
Abstract
Objectives:
To identify new magnetic resonance imaging (MRI) patterns in patients with high-grade glioma treated with bevacizumab (Avastin®).
Methods:
The retrospective study was approved by the institutional review board. An extended case series of 27 patients (19 men, 8 women) with age range of 22–76 years and an average age 52 years were studied by 1.5T/3T MRI (Siemens scanner Erlangen, Germany). Protocol included axial T1-wi spin echo (SE), axial T2-wi fast SE, three-dimensional fluid-attenuated inversion recovery (3D FLAIR), axial diffusion tensor imaging, axial T2-wi gradient echo (GE), dynamic-susceptibility contrast T2-perfusion, axial T1-wi post-gadolinium (Gd) (0.2 ml/kg of body weight) and 3D T1-wi (weighted) GE post-Gd. Evaluation comprised oedema or low-grade tumour infiltration using FLAIR sequences, perfusion using relative cerebral blood volume (rCBV) and enhancement using T1-wi post-medium contrast images.
Results:
At baseline, the study included 27 patients, of which 14 patients were excluded and 13 patients analysed. One patient under treatment showed persistent hyperperfusion, three mixed perfusion, six hypoperfusion and three normal perfusion. FLAIR sequences were used in oedema analysis. When treated, 10 patients showed decrease in perilesional oedema, 1 showed increase in perilesional oedema and 2 had stability in perilesionnal oedema. Lesion enhancement was analysed using axial T1-wi SE post-Gd images; 12 patients showed decrease and 1 patient showed stability in lesion enhancement.
Conclusions:
Bevacizumab (Avastin) alters the process of angiogenesis resulting in different perfusion patterns in patients with disease progression that must be known in order to avoid erroneous interpretation.
Keywords
Introduction
Gliomas account for 40–50% of all primary central nervous system neoplasms. 1,2 These lesions include a spectrum of low-grade astrocytomas and high-grade tumours, with glioblastoma multiforme being the most malignant type. High-grade gliomas are highly vascular lesions that show enhancement with contrast magnetic resonance (MR) in over 90% of cases with an often irregular, nodular and occasionally ring-like pattern. Surgical resection, chemotherapy and radiation therapy are the standard treatments for patients with such tumours. However, despite the treatments available, the prognosis for these patients is dismal, with a 2% survival rate at 3 years and a median survival of 14.6 months. 3
Bevacizumab (Avastin®) is a monoclonal antibody (immunoglobulin G [IgG]) to vascular endothelial growth factor (VEGF). As high-grade gliomas are highly vascularized and express VEGF, targeting the vascular endothelium is an interesting treatment option for these patients. VEGF is required for vasculogenesis (i.e. the de novo formation of blood vessels from hemangioblast during embryogenesis) and for angiogenesis (i.e. the formation of new vessels from existing ones). 4 VEGF is a cytokine that acts as a regulator of angiogenesis and is secreted by tumour cells in response to various stimuli such as hypoxia. 5 VEGF are highly expressed in glioblastomas, underlining the importance of angiogenesis in these tumours and the potential of treatment with anti-angiogenic molecules such as bevacizumab. 6 Given the role of VEGF in tumour growth, drugs targeting VEGF have become part of many anti-tumour therapies. 7 Studies regarding clinical trials in patients with a relapse have been promising. Based on this finding, in 2009 for recurrent glioblastoma, bevacizumab has been approved by the US Food and Drug Administration as a therapy for patients with glioblastoma unresponsive to conventional treatment . 7 Our study purpose is to identify new magnetic resonance imaging (MRI) perfusion patterns in patients with high-grade brain tumours treated with bevacizumab and to analyse oedema and lesion enhancement in these patients whilst under treatment.
Materials and Method
The inclusion criteria of patients in our study are diagnosis of glioblastoma confirmed by biopsy and treated with bevacizumab in our institution. Our study received approval from the institutional review board. In these patients, the indication for bevacizumab therapy is progression under conventional chemotherapy. The dosage received by patients is 10 mg/kg every 2 weeks with a cycle duration of 4 weeks.
Extended case series of 27 patients followed in our centre were included (19 men and 8 women), with age ranging from 22 to 76 years and an average age of 52 years. These patients were studied by 1.5T and 3T MRI (Siemens scanner Erlangen, Germany), with each patient followed on the same machine. Protocol performed was axial T1-wi spin echo (SE), axial T2-wi fast SE, three-dimensional fluid-attenuated inversion recovery (3D FLAIR), axial diffusion tensor imaging (DTI) 30 directions, axial T2-wi gradient echo (GE), perfusion, axial T1-wi post-gadolinium (Gd) (0.2 ml/kg of body weight) and 3D T1-wi GE post-Gd. Evaluation comprised analysis of oedema or low-grade tumour infiltration using FLAIR sequences, hypo- or hyperperfusion of lesions using rCBV and enhancement using T1-wi post-medium contrast images with an emphasis on the perfusion of the lesions. cerebral blood volume (CBV) maps were analysed using magnetic resonance work place (MRWP) syngo perfusion post-processing software, and an region of interest (ROI) of 1 cm2 was drawn in the target region of the tumour for each patient. The analysis was performed by a neuroradiologist with 10 years of experience and a radiology resident with 2 years of experience in the field.
Results
Of the 27 patients included in the study, 14 were excluded – 8 excluded due to incomplete follow-up and 6 presented an alternative tumour grade or type upon biopsy and no longer fulfilled the inclusion criteria. Thirteen patients were included in the final analysis of our study. Patients were followed by MRI for an average of 22 months (range 12–42 months). For each patient, three aspects were studied: firstly, perfusion of the lesions was analysed using rCBV images, while under treatment; secondly, oedema was analysed using FLAIR images in correlation with the perfusion; and thirdly, lesion enhancement was analysed using T1-wi SE post-Gd images.
Perfusion results were divided into four groups based on tumour perfusion: hyperperfusion, mixed perfusion, hypoperfusion and normal perfusion. The majority of patients (6 patients, 46%) presented tumour hypoperfusion on MR follow-up under bevacizumab treatment (Figures 1 and 2). Of these patients, four presented a rebound effect with rapid progression of the tumour after completion of treatment (with radiologic and clinical progression) and one patient under treatment developed new lesions at a site distant from the primary tumour and the new lesions were also hypoperfused (Figure 3). The one other patient under treatment, who showed hypoperfusion of lesions, also showed stability in the MRI follow-ups that were performed before death. Mixed perfusion was found in three patients (23%) (Figure 4) and persistence of hyperperfusion despite bevacizumab treatment was found in one patient (8%) (Figure 5). While undergoing treatment, normalized perfusion was found in three patients (23%) in our study. The presence of hypoperfused lesions limits the utilization of enhancement as a criteria for disease progression. 8

Hypoperfusion. A 48-year-old female patient. Images on the top row before starting bevacizumab. Axial T1-wi SE post-Gd images from this date show important lesion enhancement (a); FLAIR sequences show a zone of hyperintensity (b); and perfusion images show the areas of hyperperfusion (c, white arrows) and oedema which is hypoperfused (c, asterisk). On the bottom row, images dating treatment beginning show a decrease in lesion enhancement (d), a decrease in oedema (e) and a decrease in hyperperfusion (f). wi: weighted; SE: spin echo; Gd: gadolinium; FLAIR: fluid-attenuated inversion recovery.

Hypoperfusion. A 44-year-old male patient. Axial T1-wi SE post-Gd images with corresponding CBV images. The first image is before starting treatment and shows a frontal lesion with enhancement (a) and hyperperfusion (a′, black arrows). After the start of treatment, we note decreased enhancement (b) and decreased perfusion (b′, black asterisk). After the end of treatment, we note a rapid progression in both lesion enhancement (c, d) and clear hyperperfusion (c′, d′) (black arrows) with a rebound effect with rapid tumour growth. wi: weighted; SE: spin echo; Gd: gadolinium; CBV: cerebral blood volume.

Hypoperfused new lesions. T1-wi SE post-Gd image dating before the beginning of treatment (a) with bevacizumab shows important lesion enhancement and a zone of hyperperfusion visible on the corresponding CBV image (a′, white arrow). After 26 days of treatment, decreased lesion enhancement was observed (b) and the absence of hyperperfusion on CBV images was also observed (b′). Images show progression with the appearance of new lesions at distant sites in the contralateral cerebral hemisphere whilst still under treatment, note the absence of hyperperfusion of the new nodules and of the initial lesion (c, c′ white arrows). wi: weighted; SE: spin echo; Gd: gadolinium; CBV: cerebral blood volume.

Mixed perfusion. A 55-year-old female patient. Before treatment with bevacizumab, lesion enhancement on axial SE T1-wi post-Gd (a) with hyperperfusion on the CBV image (white arrow, a′) was observed. Lesion enhancement of an insular nodule before treatment and axial SE T1-wi post-Gd (b) with hyperperfusion on CBV images (b′, white arrow) were observed. Decreased lesion enhancement was observed after beginning treatment (c) with a mixed perfusion response (c′) showing persistence of areas of hyperperfusion (white arrow) and regression of other zones of hyperperfusion. Rapid progression was observed with increased lesion size (d) and hyperperfusion (d′) (white arrows), 1 month after end of treatment. wi: weighted; SE: spin echo; Gd: gadolinium; CBV: cerebral blood volume.
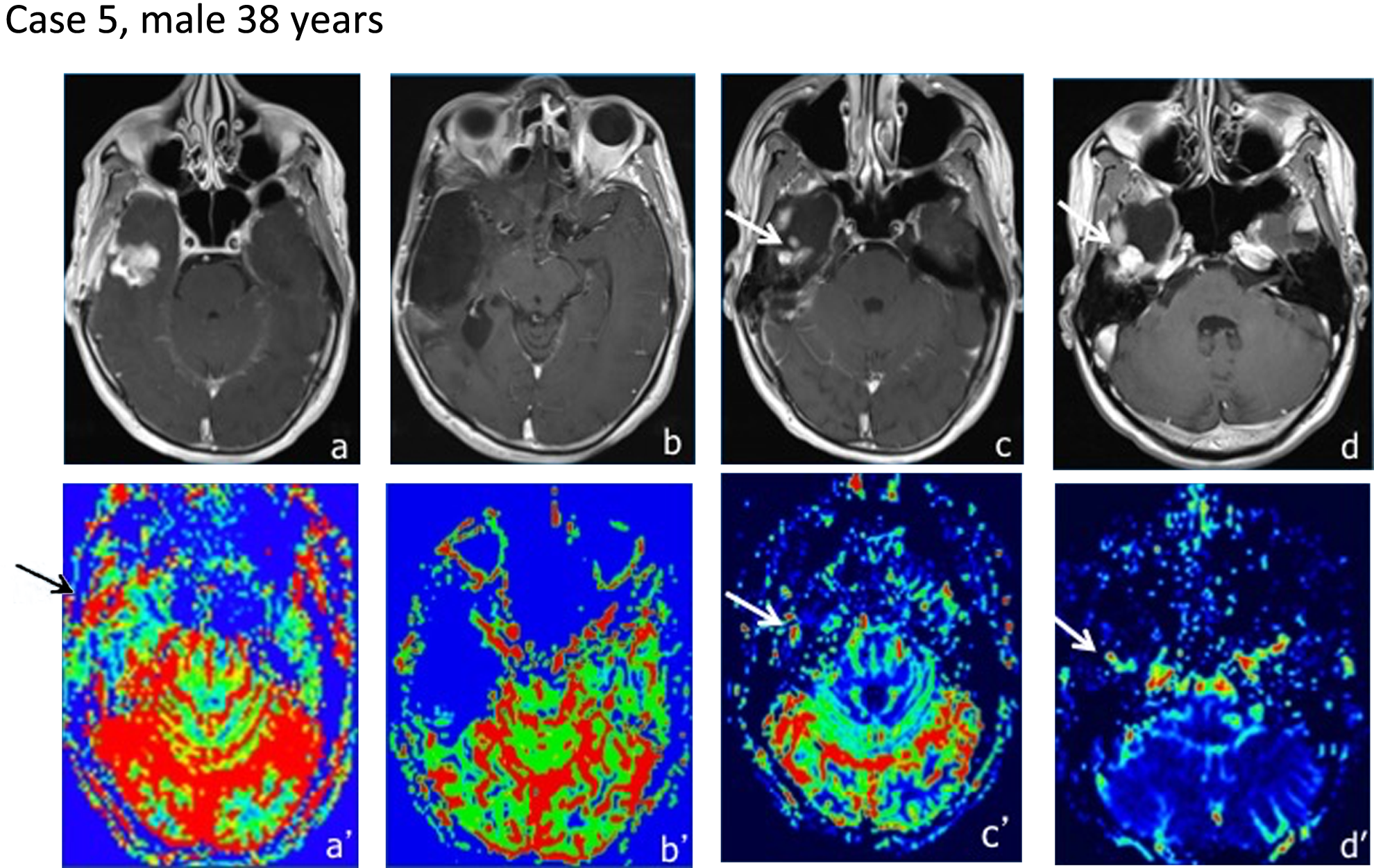
Hyperperfusion. A 38-year-old male. Axial T1-wi SE post-Gd images show a right temporal lesion with enhancement (a) and hyperperfusion on CBV images (a′, white arrow). Post-operative imaging does not show any residual tumour (b). Images showing two new nodular enhancement zones (c), (white arrow) with hyperperfusion (c′), during treatment. While undergoing treatment, progression in tumour growth was observed with an increase in the regions of enhancement (white arrow) (d) presenting hyperperfusion (d′, white arrow). wi: weighted; SE: spin echo; Gd: gadolinium; CBV: cerebral blood volume.
While undergoing treatment, oedema was analysed for each patient using FLAIR sequences and perfusion; 10 patients (77%) showed a decrease in oedema, 1 patient (8%) showed increased oedema and 2 patients (15%) showed stability in perilesional oedema. During treatment, FLAIR images and perfusion were also used to identify the appearance of low-grade tumour infiltration. The vasogenic oedema and low-grade tumour infiltration were differentiated using perfusion images. Vasogenic oedema shows reduced CBV and cerebral blood flow (CBF), which are demonstrated by previous studies. This is mainly caused by the compression of small vessels due to oedema. 9 While undergoing treatment, none of the patients included in our study demonstrated the appearance of low-grade tumour infiltration on FLAIR sequences.
The third axe of our analysis was the identification of changes in lesion enhancement, during treatment. At the time of treatment, lesion enhancement was analysed using axial T1-wi SE post-Gd images. Twelve patients under treatment showed a decrease in lesion enhancement and 1 patient showed stability in enhancement. Despite this decrease in lesion enhancement, the majority of patients undergoing treatment showed a radiologic and clinical progression of their illness.
Discussion
Bevacizumab is a second-line anti-VEGF target-therapy agent used in the treatment of highly vascular tumours such as glioblastomas. The study of MRI patterns in our patients undergoing treatment enabled us to identify new and interesting patterns. The analysis of lesion perfusion showed that hypoperfusion is the predominantly observed perfusion pattern. This pattern can be explained by the mechanism of action of the molecule that prevents the development of a rich vascular system with a regression of hypervascularization in the tumour. The absence of hypervascularization was not synonymous with regression as we observed disease progression in patients despite the absence of hypervascularization on perfusion images. As shown by other groups, the patients often had dramatic disease progression after an initial response, without an improvement in the overall survival, but they showed improved progression-free survival and quality of life. 4,10 It has been hypothesized that this is due to the initiation of compensatory survival pathways and the upregulation of hypoxia-inducible factors which enhance tumour cell invasion, cell growth and cell survival, resulting in increased tumour aggressiveness. 11
Oedema was analysed for each patient under treatment, and the vast majority showed decreased oedema, which is irrelevant to the final outcome. This decrease in oedema has been shown to have a positive effect on the neurological symptoms, 12 with an ability to substitute corticosteroid therapy. Studies have shown decrease in or stabilization of corticosteroid doses in patients treated with bevacizumab alone or in combination with irinotecan. 13 In our patient series under treatment, the analysis of FLAIR sequences did not show low-grade tumour infiltration, which was reported in other studies (e.g. Norden et al. observed the appearance of FLAIR lesions, during treatment). 3 However, it is important to underline the importance of assessing the low-grade infiltrative tumoral zones in these patients, which are not visible on classical contrast-enhanced T1-weighted images. It is essential to analyse the non-enhancing tumoral components, at the time of following up these patients. 14 The extent of peritumoral oedema is a prognostic factor that translates into a poor clinical outcome. 15 The differentiation between vasogenic oedema and low-grade tumour can be facilitated using the perfusion images, leading to decreased CBV and CBF caused by small vessel compression due to oedema. The utility of DTI in the differentiation of these two entities is controversial, with mixed results from different groups. 9,16
We observed a decrease in tumour enhancement in the majority of patients undergoing treatment. This can be explained by the normalization of the tumour vascular bed and notable decrease in vessel permeability. Despite a decrease in tumour enhancement on T1 Gd-enhanced images, clinical progression has been described in the groups of patients under bevacizumab treatment, arguing in favour of tumour extension despite a decrease in enhancement. This is in turn explained by the normalization of the blood–brain barrier. 17 However, as described by Figueiras et al., this restoration in the blood–brain barrier can lead to a decrease in the delivery of drugs to the tumour in the long-term, leading to a vasculature that is no longer efficient in the delivery of drugs. 17,18 As shown by other studies, we did not observe a modification in the progression pattern from local to diffuse. 19
Monotherapy with bevacizumab has not been shown to be curative maybe because it is unable to kill all cancerous cells, leading to inefficient drug delivery and tumour relapse through alternative pathways of angiogenesis. 5,18 As shown by other groups, no increased overall survival was observed in our patients. 4,20–22
While under treatment, the challenge of recognizing imaging patterns and their implications on patient prognosis can be facilitated with other techniques such as spectroscopy and positron emission tomography (PET). Wenger et al. showed that an elevated pH at baseline might precede progression in patients with recurrent glioblastoma treated with bevacizumab. 23 Beppu et al. demonstrated that assessment using 11C-methyl-L-methionine PET (MET-PET) enabled the differentiation of true responders from pseudoresponders. 24 Limitations of the study include the retrospective design and the small size of the population studied.
Conclusion
Treatment with bevacizumab (Avastin) alters the process of angiogenesis, resulting in different perfusion patterns in patients with disease progression. These new patterns comprise hypoperfusion, mixed perfusion and hyperperfusion and must imperatively be known in order to avoid erroneous interpretation of imagery results in the follow-up of these patients as the absence of hyperperfusion cannot be used as a reliable sign for the absence of progression. No significant differences in survival were observed between these three patterns.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.