
Abstract
Purpose:
The purpose of this case series is to report 5 new cases of ocular venous air embolism (OVAE). We define OVAE as a precipitous drop in end-tidal carbon dioxide, a choroidal detachment, or a choroidal wound, followed by signs of impending or actual cardiovascular collapse, during vitrectomy air infusion.
Methods:
A case report series was retrospectively reviewed.
Results:
Four of the 5 OVAE cases (80%) were fatal, occurring in conjunction with repair of rhegmatogenous retinal detachment (2 cases); a large surgical wound of the choroid (1 case); and vitrectomy repair of an injured eye (1 case). One patient survived OVAE during choroidal melanoma endoresection after prompt discontinuance of air infusion by anesthesia personnel previously alerted to the OVAE risk.
Conclusions:
OVAE is a rare but usually fatal complication of air infusion into the eye during vitrectomy. Because the effective response time to avoid a fatal OVAE outcome can be less than 1 minute, use of preventive measures is critical.
Keywords
Introduction
Since the early 19th century it has been known that entrainment (embolization) of air into blood vessels can cause injury or death. 1 Usually this occurs during surgery, and into the venous system (venous air embolism, VAE). 2 Much of the credit for our modern knowledge of VAE is owed to Maurice S. Albin, MD, a recently deceased coauthor of this report, who helped lead our investigations. 2 Sufficiently rapid entrainment of as little as 200 cc of air has been reported to be fatal in humans. 2,3
Anesthesiologist Thomas Ledowski and colleagues authored the first report of “possible” ocular venous air embolism (OVAE) during a (pars plana) vitrectomy performed in 2005. 4 The operating vitreoretinal surgeon noted choroidal detachment (likely from suprachoroidal air infusion through a slipped cannula, see Figure 1) after starting air infusion for retinal reattachment. Ledowski then noted a sudden decrease in peripheral oxygenation, blood pressure, and end-tidal carbon dioxide (ETCO2), followed within 1 minute by a “mill-wheel” murmur 2 —signs commonly recognized by anesthesia personnel as indicating air embolism—and after discontinuance of vitrectomy air infusion the patient recovered. A small, retrobulbar air bubble was then seen in the orbit on postoperative computed tomography scans.
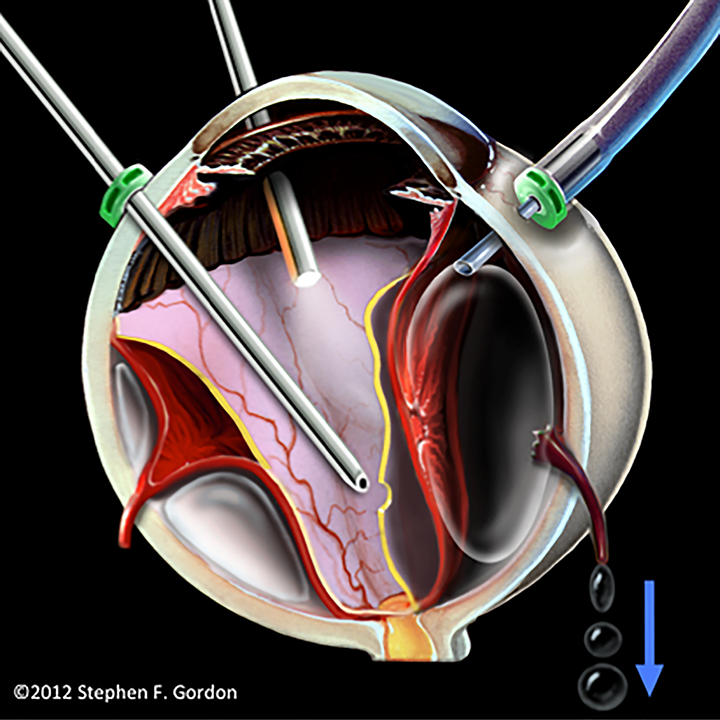
Artist’s illustration of a slipped infusion cannula causing accidental suprachoroidal air infusion. The expanding bubble tears 1 or more vortex veins, leading to ocular venous air embolism. (Reprinted with permission of the British Journal of Ophthalmology. 14 )
We define OVAE clinically as a precipitous drop in ETCO2, a choroidal detachment, or a choroidal wound, followed by signs of impending or actual cardiovascular collapse, during vitrectomy air infusion. Eight cases (5 fatal) of OVAE have thus far been reported. 4 -11 We now describe 5 heretofore unreported OVAE cases (4 fatal), with 1 fatal case occurring in the early 1990s.
Materials and Methods
To find unreported cases, we queried (with permission from the American Society of Anesthesiologists [ASA], Schaumburg, IL) the ASA Closed Claims database for vitrectomy complications during the period from 1970 through 2018. We also had discussions at several meetings of the American Society of Retina Specialists and the Ophthalmic Anesthesia Society, and communicated with authors of OVAE reports. Upon hearing of our study, an anesthetist sister of an OVAE decedent also brought 1 case to our attention.
Case Reports
Five cases of OVAE are presented here chronologically in Table 1, followed by individual, narrative reports of Cases 3 through 5 that illustrate the most common scenarios giving rise to OVAE.
Chronological Description of 5 New OVAE Cases.
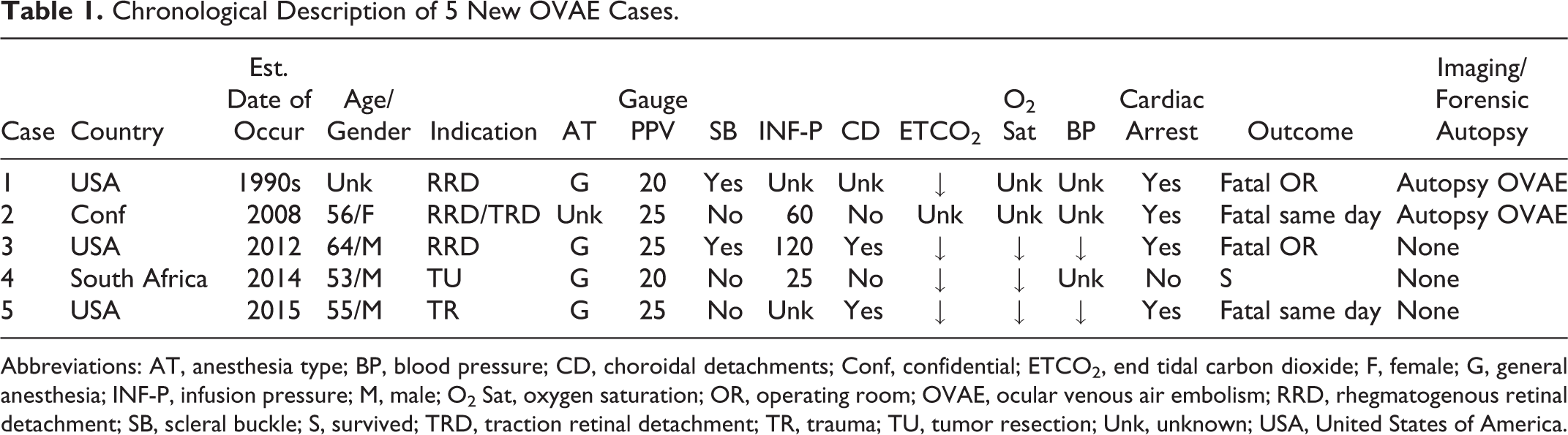
Abbreviations: AT, anesthesia type; BP, blood pressure; CD, choroidal detachments; Conf, confidential; ETCO2, end tidal carbon dioxide; F, female; G, general anesthesia; INF-P, infusion pressure; M, male; O2 Sat, oxygen saturation; OR, operating room; OVAE, ocular venous air embolism; RRD, rhegmatogenous retinal detachment; SB, scleral buckle; S, survived; TRD, traction retinal detachment; TR, trauma; TU, tumor resection; Unk, unknown; USA, United States of America.
Case 3: Retinal Detachment Repair
A 64-year-old, ASA III male patient presented for repair of rhegmatogenous retinal detachment (RRD) by 25-gauge (G) vitrectomy and scleral buckling. General anesthesia was maintained via a laryngeal mask airway and pressure support ventilation was utilized.
In preparation for an encircling scleral buckle, the conjunctiva was incised 360° and the rectus muscles were isolated and placed on traction sutures. Vitrectomy was then performed with an unsutured, 25G infusion cannula. With the working cannulae closed and still using liquid infusion, the eye was rotated with the traction sutures, sequentially exposing each quadrant of the eye to suture an encircling band to the sclera.
The eye was reentered with fiberoptic and cautery probes and the retina was marked at a site chosen for internal drainage of subretinal fluid. A finger-controlled outflow needle was then inserted. Infusion was changed from liquid to air and as subretinal fluid drainage began, increasing choroidal “effusion” was noted.
The air infusion pressure was rapidly increased stepwise to the maximum vitrectomy console level of 120 mm Hg before the infusion line was ultimately pulled from the eye, and a new infusion line was ordered. But within an estimated 1 minute of having reached maximum infusion pressure, a precipitous decrease in ETCO2 followed and the anesthetist announced impending cardiovascular collapse that quickly progressed to cardiac arrest. The surgeon voiced the possibility of air embolism. Upon removal of the surgical drapes to enable cardiopulmonary resuscitation, the patient was noted to be blue from the neck up. This persisted during 50 minutes of resuscitative efforts, using the Advanced Cardiac Life Support protocol, that were ultimately unsuccessful.
An autopsy performed 21 hours after death showed no coronary artery occlusion and no thromboembolism. But postmortem imaging and a forensic autopsy specifically to discover air embolism, 12,13 including opening the heart under water, were not performed. The operated eye was not examined to establish detachment of the choroid and torn vortex venous outflow. Serial sections of lung tissue showed congestion, and subsequent histologic examination of lung parenchyma showed “empty vessels…possibly representing air.”
The pathologist concluded that VAE was a “distinct diagnostic possibility”; however, the autopsy findings could not establish “with reasonable certainty” that air embolism caused the sudden death. No other cause of death was found. Two anesthesiologists who oversaw the resuscitative effort ultimately did conclude that massive air embolism was the cause of death. However, absent forensic autopsy confirmation of air embolism, eye surgeons conducting a mortality conference could not reach a consensus opinion as to the probable cause of death.
Case 4: Endoresection of Choroidal Melanoma
A healthy 53-year-old male underwent endoresection of a choroidal melanoma by 20G vitrectomy under general anesthesia without nitrous oxide. Significant choroidal bleeding occurred as the tumor was resected. To improve the surgical view the procedure was continued under air infusion of 25 mm Hg. During this time, the anesthesia personnel were aware of the possibility of OVAE. After approximately 15 minutes of working under air infusion, a drop in ETCO2 occurred followed by a drop in peripheral capillary oxygen saturation (SpO2).
The anesthesiologist documented the presence of a mill-wheel murmur. Air infusion was stopped and the vitreous cavity was filled with silicone oil. The patient’s ETCO2 and SpO2 recovered steadily and the murmur resolved. He then made a full and uneventful recovery.
Case 5: Trauma
A healthy 55-year-old male underwent primary repair of an open globe injury under uneventful general anesthesia. Three weeks later he was admitted to an ambulatory surgery center for vitrectomy to remove vitreous hemorrhage and to repair retinal and choroidal detachments, again under general anesthesia. A 25G vitrectomy was performed using an unsutured infusion cannula. As air infusion was initiated, the ETCO2 fell from 47 to 13 and remained depressed for the duration of the operation. The heart rate fell from 70 to 40 and blood pressure initially dropped to the 60s systolic and then returned to normal with multiple doses of phenylephrine.
The arterial blood gas (ABG) revealed: pH 7.13, partial pressure (Pa)CO2 50, and PaO2 65 on 100% oxygen. Infusion of silicone oil was performed and surgery was concluded. The patient “awakened” and was extubated prior to transfer to an affiliated general hospital. Follow-up ABGs remained very poor on 100% oxygen over the next 4 hours. The patient was then intubated with difficulty. Eight hours later the patient had cardiac arrest with pulseless electrical activity from which he could not be resuscitated.
Discussion
OVAE can occur during vitrectomy when air infused under pressure enters intact vortex veins through large surgical or traumatic choroidal wounds, as in vitrectomy for resection of choroidal melanoma or repair of eye injury (see Cases 4 and 5). 6,7 But these are relatively rare cases in which the OVAE risk is now foreseeable and thus manageable.
A more insidious OVAE threat is the risk during any vitrectomy air infusion of a slipped, unsutured cannula causing air entrainment through vortex veins torn by an expanding suprachoroidal bubble (Figure 1). 14 This scenario likely occurred in the Ledowski case and in Case 3, during which choroidal detachment was also noted immediately after beginning air infusion. The life-or-death difference in these cases was the decision to increase air infusion pressure as an immediate response to choroidal detachment in Case 3, resulting in the first known instance of an OVAE intraoperative fatality. Similar fatal outcomes following choroidal detachment with subsequent pressure increase were reported in 2014 and 2017. 9,11
Persistent blue discoloration of the head (cephalic cyanosis) during attempted resuscitation in Case 3 gives credence to a single, massive air embolus, entrained under very high pressure, internally blocking all venous return from the head. 15,16 Cephalic cyanosis is also seen in hanging deaths, when jugular veins are occluded by external means. 17 In the autopsy-proven absence of any thrombotic obstruction in an OVAE decedent, persistent cephalic cyanosis antemortem may thus be diagnostic for such a large air embolism (Figure 2). Noncontinuous, but still life-threatening embolization, without blockage of venous return from the head, is more common as lower infusion pressures are used in most OVAE cases.
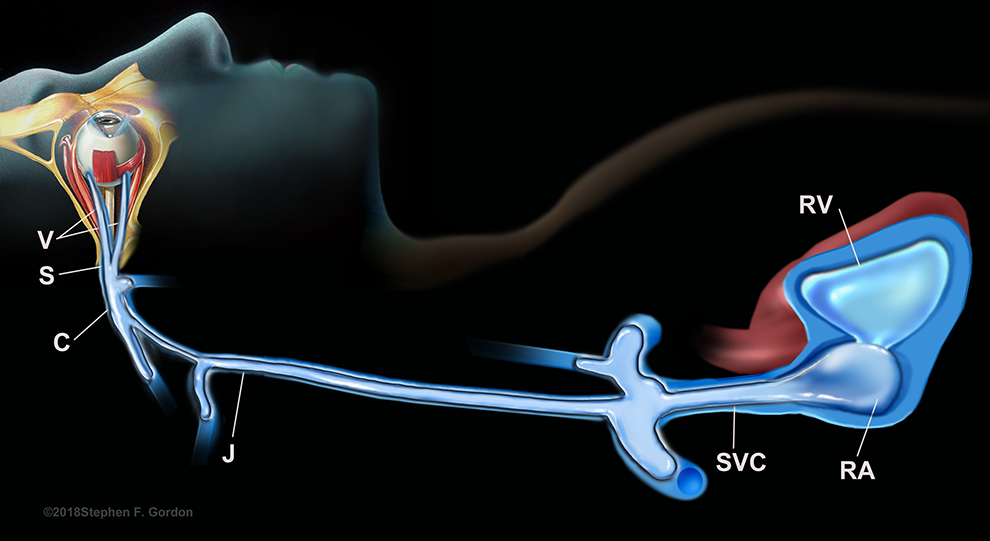
Depiction of the concept of cephalic cyanosis resulting from ocular venous air embolism. A single, massive air embolism, under very high pressure, filling the ipsilateral jugular vein, the innominate veins (blocking the contralateral jugular vein), and the superior vena cava—blocking all venous return from the head and causing the persistent “blue head” appearance noted upon drape removal (Case 3). CS indicates cavernous sinus; J, jugular vein; RA, right atrium; SVC, superior vena cava; V, vortex vein. (Reprinted with permission of artist Stephen F. Gordon ©2018.)
Conclusion
The existence of life-threatening OVAE has been proven experimentally,
10,14,18,19
and experienced clinically on multiple occasions, as shown here. Vitreoretinal surgeons must be aware of this potentially fatal complication of air infusion, and should take the following steps to prevent it: Prior to any vitrectomy air-fluid exchange, perform a brief vitrectomy team “time out” to reconfirm infusion cannula positioning into the vitreous cavity; stop infusion immediately if a choroidal detachment is noticed during air infusion; perform any combined vitrectomy and scleral buckling with a secured infusion cannula; and use a precordial Doppler monitor and alert the anesthesia team during air infusion in known high-risk cases of choroidal melanoma endoresection, posterior segment trauma with large uveal tract wounds, or intentional choroidotomy.
2,20
Footnotes
Authors' Note
None of the authors participated in any cases included in this article.
Acknowledgments
The authors are grateful to Christina Sullivan, Jessica Haynes, C. Dianne Scharper, Stephen Gordon, Stephanie Hill, and Stephanie Casterline for their assistance in this work. This article is dedicated to the memory of those who lost their lives to the OVAE complication.
Ethical Approval
This study was approved by the University of Alabama at Birmingham Institutional Review Board for Human Use and is in accordance with the Declaration of Helsinki.
Statement of Informed Consent
Because of the retrospective nature of the study, and because all data collection and analysis were performed without patient identifiers, informed consent was waived.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.