to 5 h in the meta-analysis) 5 ; Patients over 85 years, with small vessel strokes, and patients with minor disabling and severe strokes seem to have similar benefit as all other patients 6 ;
– shown the effectiveness of EVT, in particular with stent retrievers 7 –13 and/or aspiration techniques, 14,15 in combination with IVT up to about 8 h after stroke onset 16 ;
– confirmed the major prognostic importance of rapid treatment for both IVT and EVT (“time is brain”) 5,17 ;
– shown the effectiveness of direct EVT for unknown onset or late-arriving patients between 6 h and 24 h in the presence of certain neuroradiological selection criteria (computed tomography (CT)- or magnetic resonance (MR)-based perfusion imaging or a combination of clinical deficit and radiological core measures) 18,19 ;
– shown the effectiveness of direct IVT for unknown onset or late-arriving patients beyond 4.5 h since last proof of good health if certain neuroradiological selection criteria are present (CT- or MR-based perfusion imaging 20–22 or fluid-attenuated inversion recovery diffusion-weighted imaging (FLAIR-DWI) mismatch on magnetic resonance imaging (MRI)) 23 ;
– not shown the equivalence of low-dose IVT (with rtPA 0.6 mg/kg) with the usual dose (0.9 mg/kg), despite reduced bleeding risk with the lower dose 24 ;
– shown the probable ineffectiveness of IVT for patients with nondisabling stroke 25 ;
– shown the ineffectiveness of ultrasound-assisted IVT 26 ;
– shown the probable superiority of IVT with tenecteplase (Metalyse®) 0.25 mg/kg over rtPA 0.9 mg/kg before EVT 27,28 ;
– shown the ineffectiveness of EVT within 8 h for basilar artery occlusion in two RCT. 29,30 A secondary on-treatment analysis of one of these studies showed potential effectiveness, 29 whereas the analysis of patients with the National Institutes of Health Stroke Scale (NIHSS) >10 showed potential effectiveness in the other 30 ;
– shown noninferiority of IVT preceding the EVT in patients with proximal intracranial occlusions in two studies 31,32 but not in another 33 ;
– shown that short general anesthesia during EVT was not harmful 34 –36 and potentially even beneficial. 37
Furthermore, several international societies have updated their recommendations for treatment of acute ischemic stroke, 38 –42 and rtPA for ischemic stroke treatment was accepted by the World Health Organization in their 21st List of Essential Medicines. 43,44
Ongoing RCTs
Current RCTs are investigating the effectiveness of
– early EVT in patients with a minor neurological deficit (IN EXTREMIS) or with a large core (TENSION and IN EXTREMIS);
– EVT with or without preceding IVT (SWIFT-DIRECT, MR-CLEAN-no-IV, and DIRECT-SAFE);
– acetylsalicylic acid before/during early EVT (MR-CLEAN-MED);
– EVT based on simple CT-based selection criteria for unknown onset or late-arriving patients of up to 24 h (MR-CLEAN-LATE);
– IVT within 4.5 h after awakening with stroke based on simple CT-based selection criteria (TWIST) 45 ;
– IVT with tenecteplase (Metalyse®) 46 –48 compared to rtPA;
– general anesthesia compared to conscious sedation during EVT (COMET, GASS, AMETIS, and CANVAS).
Efficacy and complications of revascularization treatment
IVT within 3 h reduced long-term disability and death in about one in four patients and within 4.5 h in about one in six. 49 Early IVT avoids completely long-term disability and death in about 1 out of 10 stroke patients. 5,6 The risk of symptomatic intracranial bleeding as defined by the Safe Implementation of Thrombolysis in Stroke-Monitoring Study definition 50 of 3–4% is already included in these long-term benefits.
After IVT, long-term mortality is neither increased nor decreased, despite an initial elevated risk of death. 5,6 Orolingual edema after IVT with rtPA occurs in 1–3% of patients, particularly if pretreated with angiotensin-converting enzyme inhibitors and with insular infarct localization. 51 Despite a mostly benign course, this situation provoked by a local release of bradykinin may require immediate intensive care measures. It is unknown whether treatment by bradykinin-receptor antagonists such as Icatibant (Firazyr®) reduces the need for intensive care measures.
EVT within 6 h reduces the long-term disability in one out of two treated patients and completely avoids disability in one out of four patients. 16,17 There is no increase in hemorrhage or early mortality, and long-term mortality is probably decreased. 16
General recommendations
Given its narrow therapeutic window, we recommend that IVT be given in hospitals equipped with Stroke Units or Stroke Centers certified according to Swiss recommendations. 52 Similarly, we recommend that EVT is performed only by Stroke Centers mandated by the Inter-cantonal Agreement on Highly Specialized Medicine, 53 which fulfill the Swiss certification criteria. 52,54 In remote hospitals without a Stroke Unit, IVT may be offered in direct collaboration with a Stroke Unit or Stroke Center (e.g. via telemedicine) and should be documented in the national stroke registry for quality control. 3
IVT based on simple neuroradiological criteria is effective within at least 4.5 h (in the meta-analysis up to about 5 h) after symptom onset 5,55 –57 and EVT up to about 8 h. 17 Thereafter, patients need to be selected by specific neuroradiological criteria (see details below). Figure 1 shows the indications for different types of revascularization treatments in acute ischemic stroke, depending on delays and neuroradiological criteria.

Overview of basic indications for revascularization treatment in acute stroke, considering time from onset (or last time of good health) and neuroradiological criteria. Stroke onset is defined as the last time free of stroke symptoms. See text and tables for further details. *In meta-analyses: IVT up to 5 h, 5 EVT up to 7.3 h. 17 ^Unknown stroke onset and neuroradiological mismatch: up to 9 h after the mid-time between symptom-free and stroke discovery. 58 °Unknown stroke onset and FLAIR/DWI-mismatch (MRI): IVT without upper time limit. 23 IVT: intravenous thrombolysis; EVT: endovascular therapy; FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging; MRI: magnetic resonance imaging.
Based on current scientific data, we recommend IVT within 4.5 h than EVT (bridging therapy) for proximal intracranial occlusions unless there are IVT contraindications as mentioned above. Several RCTs are currently studying this recommendation.
The effectiveness of both revascularization methods decreases minute-by-minute with increasing time from symptoms onset. 5,17 For this reason, we recommend speedy interventions for treatable patients, independently of prehospital delays. To shorten treatment delays, we recommend
– standardized prehospital and transfer protocols aiming at defining and shortening triage and transport delays (see the simultaneously published guidelines on this topic) 59 ;
– standardized management protocols in all emergency departments of hospitals with Stroke Units and Stroke Centers offering IVT and EVT, integrating neuroradiology and urgent laboratory assessment;
– to initiate IVT in the diagnostic imaging facility while applying clinical and vital sign surveillance.
We recommend that the choice of the revascularization method for a given situation should be based on all available clinical, neuroradiological, and laboratory data while trying to avoid additional delay.
Specific recommendations
Indications and contraindications for IVT and EVT are listed in Tables 2–9. We recommend performing an individualized benefit-risk estimation in the presence of relative contraindications (Table 8); such contraindications can also be regarded as additional outcome modulators.
Mismatch definitions as used in RCTs.
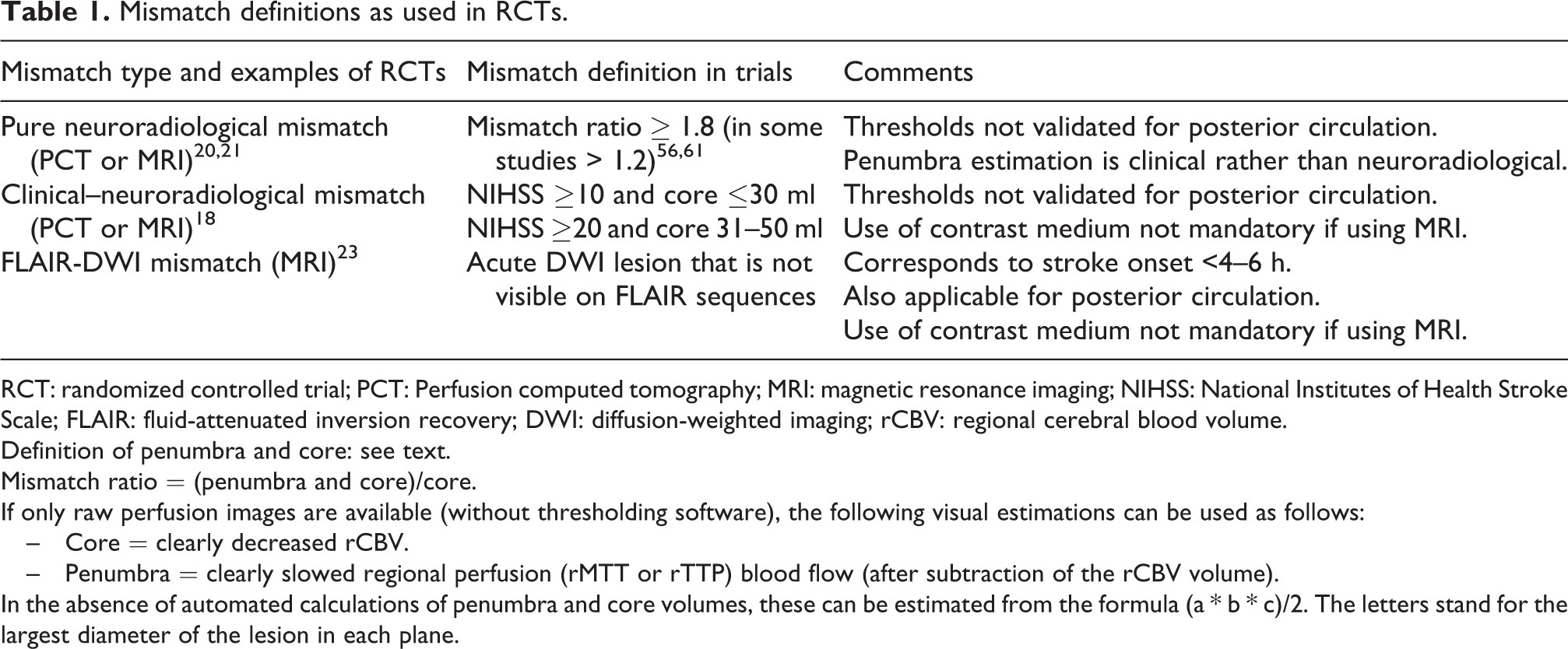
RCT: randomized controlled trial; PCT: Perfusion computed tomography; MRI: magnetic resonance imaging; NIHSS: National Institutes of Health Stroke Scale; FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging; rCBV: regional cerebral blood volume.
Definition of penumbra and core: see text.
Mismatch ratio = (penumbra and core)/core.
If only raw perfusion images are available (without thresholding software), the following visual estimations can be used as follows:
– Core = clearly decreased rCBV.
– Penumbra = clearly slowed regional perfusion (rMTT or rTTP) blood flow (after subtraction of the rCBV volume).
In the absence of automated calculations of penumbra and core volumes, these can be estimated from the formula (a * b * c)/2. The letters stand for the largest diameter of the lesion in each plane.
General indications and exclusion criteria for acute revascularization by IVT and/or EVT.
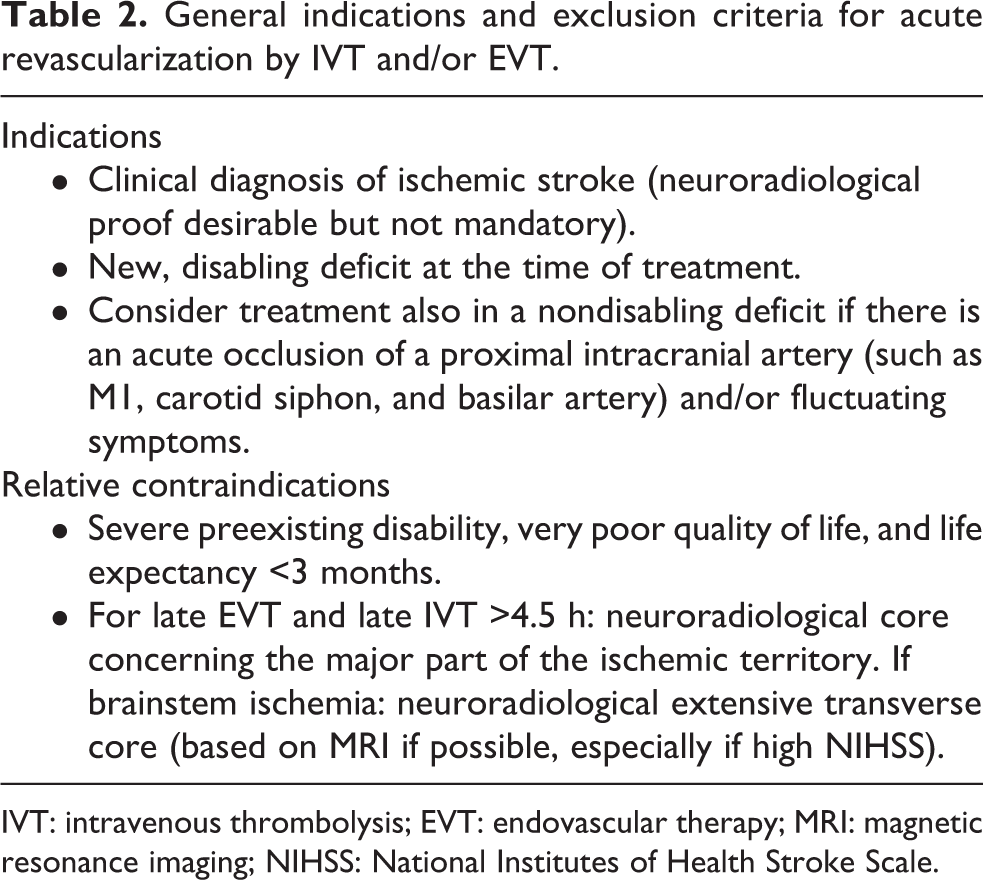
IVT: intravenous thrombolysis; EVT: endovascular therapy; MRI: magnetic resonance imaging; NIHSS: National Institutes of Health Stroke Scale.
Indications for early IVT.

IVT: intravenous thrombolysis.
Indications for early EVT.
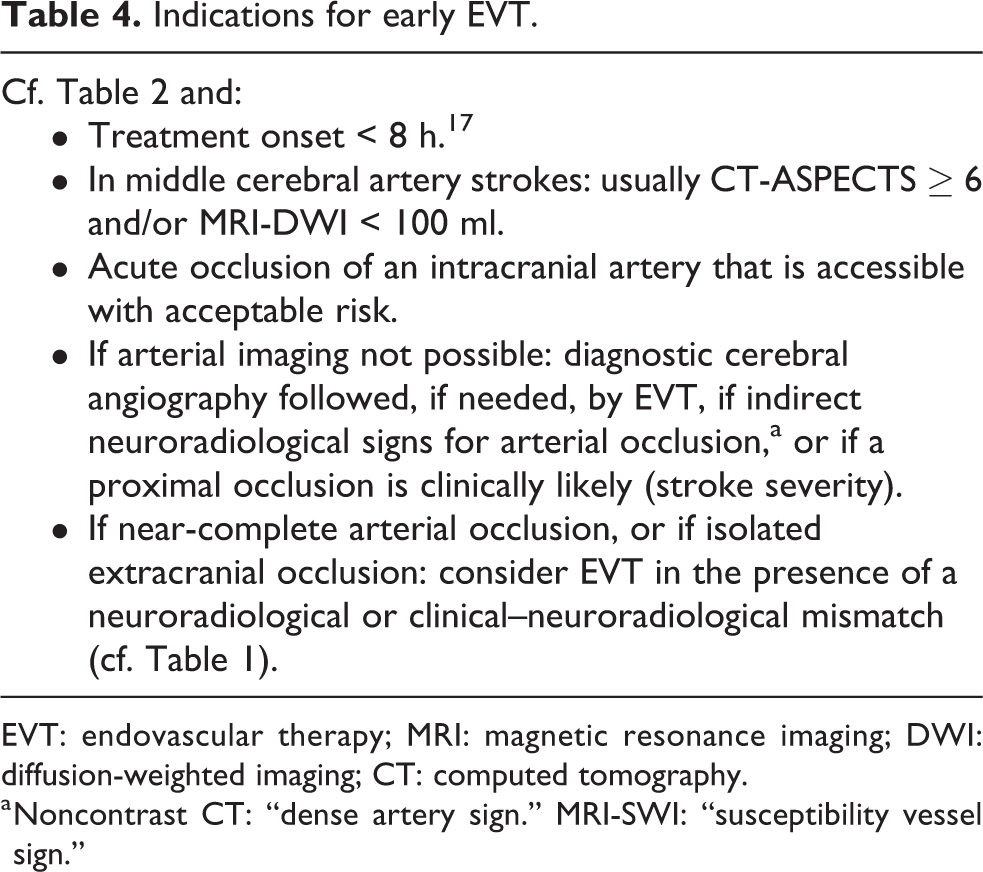
EVT: endovascular therapy; MRI: magnetic resonance imaging; DWI: diffusion-weighted imaging; CT: computed tomography.
a Noncontrast CT: “dense artery sign.” MRI-SWI: “susceptibility vessel sign.”
Indications for EVT for wake-up stroke, unknown stroke onset, or late hospital arrival.

EVT: endovascular therapy.
Indications for IVT for wake-up stroke, unknown stroke onset, or late hospital arrival.

IVT: intravenous thrombolysis; EVT: endovascular therapy; MRI: magnetic resonance imaging; FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging; CT: computed tomography.
Contraindications for IVT.

IVT: intravenous thrombolysis; EVT: endovascular therapy; aPTT: activated partial thromboplastin time; TT: thrombin time.
a No recommendation can be made regarding treatment with Andexxa® before IVT in patients with therapeutic levels of anti-Xa oral anticoagulants, because the efficacy and safety of such a pretreatment are not yet known.
Relative contraindications for IVT.
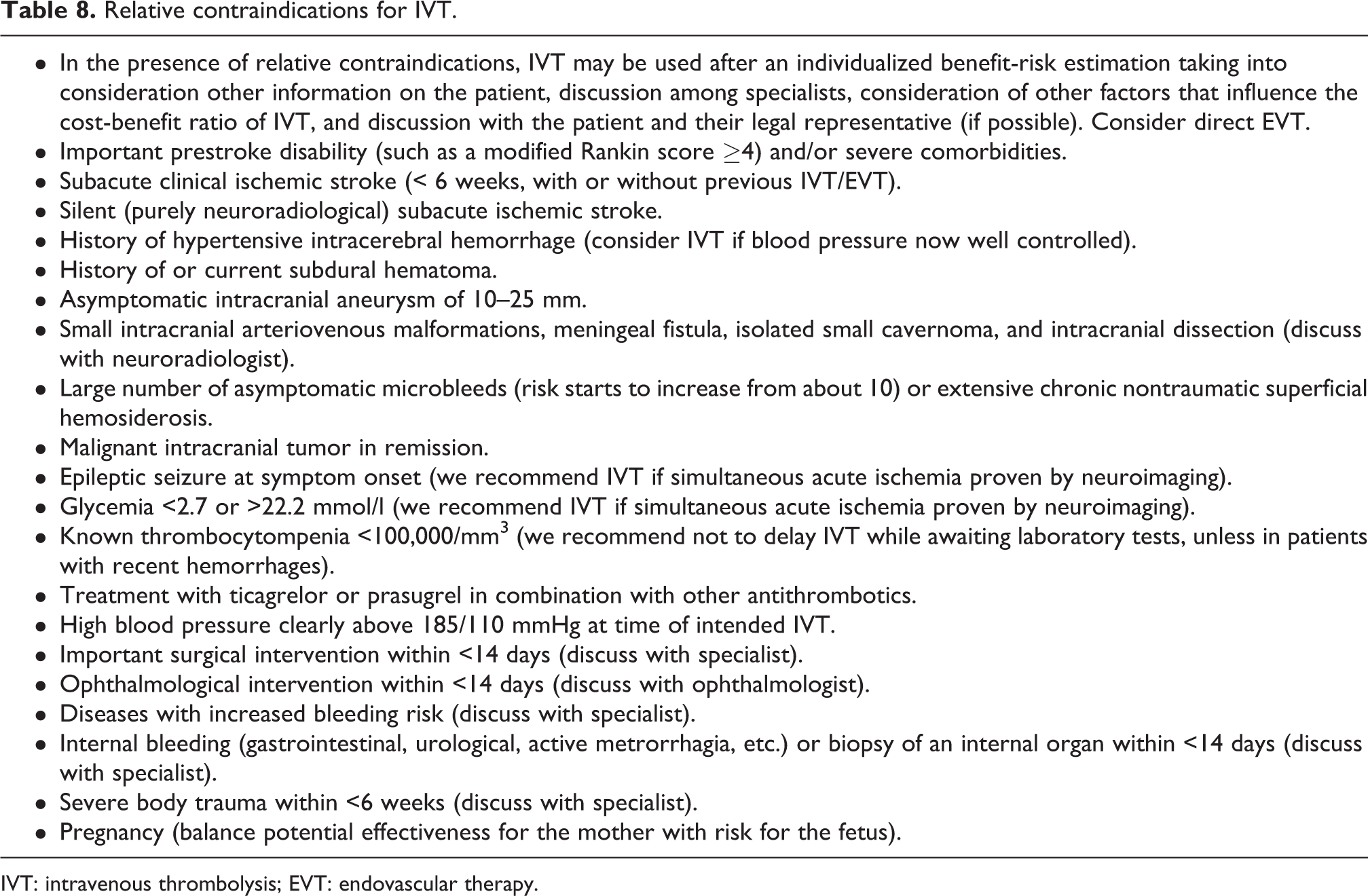
IVT: intravenous thrombolysis; EVT: endovascular therapy.
Not contraindications for IVT.

IVT: intravenous thrombolysis.
a The efficacy and safety of IVT after Andexxa® in patients on anti-Xa oral anticoagulants is not yet known.
Stroke onset is defined as the last time point when the patient was in his/her usual state of health, that is, the last proof of being without stroke symptoms. The NIHSS allows quantification of the clinical neurological deficit in stroke patients. We recommend that the NIHSS is used by medical personnel with appropriate instruction, exercise, and experience.
Given that IVT, and probably of EVT, are effective across all severities of a disabling stroke, we do not recommend to limit the treatments to a specific NIHSS window. We do recommend, however, that a disabling deficit (IVT and EVT) and/or a proven arterial occlusion within the ischemic territory (EVT) are present before initiation of treatment. For nondisabling deficits without major occlusions, IVT is may not be effective. 25
If a major occlusion is not treated initially because of mild symptoms, in the case of worsening during continuous clinical surveillance, a “rescue” revascularization may be considered.
For patients with basilar artery occlusion, we recommend applying similar revascularization criteria and time windows as for the anterior circulation. MR-based imaging can help determine the “core” and, therefore, subsequent decision-making (see Table 2). However, measurement of the penumbra for decisions in the late time window is not recommended in basilar artery occlusions.
In patients with significant preexisting disability, there is little data on the effect of IVT and EVT 60 and safety concerns are the same as in nondisabled patients. In such patients, an individual estimation of the risk–benefit ratio may be used, which also considers the patient’s personal values (if known).
There are no acute revascularization RCTs on children and adolescents up to 18 years. In this population, IVT and/or EVT may be considered along the criteria used in adult patients, if possible after a consensus discussion between neuropediatricians, adult stroke specialists, and parents. 61
Pregnancy is a relative contraindication for IVT, and potential treatment effect on the mother should be balanced by the risk of harm to the fetus. Again, we recommend a discussion with all concerned persons if this does not cause significant treatment delay. The risk for the fetus is probably minor, in particular with EVT. The usual radio-protective measures in pregnancy should be applied. 62
Neuroradiological selection of late patients
The irreversible ischemia (“core,” in general, defined by diffusion or perfusion imaging) and the reversible ischemia (“penumbra,” in general, defined by perfusion imaging or estimated from the neurological deficit) can be determined with sufficient precision for clinical decision-making. Rapid recanalization becomes more effective with a small “core” and an increasing “mismatch” between “penumbra” and “core.” Another type of “mismatch” is based on acute MRI on the presence of a DWI and absence of a FLAIR lesion; this kind of mismatch indicates the short duration of ischemia (such as <4.5–6 h) and not the direct presence of a penumbra. Different concepts of mismatch are described in Table 1.
There is also potential for a mismatch between the core and neuroradiolocially defined (good) collateral circulation, but current RCTs have not yet used this concept.
We can summarize neuroradiological findings in acute ischemia as follows:
– A large core volume increases the risk of a poor outcome and bleeding, independent of whether acute recanalization is achieved or not.
– A larger “mismatch” between penumbra and core leads to more treatment benefit if acute recanalization is achieved rapidly.
Regarding treatment decisions and its benefits, the presence of a mismatch is as follows:
– Of minor importance in the very early time window.
– More important in late time windows and in patients with unknown stroke unset.
We, therefore, recommend that neuroradiological findings are used in late decisions for IVT/EVT; they may also be used in borderline situations in the early time windows.
We recommend following the revascularization criteria described in Tables 2 –9 corresponding to inclusion and exclusion criteria used in RCTs, data from case series, other stroke treatment guidelines 37 –44 and the consensus opinion of the authors.
Additional measures during and after revascularization
Regarding the anesthesiology management during EVT: – We do not make a recommendation regarding the type of anesthesia (general anesthesia vs. conscious sedation). Arguments in favor of general anesthesia are as follows: ○ Decreased level of consciousness (Glasgow Coma Scale ≤ 8). ○ Difficult communication, agitation, and excessive movements. ○ Cardiac and respiratory instability. ○ Potentially long-lasting or complex interventions. – We recommend to elaborate institutional standardized operating procedures for anesthesiology management, aiming to ○ reduce preinterventional delays, ○ enhance patient safety, ○ respect general principles of neuroanesthesia, including pathophysiology-based blood pressure management.
Like in all strokes, we recommend that patients with revascularization treatments are admitted and continuously monitored for at least 24 h in a Stroke Unit or Stroke Center. 52,54 Treatment in intensive care in a hospital with a Stroke Unit or Stroke Center is recommended if admission criteria for intensive care are present.
We recommend that a platelet inhibitor is administered before, during, or immediately after a direct EVT, for example, with acetylsalicylic acid at a loading dose of 250–500 mg. Exceptions are patients who are already fully anticoagulated at the time of stroke. It is recommended to continue preexisting antiplatelet therapy should be continued and adapted, if needed.
We recommend avoiding antithrombotic drugs during the first 12–24 h after IVT, with justified exceptions. Prevention of deep vein thrombosis is recommended with intermittent pneumatic compression and with early mobilization of the patient. The latter may start within the first 24 h with intermittent sitting at the edge of the bed or in a chair, if the neurological deficit and collaboration permit. 64,65
According to the current evidence, acute blood pressure treatment seems to have little influence on long-term outcome. Still, the following upper blood pressure limits may be used as follows: – During and after IVT: 185/110 mmHg (mean arterial pressure (MAP) 135 mmHg); – After successful EVT resulting in a Thrombolysis in Cerebral Ischemia Score 2b or 3: 160/90 mmHg (MAP 115 mmHg); – After successful revascularization of a chronic carotid stenosis during EVT: 140/70 mmHg (MAP 95 mmHg).
Worsening symptoms during blood pressure reduction and internistic comorbidities may also be considered in the acute blood pressure management.
We recommend offering craniectomy for ischemic mass effect after IVT for large hemispheric or cerebellar infarcts according to published criteria of the SSS 66 (and may also in selected patients above age 60 67 ) after IVT and/or EVT if the clotting status (including fibrinogen levels) is within normal limits. This intervention may also be offered in the case of hemorrhagic transformation after IVT and/or EVT.
Patient information and consent for acute revascularization treatments
In an emergency medical situation in Switzerland, a patient’s consent is not required for acute treatments such as IVT and/or EVT if they are offered within scientifically proven indications. If a clear expression of treatment refusal is known (e.g. in a living will) at the time of treatment decision, we recommend that this decision is honored. Refusal of a scientifically proven therapy can only be considered valid if expressed by a patient with sufficient decisional capacity regarding the intended treatment. In noncompetent patients, we recommend that the next of kin is informed concisely about risks and benefits of the planned intervention (including anesthetic management) if this does not lead to significant time loss. Deliberations should be documented in the medical chart. If a legal representative declines a scientifically proven therapy, we recommend that the treating physician follows this advice if it corresponds to a previously expressed wish or the patient’s presumed will.
Footnotes
Appendix 1
Author affiliations, and potential past or current conflicts of interest regarding IVT and EVT.

| Name | Institution | Potential conflicts of interest |
|---|---|---|
| Patrik Michel | Service de Neurologie, Center Hospitalier Universitaire Vaudois, Lausanne | Boehringer-Ingelheim, Medtronic, PROMISE steering committee (Penumbra). All payments go to the employer and are used for research and education. |
| Michael Diepers | Neuroradiologische Abteilung, Kantonsspital Aarau | RAPID Medical, Microvention. All payments go to the employer and are used for research and education. |
| Pasquale Mordasini | Universitätsinstitut für Diagnostische und Interventionelle Neuroradiologie, Inselspital Bern | Medtronic. Honoraria for presentations and courses go directly to the employer and are used for research and education. Steering committee of the SWIFT-DIRECT trial. |
| Thilman Schubert | Diagnostische und Interventionelle Neuroradiologie Klinik für Radiologie und Nuklearmedizin Universitätsspital Basel |
None |
| David Bervini | Universitätsklinik für Neurochirurgie, Inselspital Bern | None. Honoraria for presentations and courses go directly to the employer and are used for research and education. |
| Jean-Daniel Rouvé | Service d’Anesthésiologie, Center Hospitalier Universitaire Vaudois, Lausanne | None |
| Yvan Gasche | Département d’Anesthésiologie, Pharmacologie, Soins Intensifs, & Urgences, Faculté de Médecine, Université de Genève | None |
| Guido Schwegler | Neurologie, Spital Limmattal | None |
| Christophe Bonvin | Service de Neurologie, Hôpital du Valais, Sion | Boehringer-Ingelheim: honoraria for presentations and advisory boards |
| Krassen Nedeltchev | Klinik für Neurologie, Kantonsspital Aarau | Boehringer-Ingelheim, Medtronic: honoraria for presentations and advisory boards |
| Emmanuel Carrera | Service de Neurologie, Hôpitaux Universitaires de Genève | None |
| Georg Kägi | Klinik für Neurologie, Stroke Center, Kantonsspital St.Gallen | Boehringer-Ingelheim, Zambon: honoraria for presentations and advisory boards |
| Carlo Cereda | Servizio di Neurologia, Neurocentro della Svizzera Italiana, Ospedale Civico di Lugano | None |
| Thomas Nyffeler | Neurozentrum, Luzerner Kantonsspital | None |
| Stephan Wetzel | Neuroradiologie, Hirslanden Klinik, Zürich | None |
| Susanne Wegener | Klinik für Neurologie, Universitätsspital Zürich und Universität Zürich | Boehringer-Ingelheim: for research projects |
| Henrik Gensicke | Klinik für Neurologie und Stroke Center, Universitätsspital Basel und Universität Basel | None |
| Stefan Engelter | Klinik für Neurologie und Stroke Center, Universitätsspital Basel und Universität Basel | None |
| Marcel Arnold | Universitätsklinik für Neurologie, Inselspital Bern | Boehringer-Ingelheim, Covidien, and Medtronic: honoraria for presentations and advisory boards. |
IVT: intravenous thrombolysis; EVT: endovascular therapy.
Author’s note
The guidelines were elaborated and approved by the Swiss Stroke Society, the Swiss Neurological Society, the Swiss Society of Neuroradiology, the Swiss Society of Neurosurgery, the Swiss Society for Anesthesiology and Resuscitation, and the Swiss Society of Intensive Care Medicine. The German version of this guideline is published elsewhere and is the legally binding text.
Acknowledgment
The author(s) acknowledge Mrs Melanie Price Hirt, PhD, for English language correction and editing of the text translated by the first author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Swiss Stroke Society.