
Abstract
Introduction:
Many digital tools are available to support healthy pregnancies. Far fewer focus on the postpartum period or have the explicit goal of reducing poor or inequitable maternal health outcomes. Yet, many pregnancy-related complications occur up to a year after labor and delivery. Here, we outline a healthequity-centered process, using multiple phases of data collection, which informed our design decisions when developing a comprehensive postpartum support app, Myana (“Mothers, you are not alone”).
Methods:
Drawing on a behavioral decision research approach and grounded in principles for developing equity-focused digital reproductive health tools, we iteratively designed and tested the Myana app. Our data collection included qualitative interviews, focus groups, and evaluations of an interactive experience prototype and app wireframes.
Results:
To illustrate our process, we highlight two unique features of Myana intended to address health inequities: a symptom triaging feature (“The Healing Check-in”) and a tailored educational hub (“The Learning Center”). Results from our iterative development process shaped how we asked about and responded to symptoms reported in the Healing Check-in, the topics and framing of curated content in the Learning Center, the cadence of expected interaction with features in the app, as well as the app’s overall tone and visual design.
Discussion:
We created a postpartum support app to help birthing parents make informed decisions about their health and well-being in the year postpartum, with the larger goal of improving health outcomes. The iterative design and development process integrated clinical and community perspectives while intentionally centering health disparities. This approach represents a new model for developing digital supports to supplement the formal healthcare system.
Keywords
Introduction
In the United States, many maternal deaths occur after hospital discharge following pregnancies and deliveries that appeared uncomplicated, with over 80% of deaths being deemed preventable upon review. 1 These deaths primarily occur in the 6 weeks following birth, before most birthing parents return for their routine post-delivery check-up. 2 Black and Brown birthing parents and their infants experience mortality and severe morbidity at disproportionately high rates in the year after delivery, highlighting a maternal–child health equity crisis that is driven, in part, by unequal access to information, opportunity, and high-quality health care.3–5
Digital tools are a scalable way of enhancing connection with birthing parents, providing an opportunity to meet informational needs and link them to resources.6,7 By offering remote monitoring and facilitating opportunities to re-engage with the healthcare system after birth, digital tools can also help close gaps in care, particularly for those living in areas with limited or no access to obstetric or maternity care services. 8 To effectively address health inequities, however, these tools must simultaneously serve the needs of multiple stakeholders. For such tools to be promoted by health care providers, they must adhere to clinical best practice guidelines and offer screenings or services perceived as useful. For birthing parents, tools must be engaging by offering content that is meaningful, culturally relevant, and easy to apply in the context of their lives.9,10 For policymakers, such tools will only be relevant if they can directly or indirectly address pressing public health problems.
Here, we describe the design and development process of a comprehensive postpartum support app, Myana (“Mothers, you are not alone”), centering the needs of the groups critical for its adoption and dissemination.
Methods
Theoretical approach
To iteratively inform the creation of the Myana app, we applied a behavioral decision research paradigm11–15 to an equity-focused framework for digital tool development.16,17 This research approach consists of an analytical step, in which the best available medical knowledge guides the information and functionality presented to end-users of the app. It also incorporates descriptive research, to characterize the end-users’ (birthing parents’) beliefs, values, and needs. Together, this forms the basis of the design and evaluation of a prescriptive mobile health (mHealth) intervention, with the goal of closing the loop between the lived reality of the app users and the knowledge and resources needed to make informed decisions about their health. Lastly, evaluative research must be routinely implemented to ensure that the intended goal of the app is being realized. Here, we apply this approach iteratively to produce the final app design (prescriptive intervention). Importantly, each design phase targets critical health care gaps for birthing parents from sociodemographic groups experiencing health disparities. Throughout, we produced revised versions of the app’s visual design and functionality. These versions allowed us to evaluate emergent and varied aspects of the design. 18 Figure 1 outlines the process. Using diverse examples of the app’s functionality, we offer concrete ways in which this approach can be applied to design decisions for other evidence-based digital health supports.
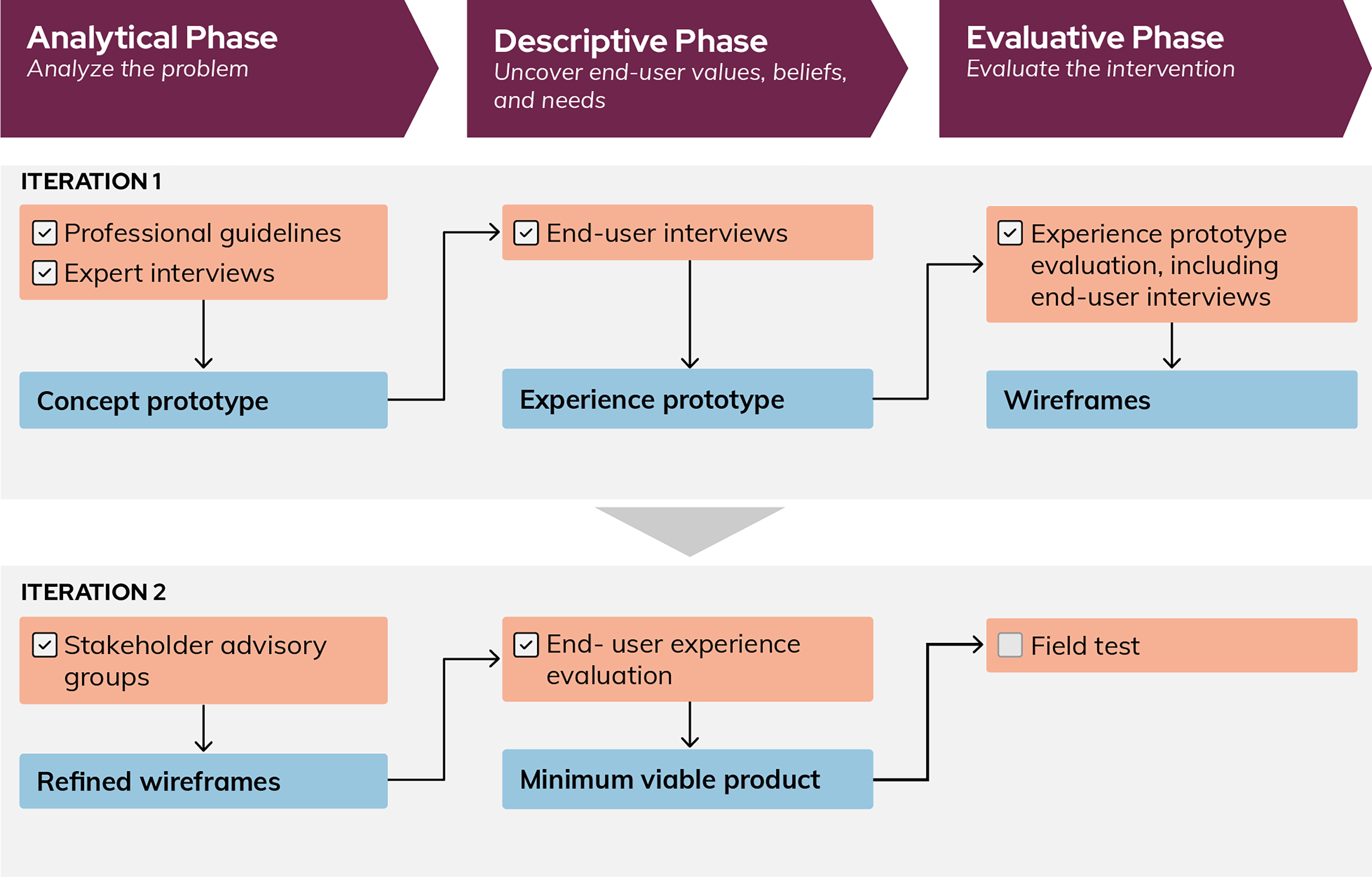
Design and development approach for the creation of a postpartum support app. The purple boxes describe the overarching design and development phases of creating a postpartum support app. Each iteration of the tool, shown in gray rectangles, details the methods of user inputs, both analytical and descriptive, (orange) and the design outputs, which are prescriptive (blue).
Participant recruitment and data collection
Iteration 1
Analytical phase
Our first analytical phase used 60-minute qualitative interviews with (n = 6) domain experts to identify gaps in postpartum care, including the clinical information and tools most needed to redress inequities in maternal health outcomes. We recruited experts from a large academic medical center and community-based care delivery organizations (STUDY20090191). Experts were purposively sampled for variation in credentials and specialized knowledge in health equity or postpartum conditions in which health disparities are prevalent (e.g., hypertensive disorders of pregnancy). All experts were active providers for postpartum patients and included family medicine and maternal–fetal medicine physicians, a nursing director of women’s health operations for a labor and delivery hospital, and the CEO of a regional Healthy Start. The interviews were centered on gaps in postpartum care and opportunities for how a postpartum support app could help meet the clinical needs of birthing parents. Interviews were recorded and transcribed. Rapid qualitative analysis methods were applied to synthesize the data. 19 These interviews were the primary drivers for a concept prototype (a relatively small number of high-fidelity screen sintended to convey the overaching functionality and design of the app).
Descriptive phase
We then gathered lived expertise through 90-minute qualitative interviews with birthing parents. Participants (n = 8) were recruited in-person while attending postpartum care at a local women’s health clinic, on social media platforms hosted by local community health organizations, and through Pitt + Me, a research registry in Western Pennsylvania operated by the University of Pittsburgh (STUDY21070134). Adults who had given birth within the past 12 months were eligible. Enrolled participants were asked questions about their physical recovery, support resources, and interactions with their health care team. They were then shown the concept prototype of Myana. Participants were asked to comment on features, topics, and visual design, offering perspectives based on their own postpartum care experiences and preferences. An affinity mapping technique20,21 was applied to synthesize the descriptive feedback from birthing parents. In affinity mapping, researchers take independent notes and jointly analyze the data, building a diagram. Here, two researchers (A.D., R.O.) built an affinity diagram to identify specific design and functionality features that would be responsive to birthing parents’ needs and desires, while still addressing the expert priorities identified in the concept prototype. These features were then incorporated into an experience prototype. The experience prototype is a realistic simulation of the app, built with off-the-shelf software tools, that allows the app to be interactively tested on a phone or laptop by birthing parents.
Evaluative phase
Evaluation of the experience prototype was then conducted with new birthing parents. Birthing parents were recruited in-person by clinical research staff at a prenatal appointment in their third trimester or during their postpartum inpatient stay at the main birthing hospital in Pittsburgh, Pennsylvania (STUDY22020017). Participants were eligible if they were at least 18 years of age, in the third trimester of their pregnancy, or had a live delivery in the past 48 hours at the hospital study recruitment site. All participants were enrolled at the delivery site (n = 15, with one participant later withdrawing). Participants were provided with an account to access the prototype and a video camera to take home. For the duration of the study, participants received daily text notifications, with a corresponding link to the web-based experience prototype. The link led the participant to a daily topic screen offering information related to health and healing that was specific to the postpartum day (e.g., Day 4 provided information on “Pain and Healing”). Participants could access the full Learning Center content, which offered 6 weeks of postpartum content, at any time. They were also able to complete the Healing Check-in daily to assess potential postpartum risks. Participants recorded six weekly video reflections and completed semi-structured interviews at 3 and 6 weeks’ postpartum. We asked them to describe how well the prototype integrated into their daily postpartum lives. An ethnographic analysis of the methods and findings of the experience prototype testing can be found in a prior publication. 22 Daily use patterns (e.g., time of day, elements most frequently engaged with), participant ratings of features, and rapid thematic synthesis across the videos and interviews were then used to inform the Myana wireframes. Wireframes are comprehensive, blueprint-like representations of all screen types in an app and intended to specify details of the underlying structures and workflows. An accompanying logic document was drafted to detail how and when the content shown on the app screens should be surfaced to the app user.
Iteration 2
Analytical phase
The wireframes were then refined with expert input through two stakeholder advisory group meetings (Summer 2023, n = 16; Spring 2024, n = 8). Members were strategically recruited through direct outreach from the research team to represent diverse organizations and perspectives that may ultimately disseminate or promote the tool. These included representatives from health care settings, city- and state-level public health departments, and those with lived experience (STUDY2209015). In the first meeting, advisory group members were oriented to the project and asked to review the Myana wireframes, with the goal of addressing key questions related to features of the tool and benefits and barriers for future users. In the second meeting, the research team conducted a collaborative human-centered design session with a subset of the members to generate ideas about how to engage users while being sensitive to their needs. Members were asked to brainstorm topics and questions served to app users to facilitate connection and support. For example, one member recommended an article on postpartum anxiety to address a common knowledge gap.
Descriptive phase
Lastly, user experience (UX) evaluation sessions were conducted with birthing parents (n = 15). Participants were recruited via posts on monitored online parenting groups and in person by clinical research staff at the main birthing hospital in Pittsburgh, Pennsylvania (STUDY22090151). Adults who had given birth within the past 12 months were eligible. UX participants were shown the refined wireframes and were asked to think aloud as they interacted with the features in Myana (e.g., Can you imagine yourself using something like this Healing Check-in in those early weeks of recovery?”). Rapid qualitative analysis methods were used to synthesize feedback. Wireframes were then refined and paired with a revised backend app logic document to produce a minimum viable product (a downloadable app with all core features and functionality built for field testing).
Ethical considerations
Each phase of this work was reviewed and approved by the University of Pittsburgh Institutional Review Board. We adhered to relevant Standards for Reporting Qualitative Research guidelines 23 for synthesized research in a methods paper. Participants in each study were compensated for their time. Participants in the experience prototype evaluation were informed that Myana was not a substitute for medical advice. Across all qualitative data collection phases, resources were made available on the sensitive postpartum topics raised (e.g., depression and local counseling resources) to participants who desired them. This research approach employed a triangulation of data sources across research phases. The iterative nature of the work allowed individuals with lived experience to verify that interpretations from each prior design decision accurately reflected their experiences and priorities.
Researcher positionality
Research team members who engaged directly in data collection activities with participants have diverse backgrounds and qualitative expertise. The senior author (T.K.) has a doctoral degree in behavioral decision research and significant mixed methods research experience. The lead author (S.K.B.) has qualitative research experience and human-centered design training. Two authors (A.D. and R.O.) are design professionals with extensive training in user-centered methodology for digital product design. Three of the four have direct lived experience of pregnancy, birthing, and parenthood. The clinical priorities of the team could introduce bias in the perspectives and subsequent design changes that were emphasized here. The inherently iterative process described should help address the risk of this bias.
Results
Specific feature development
While the methods outlined above informed all features and content provided in the Myana app, here we present results related to two core functionalities of Myana: (1) an acute maternal symptom tracker (“The Healing Check-in”) and (2) a tailored education hub (“The Learning Center”). We focus on these features because they were proactively designed to improve health outcomes by addressing areas of health disparity.
The pregnancy-related complications that happen post-labor and delivery predominantly occur in the first 6 weeks following birth. 2 Myana’s Healing Check-in was designed to help birthing parents track and triage postpartum symptoms and identify acute warning signs during this critical period. While digital information related to pregnancy and the postpartum period is prevalent, 24 the quality and reliability of information varies, and many digital resources are insufficient in addressing the clinical and cultural needs of those facing the greatest disparities in outcomes. 25
Myana’s Learning Center was designed to offer ongoing guidance for postpartum healing, self-care, baby care, and positive parenting during the first year after birth. The goal of this feature is to proactively address disparities through provision of relevant content to support informed decision making at critical timepoints (e.g., infant vaccination) and to ensure access to appropriate resources. The Learning Center’s content is specifically served to the app user at relevant timepoints in their postpartum experience via a drip-feed of topics, which change daily.
Design phases
Iteration 1
Analytical phase
In domain expert interviews (n = 6, Table 1), a need was voiced for a way to track postpartum symptoms that could prompt earlier and more frequent contact with health care providers after birth, emphasizing that the current structure of postpartum care (one visit at 6 weeks postpartum) is not designed for those with fewer resources or support networks. As one clinician noted, warning signs for acute events need to be routinely queried because they may be easy to miss:
Domain Expert and Stakeholder Advisory Group Member Affiliations

“Headache, chest pain, visual changes, high blood pressure, and depression. These are the things that [postpartum patients] will not call about, and they will not recognize because they can be explained away by other things.” (Exp1)
Similarly, domain experts identified the need for Black birthing individuals to have greater access to equitable treatment for these acute events: “Black people are more likely to be diagnosed late and at a more severe point, when treatment becomes harder, when the situation becomes more dire, and we’re more likely to die from complications of all of these things, so I think we need to look less at how women can advocate for themselves, and more so at ‘where is the gap’ in what they’re getting from the medical community.” (Exp2)
The consensus on a need for early and routine tracking of postpartum symptoms informed the initial functionality of the daily Healing Check-in. Existing professional guidelines were used to inform which specific symptoms would be assessed in a Healing Check-in for the first 6 weeks of a user’s postpartum recovery and expert feedback shaped the appropriate in-app response once those symptoms were reported by an app user. 26 The symptom and response logic was then 26 iterated upon by Maternal–Fetal Medicine physicians on the team.
All domain experts additionally raised the need for ongoing education and connection to resources to support birthing individuals beyond addressing acute symptoms, and noted the importance of opportunities for education when equitable care is lacking: “One of the things that we deal with is sometimes people don’t know what they don’t know, and everybody doesn’t get the same level of treatment and education, and so…I think that the providers have a responsibility to give everyone the same level of education, whether or not they know what questions to ask.” (Exp2)
We synthesized professional guidelines26–30 and our expert interviews to identify critical postpartum needs and areas of health disparity for Black and Brown birthing parents (e.g., postpartum hemorrhage, 31 hypertension 32 ). These topics were then categorized into 13 content domains (Table 2), which formed the initial basis for the Learning Center. At this stage, the design team created a concept prototype, incorporating the expert-informed content and logic for these two features (Fig. 2).

Concept prototype from iteration 1. The concept prototype from iteration 1 details the initial screens showing
Initial Guideline Informed Content to Include in Our Myana Learning Center

Descriptive phase
During concept prototype end-user interviews, birthing parents (n = 8, Table 3) expressed interest in the Healing Check-in and noted that it would be a welcome addition to a postpartum app. They expressed the desire for specific and straightforward results. For example, one individual shared, “I like the symptom check-in. [If] it’s ‘normal’, or ‘call your doctor,’ [you] don’t have to sit there and stress.”
Demographics of Birthing Parent Participants (n = 37) from Multiple Design Phases

not mutually exclusive.
There was also consensus that the Healing Check-in could be more personalized to the birth experience of the individual app user. For example, one participant explained, “It would be nice to have an app that would tell you what to expect depending on the mode of delivery.” From these results, the Healing Check-in was subsequently tailored to users based on delivery type (e.g., vaginal or cesarean delivery) and when the user takes the assessment. For example, content about incision healing, vaginal tears, and pain were tailored to delivery type and a question about bowel and bladder symptoms was redesigned to surface only when the user reaches 3 weeks postpartum, as it is not clinically relevant to monitor those symptoms sooner.
Birthing parents also described the many channels of information they used to answer their postpartum question, including personal networks, care teams, social media, or the internet. Generally, participants favored the topics included in the prototype because of their approachability and easy access: “I love a lot of the articles that are in there because I would know they aren’t on Google, where you can find whatever you want. [Learning Center articles] are based in fact. I don’t have to find them, they are right there.”
In addition to content related to physical recovery and postpartum healing, participants expressed a desire to be seen as more than “just patients.” They voiced a need for the Learning Center content to acknowledge aspects of their experience beyond the clinical and physical, and for the content to address things like “the stress of dealing with your parents or your in-laws or your partners, or feelings of comparison, or feelings about guilt.”
We revised the Learning Center to serve daily, tailored content based on birthing parents’ experience of the topics most critical to them at specific postpartum time points. The full library of content was also expanded (e.g., adapting to relationship changes in the postpartum period, adjusting to parenthood, and providing more information about self-care and mental health) and reorganized by postpartum theme to accommodate birthing parents’ desire to delve deeper into a topic of interest.
Evaluative phase
The experience prototype that incorporated the above changes was then evaluated with new birthing parents (n = 14, Table 3). During the experience prototype evaluation, the Healing Check-in was rated as one of the most desirable features in the app. Participants reported that completing the symptom tracker gave them a moment to pause and gauge their own health at a time when attention is largely focused on the infant. As one participant said: “[The Healing Check-in] definitely helps me pay attention with what’s going on with my body.”
The inclusion of a wider range of content in the Learning Center also resonated with participants. However, they expressed interest in further personalizing educational articles to their individual birthing experience. For example, one participant suggested surfacing articles tailored to “‘vaginal vs. C-Section [births]' so that the topics could be more focused on what I’m experiencing. Also, ‘breastfeeding' or ‘bottle’ or ‘both.’”
While participants voiced explicit appreciation that Myana was focused on their own health and healing, some participants shared that their partner also used the app to understand postpartum healing and there was a consensus among users that more information about the baby was desirable. One participant described their experience of interacting with the daily topic content: “There was a question about ‘is there anything else that you’re interested in [learning about today]?’ I kept putting in whatever the problem was with the baby—how to deal with overtired baby, how to deal with gassy baby… I think that it is a good thing that this is an app that is just focused on mom… . But nuggets about baby could be helpful for mom’s mental health.”
The experience prototype evaluation led us to adjust the content cadence and focus: users would be notified of a new daily topic for the first 6 weeks, gradually transitioning to weekly topics by month 4 with infant content layered in. Articles were also updated to include sections that provided information tailored to birthing experiences, for example, normal healing trajectory tailored to a vaginal delivery versus cesarean delivery or postpartum adjustment expectations for those with a child in the neonatal intensive care unit. Figure 3 illustrates sample screens from the resulting wireframes informed by the experience prototype evaluation.

Wireframes. The wireframes informed by the experience prototype evaluation show the
Iteration 2
Analytical phase
With the degree of content and logic revisions that had been made to the experience prototype, a second analytical review was necessary. In our second round of expert feedback, we convened a stakeholder advisory group of (n = 20, Table 1) clinical professionals, lived experience experts, and public health officials focused on health equity initiatives. Advisory group members reviewed wireframes that fully specified the app’s functionality. In reviewing the Healing Check-in, feedback was overwhelmingly positive and no revisions were deemed necessary. Some advisory group members suggested that value could be added to the tool if the information collected were shareable with a user’s health care providers and expressed interest in app integration with the electronic health record (EHR), specifically for urgent or concerning responses. Group members also generated suggestions for refinements to existing topics in the Learning Center. These included adding more detailed content on contraceptive access, cardiovascular symptoms, early bonding and infant attachment, and activities to measure and support infant milestones.
To replicate the information exchange that EHR integration would provide, we added messaging templates for sharing with clinical providers depending on the type of symptoms (“urgent” or “normal”) that users might report in the Healing Check-in. We also added language to emphasize that information in Myana does not constitute a medical diagnosis and that the app user should contact their health care provider (or 911, depending on severity) for “urgent” symptoms. The Learning Center was expanded to include newly generated topics from stakeholder group members. Each drafted Learning Center article (approximately 200 articles in total) underwent a rigorous iterative review process (Supplementary Fig. S1) to ensure relevance to the target audience, clinical accuracy, inclusion of diverse perspectives, and the supportive and approachable tone defined in the concept prototype end-user interviews.
Descriptive phase
Lastly, UX evaluation sessions were conducted with the birthing parents (n = 15, Table 3) to elicit feedback on the final app design. In their review of the refined wireframes, small changes were suggested to replace certain clinical terms used in the Healing Check-in questions with more colloquial wording: “Some of these words I don’t know… .” For example, a question in the Healing Check-in originally described postpartum blood clots as gel-like blobs of coagulated (thickened) blood and tissue but, with guidance from birthing parents, was updated to say gel-like blobs of thickened blood and tissue. Participants also recommended acknowledging the discomfort of their experience, even if that experience was considered normal. As one participant noted: “Remember that we’re super sensitive in this timeframe so the wording always needs to be super supportive, not clinical and scary. Just remember to keep all the wording and visuals in a supportive and gentle approach.”
Participants liked the range and availability of the final set of topics and offered suggestions to make the content even more inclusive (e.g., visual representation of bigger bodies). However, for the two participants in the UX sessions who had experienced an infant loss, the newly added infant content was found to be too triggering. As one participant noted: “Every time I say, ‘Yeah, this is my first kid,’ I die a little inside.”
Prior to the release of the minimum viable product, visual representation of birthing parents in the app (e.g., visual illustrations of symptoms in the Healing Check-in or embedded images paired with articles in the Learning Center) were updated to show diverse representations of body types and family structures, in addition to diverse racial/ethnic backgrounds. The clinical language in the Healing Check-in was updated to use plain language descriptors. Lastly, the app’s language and functionality were updated throughout to be more sensitive to infant loss. For example, we removed a question about whether this was the app user’s first child, since individuals who had experienced a loss found that question triggering.
Discussion
Here, we illustrate an iterative, theory-grounded process for developing a postpartum support app, focusing on the development trajectory of two features designed to proactively address issues at the core of maternal health inequities, while centering the needs of multiple stakeholders. Ongoing work includes a longitudinal observational cohort trial of Myana app use to evaluate acceptability and clinical outcomes (NCT07295015), and stakeholder-informed implementation planning prior to statewide dissemination to birthing parents in Pennsylvania. If successful, the app will enable earlier identification of and intervention on critical postpartum risks and allow for more nuanced understanding of the state’s maternal health population. In Pennsylvania, over 7% of counties are maternity care deserts, where patients have very limited access to maternal health care or birthing facilities. 33 Digital tools, like Myana, have the potential to address some of these maternal care gaps, by supporting birthing parents in differentiating critical symptoms from routine healing and recognizing when and where to seek care. Further, the framework and approach described here could be extended to other digital tool development both within and beyond the state of Pennsylvania. As states increasingly invest in digital connectedness, use of such design methods will be important for meeting their constituents' needs, while supporting equitable technology adoption.
Digital technologies are already integral to the current delivery of medicine in most health care systems, including electronic health records, 18 AI-based clinical decision supports and diagnostics,19,20 telemedicine, 21 and mHealth for patient education, 22 monitoring, 23 and intervention. The existing landscape of digital supports for maternal health largely target pregnancy. Recently, there have been some successes in digital tools supporting postpartum health monitoring and intervention. For example, remote (digital) management programs for postpartum hypertension have been shown to help birthing parents effectively self-monitor blood pressure, allowing for early recognition of hypertension, and potentially addressing racial disparities in follow-up care. 34 Similarly, studies show that some apps and other digital technologies may be successful at facilitating a return to physical activity postpartum, 35 with the larger goal of supporting cardiometabolic health. While a focus on digital tools to support more comprehensive postpartum health monitoring and education is emerging, evidence on the quality, effectiveness, and health equity considerations of existing tools remains limited.24,25,36 Therefore, those using them, whether individuals or health care systems, may have to make adoption decisions without adequate knowledge of how well the tools serve the needs of the end users. Part of the challenge of knowing whether a digital tool will deliver quality care is the lack of a unifying process driving their design, development, and evaluation. The results from the design process described here and in other recent work in the postpartum digital space37,38 highlight the need for an iterative, stakeholder-informed approach, even when addressing health disparitiesas an a priori goal of digital tool development. 16
Limitations
Qualitative interviews and focus groups are labor-intensive and, as such, tend to have small sample sizes.39,40 Our qualitative data collection sessions were conducted until views became repetitive. While small samples can inform us about a range of beliefs and experiences, some perspectives and experiences were inevitably not represented. In such work, it is important to determine the minimum target audience a tool must serve. In our own work, we found that parents who had suffered an infant loss, for example, could not be adequately served by the app we had designed and had to adjust our design to communicate this. Similarly, we found that the partners of those enrolled in our experience prototype testing were informally using the app alongside our birthing parent participants, but we had to defer the creation of a dedicated partner app as a future initiative.
A key strength of this work lies in the multiple end-user-centered iterations that informed the final design of our postpartum support app. For academic researchers, the pace and cost of such work is often dependent on federal or nonprofit funding cycles. Commercial technology moves on a faster timeline. Our approach risks building an equity-focused and scientifically rigorous app that cannot keep pace with the technological advances or widescale dissemination of its competitors unless an independent champion (e.g., a professional organization or state) commits to its support.
Conclusion
Increasingly, models of maternal care integrate digital components, including mHealth apps. Their success depends on meeting both clinical and individual patient needs. Our approach to building the Myana (Mothers, you are not alone) app included multiple, iterative phases of data collection and design revision to bridge the gap between clinical requirements and end-users’ needs, while centering health disparities as a strategy to advance health equity and improve outcomes. Using two examples of features designed to redress health inequities, we offer concrete examples of how this process was applied to design decisions. Even after dissemination, this iterative and inclusive process can and should be ongoing. As medical knowledge advances, user needs change, and public health priorities shift, such tools should be evolving with them.
Authors’ Contributions
S.K.B. analyzed and interpreted the data and drafted the article. A.D. and R.O. contributed to the design of the digital tool, interpreted results, and critically revised the article. K.N.R., A.B., and H.S. contributed to the design of the study, interpreted data, and critically revised the article. T.K. conceptualized and designed the study, acquired and interpreted the data, supervised analysis, and critically revised the article. All authors approved the final version for publication and are to be held accountable for the work.
Footnotes
Acknowledgments
The content is solely the responsibility of the authors and does not necessarily represent the official views of, nor an endorsement by, any funding source. AI was not used in any portion of the article writing. Myana is currently accessible to participants in a clinical trial designed to evaluate usability, acceptability, and preliminary effectiveness, with intent to make it freely available for all birthing parents in Pennsylvania.
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
This work was supported in part by
Supplemental Material
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.