
Abstract
Imaging diagnosis of nonatheromatous carotid artery disease is challenging due to its low prevalence in contrast to that of atheromatous disease. Congenital anomalies are frequently discovered incidentally, as the chronicity of these conditions allows for compensatory flow development. The inflammatory conditions typically present with nonspecific courses, and a high clinical suspicion along with timely imaging evaluation can guide the diagnosis. Carotid dissection is the result of a partial disruption of the arterial wall and can be seen in previously healthy patients, in patients with underlying noninflammatory arteriopathies or trauma. Traumatic injuries to the carotid artery may occur under many different conditions and mechanisms and timely recognition of high-risk patients improves patient outcomes. Although free-floating thrombi (FFT) formation is typically seen with atherosclerotic plaque rupture, different conditions may also predispose to FFT. In this review article, we study the different imaging features of nonatheromatous carotid artery disease using ultrasonography, computed tomography angiography, magnetic resonance angiography, and digital subtraction angiogram.
Introduction
Nonatheromatous disease is an overlooked pathology of the carotid arteries due to its very low prevalence in contrast to atheromatous disease. This group of conditions may be divided into congenital, inflammatory, and noninflammatory pathologies. Imaging particularly provides important diagnostic information in this group of diseases given the lack of specific biomarkers. This article intends to demonstrate the multiple imaging characteristics of the nonatheromatous involvement of the carotid artery.
Congenital anomalies
Congenital anomalies of the internal carotid artery (ICA) are exceedingly rare, as the ICA is one of the most important blood vessels supplying the brain. The major anomalies of the ICA, such as complete agenesis or hypoplasia, are only seen in 0.01% of the population. 1,2 Compensatory collateral flow through intercavernous anastomosis and patent circle of Willis make these conditions asymptomatic during childhood, although symptoms of vertebrobasilar insufficiency may arise later in adulthood. 3 –5 It is also known that patients with ICA congenital anomalies have an increased risk of aneurysm formation. 6
The majority of these cases are incidentally diagnosed while studying for other diseases, and the most common modalities involved are ultrasonography (US), computed tomography angiogram (CTA), and magnetic resonance angiogram (MRA). 7,8 There are multiple clues that a carotid US may provide, such as size discrepancy between the affected size and the contralateral (Figure 1a). The hypoplastic segment can also demonstrate high resistance waveforms with a slim sign representing highly a stenotic lesion. 9 However, confirmation is often obtained with CTA or MRA, showing a narrow vessel lumen. 10 Computed tomography (CT) of the skull base can show hypoplastic carotid canal, an indirect sign of congenital ICA abnormality (Figure 1b, 1c). 10 Digital subtraction angiogram (DSA) is often unable to distinguish from acquired causes of carotid stenosis and, therefore, not commonly used for the diagnosis. 11

50-year-old male with left-sided carotid bruit. (a) Transverse color Doppler ultrasound of the right ICA demonstrates a small ICA. (b) Axial CT angiography of the head demonstrates a small right precavernous ICA. (c) Axial bone window of a CT at the level of skull base demonstrates a small right foramen lacerum, confirming the presence of a congenitally small or hypoplastic right ICA. CT: computed tomography; ICA: internal carotid artery.
Agenesis or aplasia of ICA
First described in 1787 in a postmortem examination by Tode, 12 the complete or partial absence of the carotid artery can be referred as agenesis or aplasia, respectively. 13 This distinction is made based on the presence of the bony carotid canal. Agenesis occurs when there is a complete absence of the carotid canal and the ICA, whereas aplasia occurs when the bony carotid canal is present, along with a vestigial remnant of the ICA. 14 This condition is more often unilateral, but bilateral anomalies of the ICA have also been reported. 8
Hypoplasia of ICA
Although it is common to use the terms hypoplasia and aplasia interchangeably, they represent different entities according to the original classification by Lie. 14 While both hypoplasia and aplasia of the ICA present with an asymmetric bony carotid canal and narrowing of the vessel lumen, hypoplasia refers to an underdeveloped the vascular structure, whereas aplasia is mostly associated with a vestigial remnant. 14,15 Hypoplasia of the ICA shares similar incidence, demographic presentation, and clinical history compared to the rest of the congenital anomalies. It is important to note, however, that the main differential diagnosis of hypoplasia of the ICA will be any type of acquired ICA stenosis. 16
Inflammatory arteriopathies
Inflammatory diseases of the carotid arteries are usually classified in two big categories: atheromatous and nonatheromatous carotid artery disease. This review article will focus on a detailed clinical history with the physical exam can help clinicians narrow down the differential diagnosis for nonatheromatous diseases.
Symptoms can vary greatly from no symptoms to focal neurological deficits, according to the etiology. 17 Growing understanding and imaging advances have made possible earlier diagnosis of these entities. Screening tools include US with Doppler, transcranial Doppler, CTA, MRA, and positron-emitting tomography (PET). Diagnosis is generally confirmed by DSA or biopsy.
Carotidynia
Carotidynia, also known as Transient Perivascular Inflammation of the Carotid Artery (TIPIC) syndrome, is a rare vascular disorder characterized by throbbing neck pain in the area of the carotid bifurcation. 18 Pain is commonly aggravated by chewing, head movements, or even light palpation. 19 Initially proposed as a symptom shared by many inflammatory processes, recent literature has confirmed carotidynia as a separate pathological entity with distinctive radiological findings. 20 –24 The diagnostic workup for the TIPIC syndrome is extensive and often requires a high degree of suspicion from the clinician. Biopsy ultimately confirms this elusive diagnosis. 25 Most of the available information comes from case reports available in the literature.
A sonographic evaluation may show soft perivascular infiltration represented by thickening of the posterior or lateral wall of the carotid artery, which measures between 4 mm and 5 mm. Mild narrowing of the lumen can also be seen in approximately half of the patients. This perivascular infiltration is seen in CTA and MRA as fat stranding (Figure 2). 21,26 Postcontrast T1-weighted sequence can also show carotid wall enhancement. 21
40-year-old female with right-sided neck pain, fever, and malaise. Axial postcontrast fat-saturated T1-weighted images of the neck at the level of the thyroid cartilage demonstrate significant enhancement of and around the right common carotid artery extending into the parapharyngeal space and carotid space.
Giant cell arteritis
Considered one of the most common inflammatory vasculitic processes, giant cell arteritis (GCA) is known to affect both large- and medium-sized vessels (Figure 3). 27 The incidence of GCA reaches its maximum during the seventh decade of life, 28 and the highest prevalence of this disease is seen in the Northern hemisphere, particularly in the Scandinavian region. 29 Patients diagnosed with GCA can complain from unspecific systemic symptoms such as fatigue and weight loss, and prolonged fever 30 to vessel-specific manifestations such as optical neuropathy, jaw claudication, or intramural hematomas. 31 Currently, although the gold standard for diagnosis of GCA is biopsy, a negative test cannot fully exclude this disease. Under this circumstance, imaging has proven to be useful. The vessels that are commonly involved are the ophthalmic, external carotid, vertebral, subclavian, and axillary arteries.

75-year-old patient with history of monocular visual disturbance and headaches. (a) Curved reformat CT angiogram of the left subclavian artery demonstrates multifocal narrowing of the left subclavian artery and axillary artery. Minimal calcification is noted within the proximal subclavian artery. (b) CT angiogram, curved reformat centered in the right subclavian artery demonstrates a beaded appearance of the entire length of the subclavian artery with significant stenosis in its distal aspect. (c) Axial FDG PET at the level of the aortic arch shows circumferential uptake, likely representing large vessel vasculitis. (d) Thickening of the aortic wall at the level of the upper mediastinum also representing large vessel inflammation. CT: computed tomography; FDG: fluorodeoxyglucose; PET: positron-emitting tomography.
US provides a sensitivity is 87% and specificity is 96%. 32 The presence of a halo sign and elevated velocities in the superficial temporal artery increases the suspicion, especially in the absence of atheromatous disease. Recently, magnetic resonance imaging (MRI) vessel wall imaging has reported promising values in sensitivity and specificity diagnosing of GCA. In patients with proven positive biopsy for GCA, the sensitivity was 88.7% and specificity was 75.0%. 33 Visual and quantitative PET scores have demonstrated not only to have a strong regional association to GCA but were also superior to CT scores. A strong correlation between quantitative PET score and inflammation markers is usually observed, especially when using a vessel to liver ratios. 34
Takayasu arteritis
Takayasu arteritis (TA) is a rare large-vessel arteritis that is limited to the aorta and its primary branches. Although some clinical overlap can be seen with GCA, the demographical predilection of these diseases is largely divergent. In TA, the majority of the diagnosis comes from young females in their second and fifth decade of life. 35 The highest prevalence of this disease is found in Asia, particularly in Japan, 36,37 where an estimated incidence of one to two cases per million has been previously reported. 38 Newer studies, however, have detected high incidence in Turkey and Normway. 39 The American College of Rheumatology requires three of the following six criteria to be met: age at disease onset ≤40 year, claudication of extremities, decreased brachial artery pressure, blood pressure difference >10 mmHg, bruit over subclavian arteries or aorta, and abnormal arteriogram. 40
Takayasu is known to have three different phases: (1) prepulseless, where nonspecific systemic symptoms predominate; (2) vasculitic, where features of vascular involvement, such as angiodynia, is seen; and (3) fibrotic, where the long-term vascular complications, like arterial stenosis and aneurysm formation, develop. 41 Not uncommonly, the diagnosis of TA can be reached by a thorough clinical history, physical exam, and imaging findings suggestive of large vessel narrowing. The imaging modalities employed are US, CTA, or MRA; the common findings are pictured in the following.
Ultrasound has demonstrated significant use in the carotid and femoral artery involvement (Figure 4a). Characteristically color Doppler sonography revealed a smooth, homogeneous, isoechoic, circumferential thickening of the vessel wall. This accompanied with varying degrees of stenosis and calcification or shadowing in 27% of the patients. Doppler waveforms usually demonstrate high resistant waveforms. 40 Ultrasound is also the preferred method for follow-up treatment given its noninvasive, and nonradiation properties and low cost.

15-year-old female presented with loss of strength in the right hemibody. (a) Transverse B mode ultrasound of the left common carotid artery demonstrates extensive endothelial thickening of the carotid wall with a small residual lumen diameter. (b) Coronal MRA reconstruction demonstrating occlusion of the common carotid arteries and right innominate bilaterally, stenosis of the left subclavian artery, and reflective of the patient’s known diagnosis of the Takayasu disease. (c) MRA of the head demonstrates absence of flow-related enhancement of the left ICA, middle cerebral artery, and proximal anterior cerebral artery.
CTA and MRI angiographies have several benefits in the early staging of the disease, since they delineate the extent of the disease (Figure 4b, 4c). The typical manifestation on CT images is the concentric vessel wall thickening of the involved arteries. Previous works suggested that mural thickening may be the most important finding in the early phases of the disease. 42
Postradiation carotid arteritis
The first report of radiation-induced arteritis dates back to 1893, when intimal thickening and medial vacuolization of a vessel wall from a radiation-induced skin ulcer was analyzed. 43 Since then, two different patterns of vessel wall injury have been described based on the timing of radiation exposure. Acute injuries can be seen up to 1 year after exposure; vessels are prone to inflammation, rupture, and thrombosis. 44,45 Chronic radiation exposure is known to cause accelerated atherosclerosis, 46,47 calcification, and fibrosis, 43,45 all leading to vascular stenosis (Figure 5). An increased risk of postradiation aneurysm formation with subsequent rupturing has also been reported. 44 Since the histological changes are identical to those in naturally occurring atherosclerosis and fibrosis, 45 knowing the previous antecedent is pivotal in making the diagnosis. The most commonly affected vessels are the cervical and cranial arteries, 48 followed by the visceral and pelvic arteries. 49

55-year-old male with thyroid cancer. (a) Axial CT angiogram of the neck demonstrates heavily calcified plaque within the anterior aspect of the common carotid arteries bilaterally. (b) Dense circumferential calcified plaque is noted within the left common carotid artery resulting in moderate stenosis of this vessel. (c) Coronal reformat of the carotid arteries demonstrates extensive calcification of the proximal mid and distal common carotid arteries, typical in patients with history of radiation to the neck. CT: computed tomography.
Ultrasound imaging shows an increase in carotid intima-media thickness, carotid stenosis, and consequently leads to a higher risk of cerebrovascular events such as transient ischemic attack and stroke. Postradiation patients showed a statistically significant higher incidence of overall stenosis (pooled risk ratio = 4.17 [2.44, 7.10], p < 0.00001) and an even greater incidence of significant stenosis (50% or more; pooled risk ratio = 8.72 [3.53, 21.55], p < 0.00001). 50
Carotid dissection
Arterial dissection is the result of any process that disrupts the integrity of the arterial wall with subsequent bleeding into a false lumen. 51 Continuous blood extravasation into any layer of the arterial wall can result in pseudoaneurysms formation and intramural hematomas. 52 When found in the extracranial carotid arteries, it is usually located distal to the carotid bulb. 53 Common symptoms that should raise suspicion for this entity include headache, neck pain, transient ischemic attacks, as well as spontaneous Horner syndrome. 54
Although DSA is considered the gold standard, CTA and MRA are most commonly used in the acute setting. 52,55,56 Contrast-enhanced MRI that includes fat-saturated T1 sequence and time-of-flight MRA is considered the best initial study, demonstrating intramural hemorrhages, and narrow vessel lumen. 57 It is important to note that the isointense visualization of blood in the acute period may be difficult for the diagnosis using T1-weighted sequences. 52,58 Common imaging findings in CTA include the target sign, which represents a narrow lumen with crescentic mural thickening and annular enhancement of the vessel wall. 58 Other findings include an intimal flap, intramural hematomas, and pseudoaneurysm formation. Previous search has established that the diagnostic performance between CTA and MRA are comparable, 59 and the choice of modality should depend on the availability. DSA study is reserved for scenarios where there is a high suspicion of dissection and the other modalities are inconclusive.
Doppler sonography can also be useful with some limitations. US evaluation is able to yield information about the presence of proximal dissection membranes, intimal flap, and luminal stenosis (Figure 6a). Dissection membranes are characterized by thickened and hypoechoic vessel walls, while luminal flaps are hyperechoic structures found within the mural hematomas. 60 Luminal stenosis can be evaluated by measuring the peak systolic and diastolic velocities. The diagnostic performance of the ultrasound depends on the location and severity of symptoms, and it is currently recommended that all imaging findings should be confirmed with CT, MRI, or DSA (Figure 6b, 6c). 60

40-year-old female with history of FMD, migraines, and high blood pressure. (a) Color flow ultrasound of the right ICA demonstrates turbulent flow and focal outpouchings of the ICA. (b) DSA of the right internal carotid shows a classic dissection and pseudoaneurysm formation. (c) Multiple striations within the proximal ICA, also pathognomonic of FMD. FMD: fibromuscular dysplasia; ICA: internal carotid artery; DSA: digital subtraction angiogram.
Spontaneous carotid dissection
Truly spontaneous carotid dissections compose approximately 60% of all cervical dissections. However, close to 40% of the cervical dissections are preceded by minor or daily activities and, therefore, good clinical history is usually warranted for this diagnosis. 61
Not infrequently, patients presenting with spontaneous carotid artery dissection (SCAD) may have an underlying predisposing factor, such as connective tissue disorders, 62 hypertension, 63 or recent infections. 64 Marfan syndrome, Ehler–Danlos, and fibromuscular dysplasia (FMD) are common examples of connective tissue diseases with high predisposition to SCAD and can also manifest in the carotid arteries with stenosis or aneurysm formation. 65 –69
Traumatic carotid dissection
Although less prevalent than spontaneous carotid dissection, traumatic carotid artery dissection (TCAD) has an extremely high fatality rate. 70 The mechanism of injury usually involves rotational, hyperextension, or hyperflexion injuries as seen in motor vehicle accidents. 55 The clinical diagnosis can be challenging, since most patients are asymptomatic or have mild symptoms for up to 12 h until cerebral ischemia manifest. 71 Low-velocity impact in patients with underlying conditions, such as connective tissue diseases, may also increase the risk of TCAD. 72 In the setting of blunt injuries to the head and neck, a high degree of clinical suspicion is warranted to make the correct diagnosis. 70,73
Not infrequently, TCAD is seen in combination with traumatic pseudoaneurysms, but these are exceedingly rare, seen in only in 0.02–0.4% of all traumas. 74,75 Approximately 30–60% of the patients with traumatic pseudoaneurysms can be asymptomatic (Figure 7). Common complications include thrombosis with subsequent ischemic embolization, enlargement with mass effect and cranial palsies, or hemorrhage due to rupture. 76 Dissections and pseudoaneurysm formation are highly associated with thromboembolic infarcts, 52 and timely recognition of these two vascular injuries in the traumatic setting can reduce neurological sequelae and improve patient outcome. 58

A 25-year-old male patient presented to the emergency department with altered mental status after a biking accident. (a) Axial view of a CT angiography at the level of the skull confirms right intraluminal thrombus in the right ICA. (b) Coronal view confirms the presence of intraluminal thrombus, pseudoaneurysm formation, and luminal stenosis of the right ICA. (c) T1-weighted image with fat saturation sequence, axial view at the level of the skull base demonstrates hyperintensity in the right ICA, confirming the diagnosis of traumatic carotid dissection. CT: computed tomography; ICA: internal carotid artery.
Carotid webs
Also known as intimal FMD, this entity represents a rare variant of FMD with a different clinical and radiological presentation from other more common variants. 77,78 In contrast to the medial fibroplasia FMD, carotid webs are typically not associated with an intermittent luminal narrowing. 79,80 Angiographically, it is characterized as thin, membranous-like tissue extending from the vessel wall that creates an endoluminal filling defect and past efforts to describe it include webs, 81 septa, 82 shelfs, 83 and pseudovalvular folds (Figure 8). 84 The clinical course of carotid webs also differs from classic FMD variant, being more frequently linked to thromboembolic events despite treatment. 77 Recognition of this angiographic variation of FMD is important due to the high risk of recurrence of thromboembolic events. 77,83

48-year-old female with history of transient right upper extremity weakness. (a) Curved reformat reconstruction of the left carotid artery demonstrates a web-shaped lesion within the inferior aspect of the bulb, which results in mild narrowing of the ICA. ICA: internal carotid artery.
Free-floating thrombus
Free-floating thrombi (FFT), although a rare entity, 85,86 can be found in the carotid arteries. To consider this diagnosis, circumferential flow around the thrombus is required. The pathogenesis is thought to involve rupturing of an atherosclerotic plaque, with subsequent in situ thrombi formation. 85 Additional risk factors for developing FFT include active malignancy, infectious processes, and pregnancy. 87 More than 90% of the patients will present with acute neurological deficit. 88
All diagnostic modalities show a filling defect surrounded completely by contrast, and when compared, a high degree of congruency is seen across (Figure 9). 88 Previously, DSA was frequently used in the diagnosis of FFT, but noninvasive techniques are now commonly used. 87 Currently, the American Heart Association has established that the preferred modality to study any acute neurological deficit is CTA.

73-year-old male patient presented to the emergency department with left hemiparesis, altered mental status, and slurred speech. (a) CT angiogram, axial view at the level of the neck demonstrated a filling defect in the right ICA, corresponding to the “donut sign.” (b) Coronal reformat confirms the finding of intraluminal filling defect distal to the carotid bifurcation, confirming the presence of free-floating thrombus. CT: computed tomography; ICA: internal carotid artery.
Carotid body tumor
The carotid body is located within the adventitia of the common carotid artery at the inferomedial aspect of the carotid bifurcation. 89 Embryologically, carotid body tumors (CBTs) are derived from the neural crest. The incidence of CBTs is less than 1 in 30,000 and rarely occurs before the age of 20. The most common presentation of CBT is an asymptomatic neck mass in 75.3% of patients, followed by symptomatic patients in 14%. Other classical indications for work up in patients with CBT are cranial nerve palsy in 3.1%, headache in 2.6% and dysphonia in 1.7% of the cases. The classic syncopal episode is only present in 1.5%. 90
Color Doppler US is a useful method in triaging patients with suspected CBTs. US imaging depicts 86% of lesions measuring a maximum diameter of 5–10 mm 91 and prior reports demonstrate a sensitivity of 92% and a specificity of 100%. The classic US imaging features is an oval, solid, and hypoechoic mass located in the carotid bifurcation. Color Doppler US may reveal a richly vascularized mass.
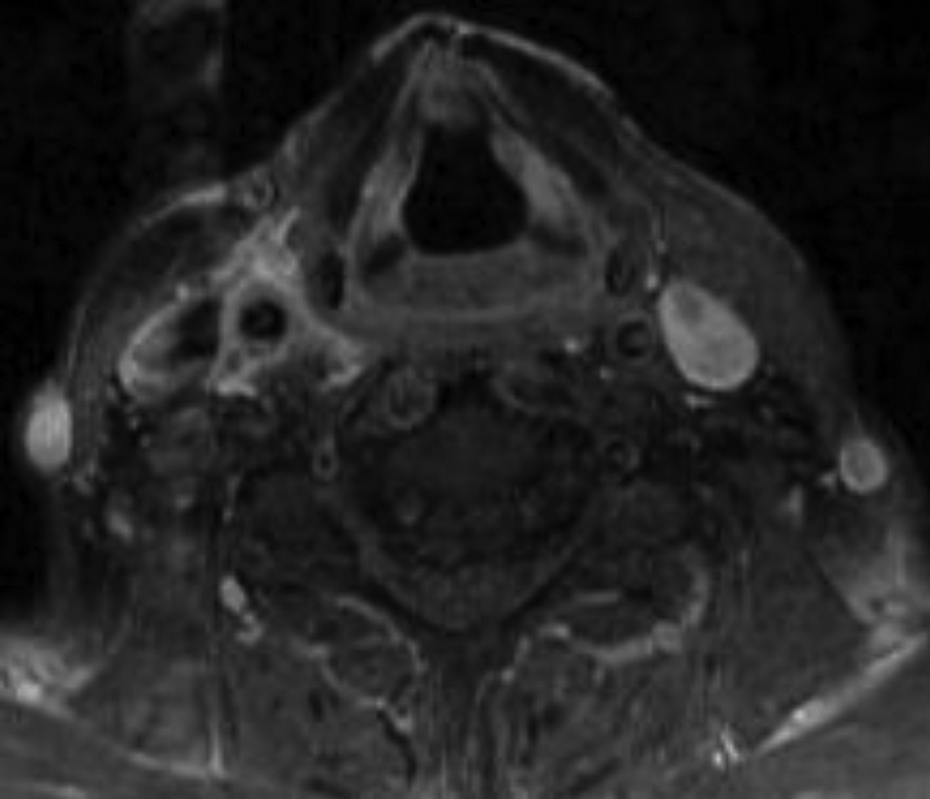
CTA of the neck can advantageously determine the anatomical relationship between the CBT mass and the vascular and nerve roots (Figure 10). The lesion usually appears as a soft tissue density mass with avid enhancement. Contrast-enhanced MRI is ideal for the characterization of CBTs, as it classically shows a “salt and pepper” appearance. The “salt and pepper” appearance is the product of focal hemorrhage as the hyperintense lesions and flow voids as the hypointense lesions. 92
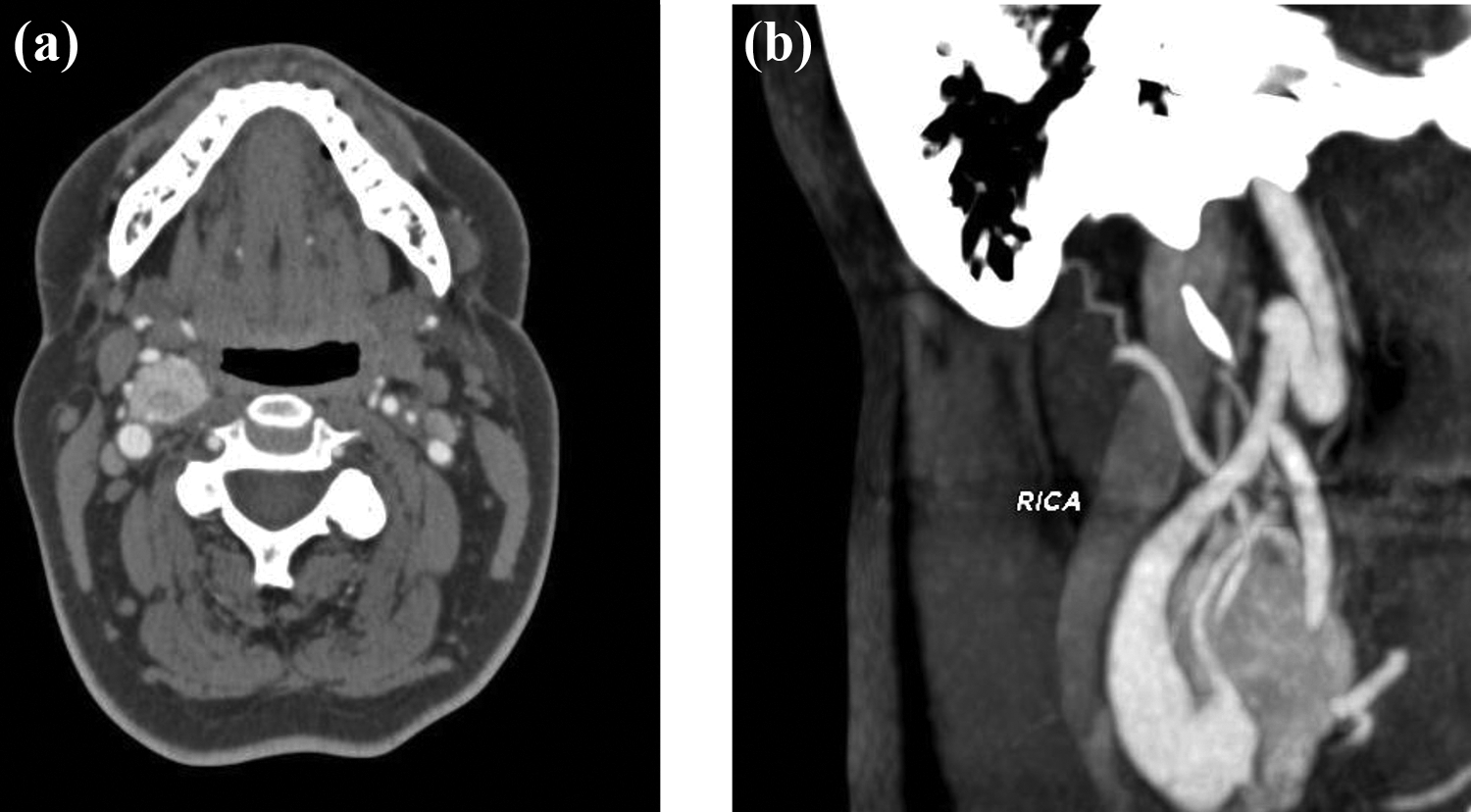
(a) Axial CT angiogram of the neck at the level of the carotid bifurcation demonstrates a heterogeneously avidly enhancing mass splaying the ICA posteriorly and the external carotid artery anteriorly. (b) Curve reformat centered within the right ICA demonstrates the relationship of the heterogeneously enhancing mass with the external carotid artery and ICA. CT: computed tomography; ICA: internal carotid artery.
Footnotes
Author contributions
JM conceived the study. DM reviewed the literature and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.