
Abstract
Summary Statement
We report a case of paracentral acute middle maculopathy following routine sinus surgery. Although evidently rare, this is a newly noted possible complication of sinus procedures that should be considered in the setting of postsurgical vision loss.
Introduction
Paracentral acute middle maculopathy (PAMM) is a finding seen on spectral-domain optical coherence tomogram (SD-OCT) felt to be secondary to ischemic changes in the intermediate and deep retinal capillary vasculature first described by Sarraf et al in 2013. 1 It has been described as related to a variety of conditions causing insufficient blood flow within the deep capillary plexus. 2 We describe a case of PAMM that developed following a routine sinuplasty procedure. To our knowledge, this is the first reported case of PAMM associated with sinus surgery.
Case Report
A 47-year-old woman with a history of migraines and sinusitis secondary to IgA deficiency presented to the outpatient retina clinic complaining of acute onset of a “gray patch” in the inferior field of vision in the left eye. She reported that she had undergone a sinuplasty procedure performed under local anesthesia 2 days prior with visual symptom onset the evening of surgery. The operative report was reviewed, revealing that this procedure involved anesthetic usage of topical lidocaine 4% and Afrin, topical lidocaine 4%/1:1000 adrenaline, and injections of 1% lidocaine and epinephrine into the patient’s uncinate process, middle turbinate, and sphenopalatine region. The patient had undergone bilateral maxillary and sphenoid sinus balloon dilation at up to 12 cm H2O pressure for 2 minutes per sinus. She was left packed with lidocaine and adrenaline cotton balls at the end of her procedure. On ophthalmic examination, visual acuity was 20/20 in both eyes. Dilated fundoscopic examination revealed pearlescent retinal changes in the superior parafoveal macula of the left eye (Figure 1). The examination was otherwise unremarkable, with no optic disc pallor, retinal nerve fiber layer defects, hemorrhages, holes, or tears noted in either eye. Optical coherence tomography (OCT) showed a demarcated hyperreflective band extending from the inner plexiform layer to the outer plexiform layer (Figure 2, A). This corresponded to a hyporeflective parafoveal lesion on the near-infrared image. There were no signs of retinal ischemic perivascular lesions noted on OCT in either eye. Early- and late-phase fluorescein angiography (FA) demonstrated normal vascular filling without any perfusion defects or leakage (Figure 3). Central 10-2 Humphrey visual field testing revealed an inferior paracentral scotoma in the left eye, which aligned with the patient’s subjective visual loss (Figure 4, A).
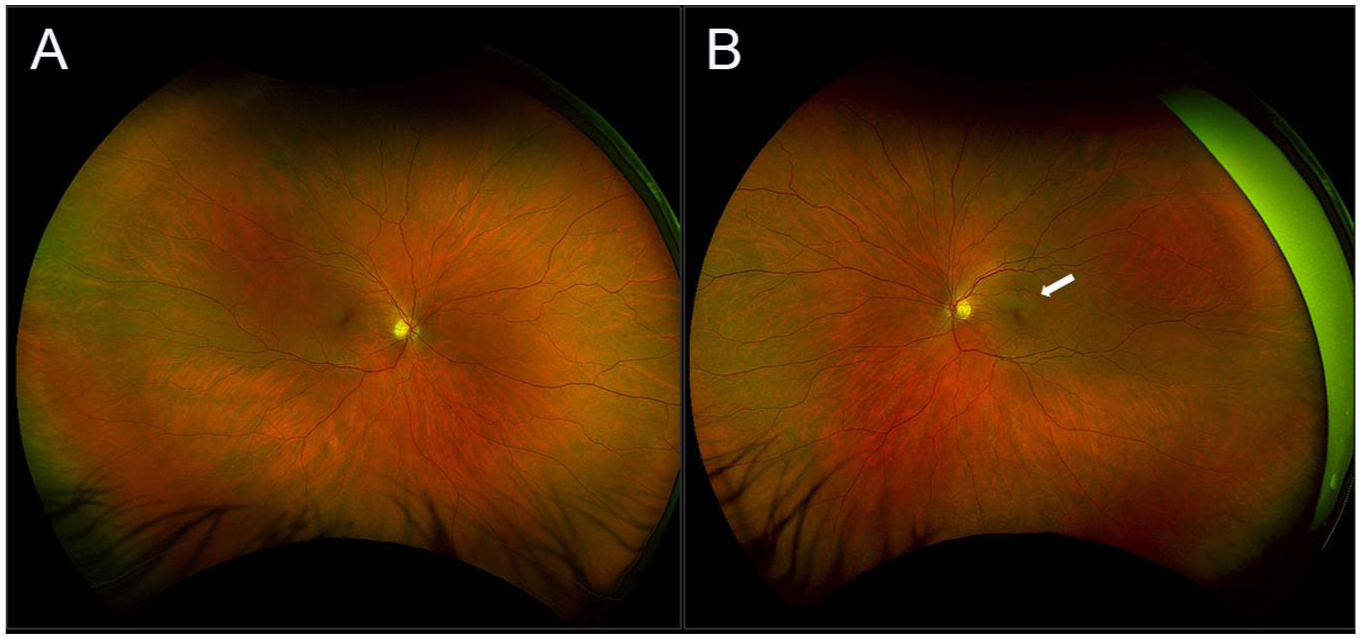
Widefield color fundus image at the time of presentation. The right eye was unremarkable (A). In the left eye (B), there was a pearlescent retinal lesion in the superior parafoveal macula (arrow).
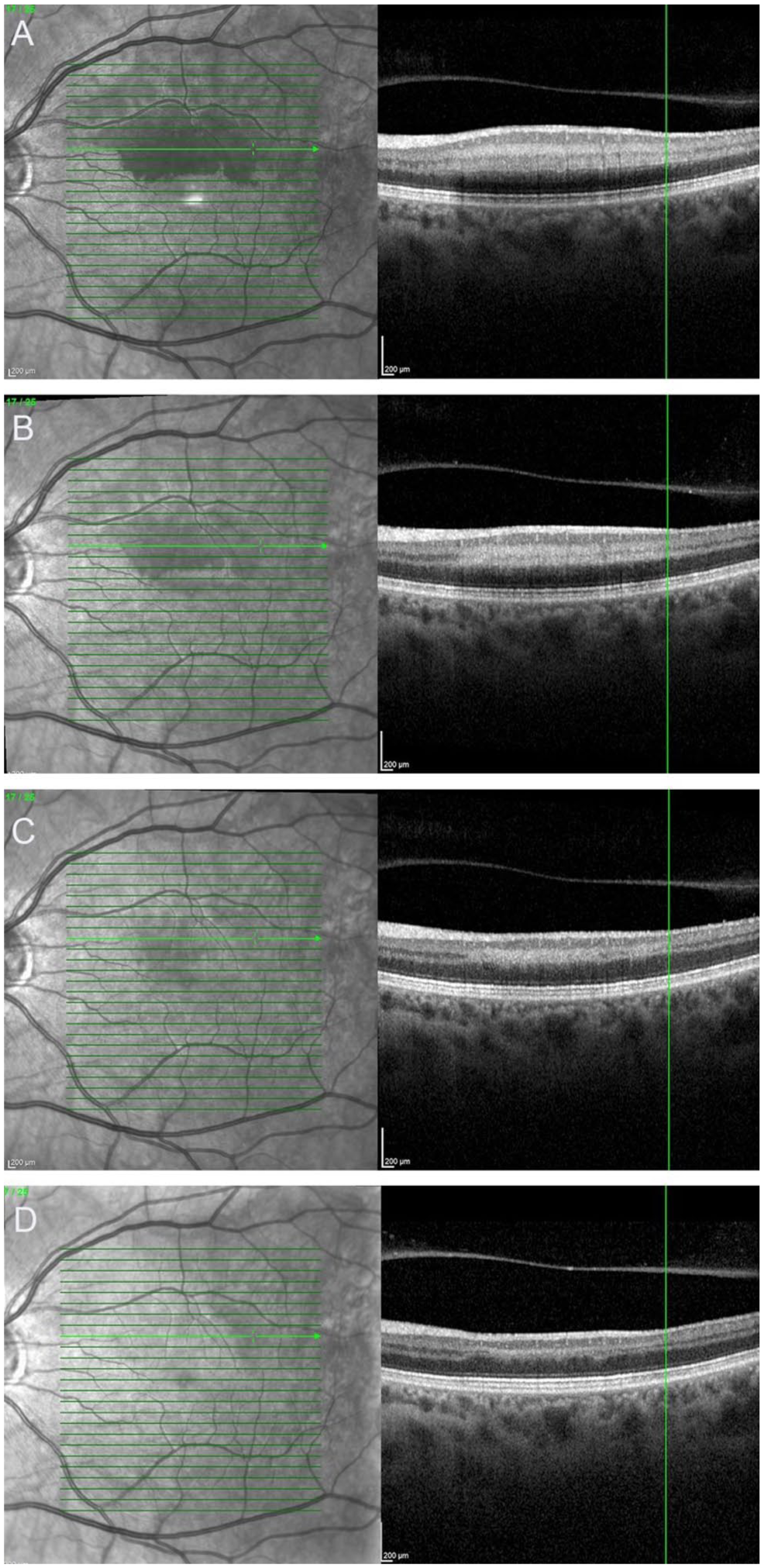
Optical coherence tomography of the left eye on presentation (A) demonstrated a hyporeflective parafoveal lesion on near-infrared and a hyperreflective band extending from the inner plexiform layer to the outer plexiform layer consistent with a paracentral acute middle maculopathy (PAMM) lesion. Follow-up at 5 days (B) and 1 month (C) demonstrated reduction of the hyperreflective PAMM lesion. Upon final follow-up at 4 months (D), there was residual thinning of the inner nuclear layer and irregularity of the inner and outer plexiform layers.
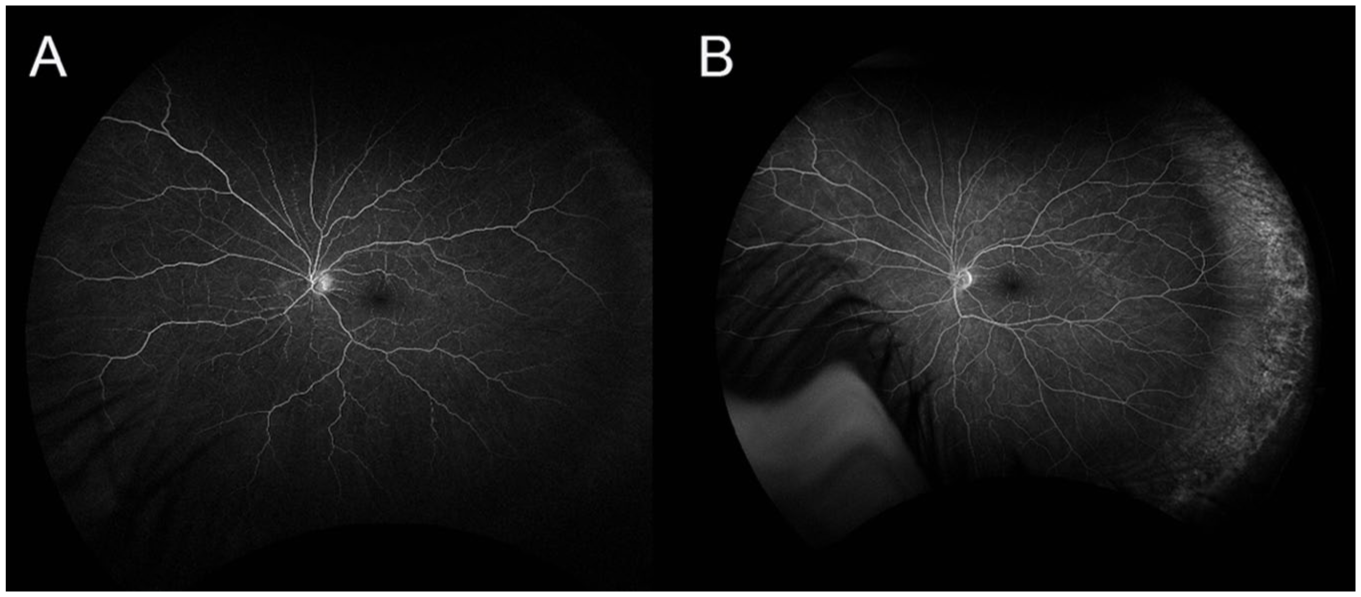
Early-phase (A) and late-phase (B) fluorescein angiography of the left eye on presentation were normal, without evidence of delayed filling, perfusion defects, or leakage.
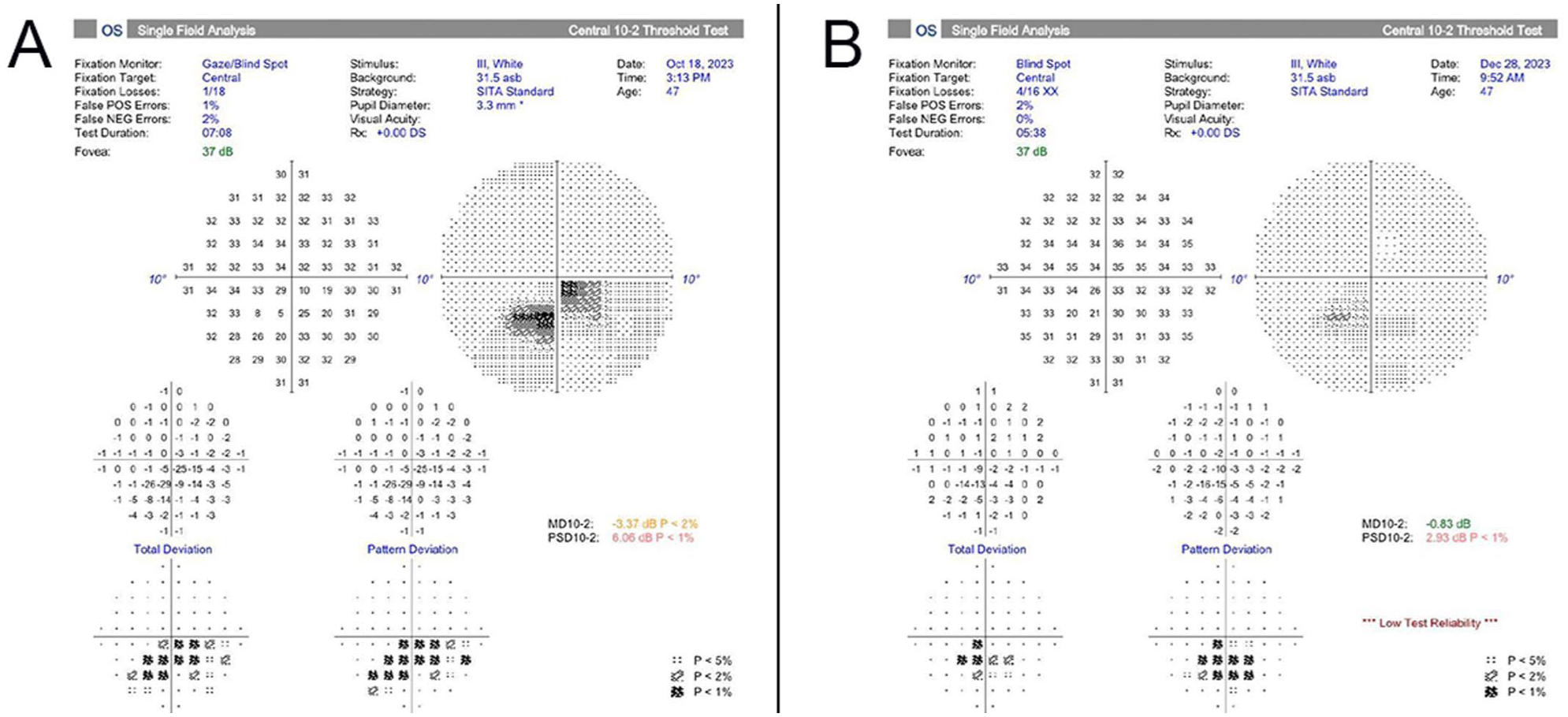
Humphrey visual field 10-2 testing at the time of presentation (A) demonstrated an inferior paracentral scotoma in the left eye that correlated with the patient’s subjective visual symptoms and the superior macular changes seen on optical coherence tomography. At follow-up 2 months later, there was improvement in the visual field defect (B).
A diagnosis of PAMM was made, and the patient was emergently referred to a stroke center. A complete workup revealed mild hypercholesterolemia but was otherwise unremarkable. Electrocardiogram was normal. Computed tomography without contrast excluded mass or stroke. Computed tomography angiogram of the head and neck revealed no significant stenosis of the proximal internal carotid artery bilaterally, nor any obstruction in the vertebrobasilar system. Magnetic resonance imaging of the brain with and without contrast was normal. Additional laboratory tests, including complete blood count, erythrocyte sedimentation rate, prothrombin time, partial thromboplastin time, protein C, protein S, antinuclear antibody, homocysteine, factor V Leiden, fluorescent treponemal antibody-absorption, antithrombin III, anticardiolipin antibodies, lupus anticoagulant, and anti-B2-glycoprotein-I, were unrevealing. Hyperbaric oxygen therapy was recommended by the patient’s otolaryngologist, and she underwent multiple 90-minute sessions of hyperbaric oxygen therapy beginning at 96 hours after symptom onset. Upon follow-up 5 days after diagnosis, examination and OCT demonstrated reduction of the hyperreflective band and retinal thickening (Figure 2, B), and FA remained unremarkable.
At the next follow-up 1 month later, the patient reported improvement in her symptoms, and OCT demonstrated continued reduction of the PAMM lesion (Figure 2, C), which continued to improve at the 2-month follow-up visit. Visual field testing also revealed improvement in the paracentral scotoma at 1 and 2 months after diagnosis (Figure 4, B). At final follow-up 4 months after presentation, the patient reported minimal residual symptoms. On OCT, the hyperreflective acute PAMM lesion had essentially resolved, but resulted in attenuation of the inner nuclear layer (INL) and irregularity of the inner and outer plexiform layers (Figure 2, D).
Discussion
PAMM is characterized by band-like hyperreflective parafoveal lesions at the level of the INL, likely resulting from ischemia of the deep capillary plexus, and to a lesser extent, the intermediate capillary plexus.2–5 The middle retinal layers of the parafoveal macula are a watershed area, where high oxygen demand creates risk for hypoperfusion. 3 Accordingly, OCT angiography has demonstrated areas of capillary dropout in the deep capillary plexus in some eyes with PAMM. 6 Reperfusion injury may also play a role in its etiology. 4 Over time, retinal ischemic perivascular lesions subsequently develop in the same areas as the PAMM lesions, visible on OCT as thinning of the INL. 7
PAMM typically presents with sudden onset of paracentral scotomas with normal or slightly decreased visual acuity. 4 Unfortunately, these scotomas can often be permanent. 7 Fundus examination may appear normal or may reveal deep gray lesions in the macula. 4 The diagnosis of PAMM is typically confirmed by identification of characteristic lesions on OCT. 4 En face OCT has been used to describe several types of PAMM, including perivenular fern-like and diffuse globular patterns. 6 The perivenular fern-like pattern may be associated with milder PAMM lesions, while the globular pattern may reflect more severe disease. 5 FA is typically normal in PAMM, as it is insufficient to image the deep capillary plexus. 3
A variety of conditions causing insufficient blood flow within the deep capillary plexus can lead to PAMM. 1 Retinal vascular occlusions, such as central retinal vein occlusion (CRVO) and central retinal artery occlusion (CRAO), are the most frequently identified cause. 7 Approximately 5% of eyes with CRVO demonstrate evidence of PAMM. 8 In addition, PAMM may be the only visible finding in incomplete CRAO, branch retinal artery occlusion, or incomplete CRVO.1,5,7 PAMM has also been associated with other retinal disorders, including diabetic retinopathy, hypertensive retinopathy, sickle cell retinopathy, Purtscher retinopathy, and retinal vasculitis.3,4 PAMM has also been reported after eye compression injury, excessive caffeine intake, hypovolemia, flu-like illnesses, and cosmetic procedures including, injections of filler. 3 Drugs with vasoconstrictive effects such as sumatriptan and synephrine have also been associated with PAMM. 4
Systemic risk factors may include hypercoagulable states, diabetes mellitus, hypertension, dyslipidemia, carotid arterial disease, migraine, pregnancy, amphetamine abuse, and autoimmune diseases such as systemic lupus erythematosus.1,3,4,7 While our patient had a history of migraines, her presentation with PAMM was not temporally associated with a migrainous episode. Changes in retinal microvasculature in migraine have been hypothesized to increase susceptibility to retinal ischemia; thus, our patient’s history could be considered a predisposing factor.
Finally, PAMM has been reported as a sequel of several different types of surgical procedures. Intra- and extraocular procedures associated with PAMM include intravitreal injections, phacoemulsification, pars plana vitrectomy, and pterygium removal.1,4 In these cases, vasoconstriction secondary to periocular anesthesia may be a contributing factor. 4 PAMM has been reported after vascular surgeries such as aortic aneurysm repair, endovascular coil embolization, and cardiopulmonary bypass. 4 Our case is the first to our knowledge following routine sinus surgery.
The ophthalmic artery, which originates from the internal carotid artery, provides the blood supply of the retina and choroid. The face derives its blood supply from the external carotid artery. Multiple anastomoses occur between these systems, including within the nasal passages at the Kiesselbach plexus. 9 Therefore, unintentional intravascular injection within the nasal passages can create retrograde flow into the ophthalmic artery. In our case, inadvertent intravascular injection of local anesthetic may have led to vasoconstriction of the retinal vasculature and subsequent reperfusion injury.
Weinstein and Greven 9 recently reported a case of PAMM following an intranasal steroid injection. Although there are similarities between this case and ours, there are some key differences. The patient in the report by Weinstein and Greven 9 experienced sudden transient vision loss immediately following the steroid injection, and they presented with PAMM 5 days later. In our case, the patient did not relay any immediate symptoms at the time of the surgery but noted symptoms later in the evening and presented 2 days later. Weinstein and Greven 9 proposed that the etiology in their case was a brief occlusion of the central retinal artery by steroid material that subsequently moved downstream within the retinal vasculature. In contrast, our case was likely due to vasoconstriction secondary to local anesthetic administration. Subsequent reperfusion injury following resolution of the vasoconstrictive effects of the anesthetic may explain the time delay before symptoms developed. The anastomosis between the internal and external carotid systems within the nasal passages was likely a contributing factor in both cases. Strategies to reduce intravascular injection including, the use of smaller gauge needles and aspirating before injecting, may help to avoid this complication. 9
As PAMM may be the only finding of potentially vision- or life-threatening conditions such as cardiovascular disease and giant cell arteritis, an immediate and thorough systemic workup is indicated. 7 In the presence of PAMM without evidence of CRVO, CRAO, or other clear etiology, a diagnosis of incomplete CRAO should be considered, and patients should be referred for an urgent stroke evaluation.5,7
Our patient underwent a complete stroke, hypercoagulable, infectious, and autoimmune workup that was largely unremarkable, further supporting the hypothesis that the preceding sinus surgery was likely the triggering factor. 10 In our case, the patient’s treating head and neck surgeon referred the patient for hyperbaric oxygen therapy, and she received 5 sessions of this treatment. Hyperbaric oxygen therapy may provide some benefit in the treatment of CRAO and is generally thought to be low risk. 11 Fortunately, our patient had a good outcome with improvement of the scotoma in the left eye.
This case demonstrates that PAMM is a possible rare complication of sinus surgery, conceivably due to the vasoconstrictive effects of local anesthetics. This diagnosis should be considered in the setting of acute vision loss following sinus procedures. In the absence of a clear etiology for PAMM, an urgent stroke evaluation should be performed due to the risk of potentially vision- or life-threatening conditions.
Footnotes
Author Contributions
Each author contributed materially to the writing and review of the final manuscript.
Ethical Approval
The Institutional Review Board for the Retina Group of Washington approved this study. We received approval from WCG Clinical. IRB number 1-1699888-1.
Statement of Informed Consent
The patient gave full informed consent for participation in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.