
Abstract
Objective:
Maternal mortality in Ethiopia is estimated to be 205 per 100,000 live births, with postpartum morbidities expected to surpass maternal mortality substantially. Beside this, there is a lack of information on postpartum morbidities in the study area. Thus, the purpose of this study was to assess the magnitude of postpartum morbidities and associated factors in Bale Robe Town, southeast Ethiopia.
Method:
An institution-based cross-sectional study was employed among 371 from 1 April to 30 May 2022 among postpartum women attending postnatal care service in the Bale-Robe Town public health facilities. A face-to-face interviewer administered a structured questionnaire, and the participants were selected through a systematic random sampling technique. A bivariate analysis was performed to see the association between each independent variable and dependent variable, and variables with p-values less than 0.25 in the bivariate analysis were retrieved for multivariable analyses. A p-value of less than 0.05 indicated a 95% confidence interval as the level of statistical significance.
Result:
A total of 366 participants were involved in the study, giving us a response rate of 98.6%. The magnitude of postpartum morbidities among mothers was found to be 102 (27.9%), with a confidence interval of 95% CI: 23.3, 32.8. Women who hadn’t had antenatal care follow-up (AOR = 2.47, 95% CI: 1.36, 4.50), instrumental delivery (AOR = 2.69, 95% CI: 1.16, 6.26), unskilled birth attendant (AOR = 3.35, 95% CI: 1.06, 10.63), rural residence (AOR = 2.21, 95% CI: 1.26, 3.89), and current pregnancy-related morbidity or abnormality (AOR = 3.81, 95% CI: 2.00, 7.25) were significantly associated factors.
Conclusion:
This study revealed that the occurrence of postpartum morbidity in Bale Robe is a great health concern. Therefore, we recommend health professionals and health extension workers strengthen early detection and management of intrapartum abnormalities, give attention during instrumental deliveries, and strengthen skilled birth attendants.
Introduction
Postpartum morbidity refers to a disease or complications that happen after the placenta has been expelled from 1 h to 6 weeks after. 1 It’s complicated, with many origins, varying durations from acute to chronic, and severity levels ranging from transitory to permanent, as well as a variety of diagnoses and treatment choices.2–5 Pregnancy, childbirth, and postpartum complications can result in death or persistent morbidities that impact a woman’s health for different periods of time, either during or after delivery. 4 The World Health Organization (WHO) describes the postnatal period as the most critical, and yet the most neglected phase in the lives of mothers and babies; most maternal and newborn deaths occur during this period.6,7
Globally, maternal mortality declined by more than a third from 2000 to 2017. Yet, tragically, an estimated 810 women continue to die each day due to complications of pregnancy and childbirth, mostly from preventable or treatable causes such as complications during or after pregnancy and childbirth. 8 Over 54 million women in developing countries are estimated to suffer acute morbidities yearly, with over 20 million considered so serious as to warrant referral care, and around 30 million women suffer from short- or long-term illnesses related to childbirth that adversely affect the quality of their lives and those of their families. 8 In a similar context, in developing nations, 15–20 million women develop disabilities each year as a result of childbirth complications, and in sub-Saharan countries, the magnitude of maternal morbidities varies from 20 to 920 per 100,000 live births. 9
The highest burden of severe postpartum maternal morbidity is in sub-Saharan Africa, where estimates of morbidity are as high as 198 per 1000 live births, hemorrhage and hypertensive disorders are the leading conditions contributing to severe maternal morbidities across all regions. 10 Ethiopia has one of the highest estimated numbers of maternal deaths, estimated to be 205 per 100,000 live births in the 2019 Ethiopian Demographic Health Survey (EDHS), where the first 48 h following childbirth account for a substantial share of maternal and newborn deaths. 11 Additionally, according to this report, approximately 200,000 Ethiopian women and girls are deprived of access to expert medical care during pregnancy, childbirth, and the postpartum period. Furthermore, a pocket of studies in Ethiopia revealed that postpartum morbidity ranged from 23.6% to 32.8%.12–14
In low-income countries, including Ethiopia, postpartum maternal morbidity is widespread and underrecognized. Aside from this, how frequently these issues occur and when women seek medical help are not well recorded. 12 Particularly, poor women commonly suffer from maternal morbidity because they either die or develop debilitating health problems such as fistulas, pelvic inflammatory disease (PID), and infertility for the rest of their lives.2–5
Previously, different studies showed that place of residence, marital status, antenatal care (ANC) service, maternal education, parity, iron supplementation during pregnancy, maternal Human Immune Deficiency (HIV) status, abnormal labor, mode of delivery, postpartum visit, severe anemia, low socioeconomic status, and parity were found to be determinants of postpartum morbidity.1,8,15
Maternal and child care during conception, pregnancy, labor, delivery, and the postpartum period is generally highly prioritized in many countries. 16 Unfortunately, there is an unacceptably significant possibility of dying, particularly in countries with poor infrastructure like Ethiopia. To overcome this global community expert plan by 2030, they aim to decrease maternal mortality to 70 per 100,000 and neonatal mortality to 12 per 1000. 17 A certain approach is to refocus efforts on addressing the health complications that affect these women rather than just focusing on lowering maternal mortality rates. Programs like the Initiatives toward Ending Preventable Maternal Mortality (EPMM) are a good instance of this matter.18–20 Even though maternal and newborn mortality is receiving a lot of attention around the world, the topic of maternal health concerns following delivery has gotten a lot less attention.13,21,22 Postpartum morbidity is a severe maternal health issue with several contributing factors, yet very little is known about its extent and affecting factors in Bale Robe town. As a result, the purpose of this research is to assess the extent of and identify contributing factors in Bale Robe town to fill an information vacuum.
Methods and materials
Study setting and period
A facility-based cross-sectional study design was employed from 1 April to 30 May 2022, among postpartum women attending postnatal care (PNC) service in the Bale-Robe Town public health facilities. Bale-Robe town is the capital of the Bale zone and is located 430 km from Addis Ababa, the capital of Ethiopia. According to the town administrative health office, the total population of the town was 148,089 in the year 2019, of whom 72,860 (49.2%) are females. The town is found at an altitude of 2492 m above sea level, and there is one general public hospital, one public health center, and twelve private clinics in the town. Postnatal care is available at the town’s public health facilities, whereas private clinics do not offer delivery or postnatal services.
Source population
All postpartum women who were visiting postnatal care services at public health facilities in Bale Robe Town were our source population.
Study population
Mothers who were visiting postnatal care services during the data collection period at public health facilities in Bale Robe Town.
Eligibility criteria
Postpartum women who visited postnatal care services during the study period were included, while postpartum women whose medical records contained incomplete information were excluded.
Sample size determination
The sample size required for this study was calculated using a single population formula with the assumptions of a 95% confidence level (Zα/2 = 1.96), 5% margin of error (d = 0.05), and the proportion of postpartum morbidity taken from a study done in Debre Markos, Northern Ethiopia was 32.8. 13 Considering a 10% nonresponse rate, the final sample size required for this study was found to be 371 postnatal mothers.
Sampling procedures
The study was conducted among postnatal women who arrived at public health facilities found in Bale Robe town for a postnatal visit. According to the town health office report, the town has two public health facilities that provide PNC, namely Bale Robe Hospital and Baha Biftu Health Center. Initially, for our study, we selected both public health facilities found in town. Then, to know the average postpartum mothers flow, we took a sample of data 6 months prior to the study. The average postnatal woman flow in 6 months at Bale Robe Hospital was 3312, and similarly, the six-month client flow at Baha Biftu Health Center was 966. By having this, we calculate the monthly postnatal mothers flow since our data collection period was in the month. From this, we got 552 and 161 the average monthly postnatal mothers flow in Bale Robe Hospital and Baha Biftu Health, respectively. Then, proportional allocations were made for the respective health facilities. By using this, we calculated the interval (K) for which we could select the women. Thus, the interval (K) was calculated by dividing the total number of mothers by the total number of proportionally allocated numbers respective to each public health facility, and therefore we obtained K = 1.92–2. Lastly, the first client was selected by the lottery method, and then the rest were selected by the systematic random sampling method at every K interval.
Data collection method
Data collection tool
A structured, interviewer-administered questionnaire and check list for document-reviewed data collection were used for this study. Data was collected by check list items containing items to assess outcome variables postpartum morbidity, sociodemographic characteristics of the study participants, obstetric characteristics of the study participants, and medical-related factors. To assess postpartum morbidity, a validated WHO guideline check list that was used in both developing and developed countries was used, a tool also used in previously published articles in Ethiopia. The questionnaires to assess sociodemographic status, obstetrics, and health services-related factors were adapted from similar previously published literature.17,19,20
Data collection process
Detail training was given for data collectors and supervisors on the contents of the data abstraction tool and how to collect data from selected mothers, review medical records, and postnatal log books for 2 days before the data collection period by the principal investigator. The data collection formats were made ready for use, then the data were collected by face-to-face exit interviews using questionnaires for sociodemographic factors, and a checklist was used to review mother’s charts, delivery records of labor wards, and reporting logbooks. During actual data collection, data collectors were supervised, and the questionnaire was checked for completeness daily. Data collectors were midwives and nurses, and two experienced supervisors were allocated.
Study variables
Dependent variable
Postpartum morbidity.
Independent variable
Sociodemographic factors include age of the women, marital status, educational status of women, residence, occupation, the households monthly income; and obstetrics factors include gravidity, parity, gestational age, place of delivery, mode of delivery, clinical comorbidity, pregnancy-related Morbidity, and person attended labor (skilled or unskilled). Lastly, medical factors such as anemia, HIV/AIDS, diabetic mellitus, heart disease, and tuberculosis.
Operational definitions
➢ Maternal morbidity: Any health condition attributed to and/or complicating pregnancy and childbirth that has a negative impact on the woman’s well-being and/or functioning. 24
➢ Postpartum morbidities: Postpartum morbidity encompasses diseases or complications occurring from 1 h to 6 weeks after childbirth, following the expulsion of the placenta. 2 For the purposes of this study, a mother diagnosed with any morbidity, including conditions such as postpartum hemorrhage, preeclampsia, sepsis, and others, was classified as experiencing postpartum morbidity.
Data quality control
To assure the quality of the data, close supervision was maintained by the principal investigator. Any ambiguities or unclear ideas during the data collection process were resolved by having a discussion with data collectors, supervisors, and the principal investigator. Every day, the investigator participated in the evaluation of the data gathering process and made necessary corrections before the next day’s activities. The English version of this questionnaire was translated by language experts to Amharic and Afaan Oromo and back to English to check for consistency. A pretest was done at Goba Hospital, which was found in a different town, 2 weeks before the actual data collection period, with 5% to assure clarity, logical sequence, and feasibility of measuring important variables.
Data analysis
The collected data were coded, entered, checked, and cleaned by Epi-data 3.1 and exported to a statistical software package, SPSS 25, for data analysis. The proportion of postpartum morbidity (PPM) was computed by running descriptive statistics, followed by bivariate and multivariable analysis to determine the statistical association between independent and dependent variables. The model’s fitness was tested by Hosmer and Lemshow at a significant value of less than 0.05. Variables that were <0.25 significance level in the bivariate logistic regression analysis were considered for multivariable logistic regression analysis. The presence and degree of association between outcome and independent variables were computed through an odds ratio with a 95% confidence interval (CI) and a p-value < 0.05. Then, the result was presented using tables, figures, and narratives.
Results
Sociodemographic characteristics of the respondents
A total of 366 participants were involved in the study, yielding a response rate of 98.6%. The mean age of the participants was 28.69 (±SD 6.07) years, with a range of 18–44 years, and 106 (29.0%) were between the ages of 20 and 24. Most of the respondents were married women, 309 (84.4%). 132 (36.1%) of the respondents had secondary school education, followed by college and above education (97 (26.5%)). The respondents comprised 158 (43.2%) housewives and 262 (71.6%) residents of Robe town, respectively (Table 1).
Sociodemographic status of mothers on postpartum morbidities in health facilities found in Bale robe town, 2022.

Obstetrics history of the mother
Most of the mothers, 301 (82.2%), were multipara, and 296 (80.9%) had antenatal care follow-up. More than half of the mothers, 229 (61.2%), were delivered by spontaneous vaginal delivery; less than 10%, 35 (9.3%), gave birth by instrumental assisted moreover, 349 (95.3%) of the mothers were delivered with the support of skilled health professionals. About 308 (84.2%) had a term pregnancy. Around 59 (13.9%) mothers had pregnancy-related morbidity at the time of their current pregnancy (Table 2).
Obstetrics and medical status of mothers on postpartum morbidities in health facilities found in Bale robe town, 2022.

ANC: ante natal care; PNC: post-natal care; Parity: number of deliveries; Gravidity: number of pregnancies.
The magnitude of postpartum morbidities
Out of the 366 maternal charts examined, 102 (27.9%) had postpartum, of which 48 (13.1%) had two or more morbidities. Major morbidities include postpartum hemorrhage (9.3%), preeclampsia/eclampsia (6.3%), anemia (4.6%), cesarean section (6%), and problems related to the episiotomy such as wound dehiscence and episiotomy breakdown (6.0%) (Figures 1 and 2).

Magnitude of postpartum morbidities found in public health facilities in Bale, Robe town, Oromia region, southeast Ethiopia, 2022.
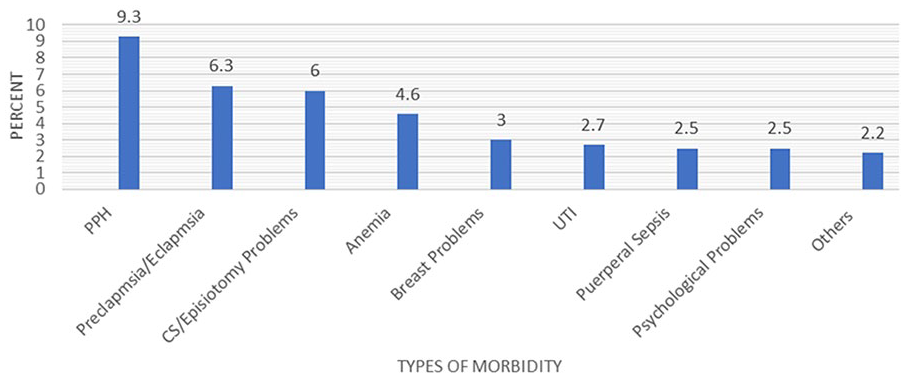
Types of postpartum morbidities found at public health facilities in Bale Robe town, southeast Ethiopia, 2022.
Factors associated with postpartum morbidities
In bivariate analysis, variables such as residence, occupation of a mother, marital status, mode of delivery, place of delivery, pregnancy-related morbidity in a current pregnancy, antenatal care follow-up, and delivery attended were statistically significant at a p-value less than 0.25. In the multivariable analysis, five variables—antenatal care follow-up, mode of delivery, residence, delivery attended by, and current pregnancy-related morbidity showed a significant association with a p-value of <0.05. Mothers who have current pregnancy-related morbidity are 3.8 times more likely to develop postpartum morbidity compared to those who have no current pregnancy-related complications, as indicated by an adjusted odds ratio (AOR) of 3.81 (95% CI (2.0, 7.25)). Additionally, not having antenatal care follow-up makes it 2.4 times more likely to develop postpartum morbidity, with an adjusted odds ratio (AOR) of 2.50 (95% CI (1.36, 4.50)). Women delivered by unskilled birth attendants have a 3.3 times greater likelihood of experiencing postpartum morbidity compared to those delivered by skilled birth attendants, as indicated by an AOR of 3.35 (95% CI (1.06, 10.63)).
The other significant factor is the mode of delivery. Mothers whose deliveries are instrumentally assisted are 2.6 times more likely to develop postpartum morbidity as compared to mothers who delivered by spontaneous vaginal delivery, with an AOR of 2.70 (95% CI (1.16, 6.24)). Residence is also the other significant factor in the model. Mothers who live outside of Robe town had a 2.2-fold higher likelihood of having postpartum morbidity than those who live inside Robe town, as evidenced by an adjusted odds ratio (AOR) of 2.20 (95% CI (1.26, 3.89)). The study showed that factors such as marital status, the mother’s work, the attendant during delivery, and the location of delivery had no significant association with postpartum morbidity. This implies that these characteristics do not have a substantial impact on their likelihood of having postpartum problems (Table 3).
Factors associated with postpartum morbidity among women who gave birth at public health facilities in Bale Robe town, Oromia, southeast Ethiopia, 2022.

Key: *p-value ⩽ 0.05 in bivariate analysis; **p-value ⩽ 0.05 in multivariable analysis. 1-Reference group.
Discussion
This research was conducted in Bale Robe town’s public health facilities to determine the prevalence of postpartum morbidity and pinpoint risk factors for it. According to our study, postpartum morbidity was at a proportion of 27.9%, which is congruent with the studies conducted in Gondar (23.6%) and DebreMarkos, Ethiopia (32.8%).12,13 This might be due to studies carried out in the same nation under analogous circumstances, which suggest that the health care system there is probably comparable.
The finding of our study was greater than those of the studies conducted in Brazil (21.2%), Morocco (13.1%), Pakistan (4%), and Nepal (2.96%). The difference between our study and the former study conducted in Brazil might be due to the variations in sample size, the research setting, and the factors affecting maternal health issues. 23 Additionally, our research’s finding was comparatively high compared to the study’s in Morocco, which might be a result of variations in the study population and the healthcare services provided. 18 In contrast to our study, the results of a study carried out in Pakistan, which solely involved rural people and severe postpartum maternal illness, also differ in sample size. Comparably, the results of this study were higher than those of the study carried out in Nepal. Our study covers all women who seek postpartum health care services, regardless of whether they were hospitalized or not, which is the key difference between it and the Nepalese study.2,24 Furthermore, the disparity may be due to the differences in the health care system in terms of infrastructure, quality of health care, and policy among different countries. Specifically, compared to studies conducted in Brazil, Pakistan, and Nepal, our study was conducted in low-income countries, which affect the health systems of one nation.
Our study’s finding was lower than those of studies conducted in Morocco (44%), the Democratic Republic of the Congo (64.5%), and India (39.5 %), this may be related to the size of the sample used, the duration of the study, and the fact that the Morocco study included self-reported morbidities in addition to those that were actually diagnosed. Furthermore, the variability might be the difference in health care delivery system, distribution of risk factors among the studied group, and regional variability (Democratic Republic of the Congo), Moreover, variations in study populations, research methodologies, and self-reported morbidity may account for these studies’ discrepancies (India).22,25,26
The findings of this study have shown important health risks for pregnant and postpartum mothers. The most common cause of morbidity was postpartum hemorrhage (9.3%), which was followed by preeclampsia/eclampsia-related complications (6.3%), problems from cesarean sections and episiotomies (6%), and anemia (4.6%).
According to this study, there is a statistically significant correlation between receiving ANC services throughout a woman’s pregnancy and the development of postpartum morbidity. Agreed to this study is a studies done in Gamo Gofa Zone, and Debre Markos reported not having prenatal care as a risk for postpartum morbidity.13,27 This is because women benefit from early case detection and management when they receive ANC follow-up. Furthermore, since the majority of obstetric difficulties are predicted, healthcare professionals rigorously monitor perinatal care and separate high-risk women during ANC follow-ups.
A substantial positive link exists between postpartum maternal morbidity and mothers who currently had a pregnancy-related complication or problem. The research from Gondar, Debre Markos, and Bangladesh supports this study by stating that women’s who experience abnormal labor are more likely to experience postpartum morbidity.12,13,21 This is because the majority of obstetric problems continue from pregnancy into the postpartum phase. Similarly, some obstetric complications might also be risk factors for the occurrence of others.
Maternal morbidity and delivery methods have a strong relationship. Women who give birth with instrumental assistance have a 2.6 times higher risk of developing postpartum morbidity than mothers who give birth spontaneously. This result agrees with a study conducted in Canada and Felege Hiwot Comprehensive Specialized Hospital. Consequently, there is a significant connection between the delivery attendant and postpartum morbidity. Women who deliver with an unskilled birth attendant have a 3.3 times greater likelihood of experiencing postpartum morbidity than women who deliver with a trained birth attendant. This is due to the fact that providing skilled birth might decrease three-fold maternal morbidity.
The aforementioned conclusion is consistent with the findings of Debre Markos’ investigation, which found that women delivered by doctors are around 89% less likely to experience postpartum problems than those delivered by untrained birth attendants. Moreover, women in rural areas have a twofold increased risk of experiencing postpartum morbidity compared to their counterparts in urban areas, owing to the lack of infrastructure such as roads, nearby health centers, and transportation.13,28
Limitations and strengths
This study includes all public health facilities in Bale Robe town, and our study used both primary and secondary data, thereby improving the quality of the data. In addition to this, the result of this study might be used in the future to investigate the health-seeking behavior of mothers for postpartum morbidity and knowledge about postpartum morbidities in the community. However, this study does not measure self-reported complaints or morbidities, which might underestimate the magnitude of postpartum morbidities in a community.
Conclusion and recommendation
Conclusion
This study revealed that the occurrence of postpartum morbidity is a great health concern. Women who didn’t have antenatal care services, a complication in current pregnancy, instrumental delivery, women delivered by unskilled birth attendants, and rural residents were factors associated with maternal postpartum morbidity. Therefore, we should focus on access to prenatal care services, early detection and management of intrapartum abnormalities, educating mothers on the benefits of institutional delivery by a skilled birth attendant, and giving great attention while using instrumental deliveries.
Recommendation
We recommend that health professionals strengthen maternal health education on the benefits of antenatal care, provide special follow-up for mothers who have pregnancy-related problems as well as labor abnormalities, give a great deal of attention while using instruments during delivery, or reduce instrumental deliveries as much as possible. In addition, it is recommended that maternal health care providers educate and sensitize all pregnant women to give birth in the health institution and work on reducing unskilled birth attendants. Furthermore, educate the mothers on the prevention of complications and early recognition of postpartum morbidity and danger signs.
Second, in general, in order to reduce postpartum morbidities, health extension workers, together with professionals from health institutions, should prioritize creating awareness, antenatal care follow-up, place delivery, and birth preparedness plans. Additionally, woreda officers and programmers should be strengthening the monitoring and evaluation system of obstetrics care. Furthermore, it is expected to expand infrastructure like maternal waiting homes and other infrastructure for rural residents. Finally, we recommend the researchers do further studies on community-based research to increase the representativeness of the study.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241272580 – Supplemental material for Magnitude of postpartum morbidity and associated factors in southeast Ethiopia, 2022: A facility-based cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121241272580 for Magnitude of postpartum morbidity and associated factors in southeast Ethiopia, 2022: A facility-based cross-sectional study by Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo and Woiynshet Gebretsadik in SAGE Open Medicine
Footnotes
Acknowledgements
Our gratitude goes to Arba Minch University, College of Medicine and Health Science, School of Nursing, for providing ethical clearance and opportunity. Our appreciation also goes to the data collectors, supervisors, and respondents, without whom this study would not have been realized. Last but not least, we would like to acknowledge Bale Robe General Hospital, Baha Biftu Health Center, their medical directors, and staff for their cooperation and support.
Authors’ contributions
Feisal Hussein Hasen and Solomon Seyife have contributed equally to the proposal development, development of the tools, data collection process, and analysis. The authors have revised the final version of the manuscript and given their approval for publication. Conceptualization: Feisal Hussein Hasen, Woiynshet Gebretsadik. Data Curation: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, Woiynshet Gebretsadik. Formal analysis: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Investigation: Feisal Hussein Hasen and Woiynshet Gebretsadik. Methodology: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Project administration: Feisal Hussein Hasen. Resources: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Software: Feisal Hussein Hasen and Woiynshet Gebretsadik. Validation: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Visualization: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Writing: original draft: Feisal Hussein Hasen, Solomon Seyife Alemu, Derese Eshetu, Bedria Mohammed, Eden Nebi, Hana Israel, Yomilan Geneti, Lema Fikadu Wedajo, and Woiynshet Gebretsadik. Writing: review and editing: Feisal Hussein Hasen, Solomon Seyife Alemu, and Woiynshet Gebretsadik.
Availability of data and materials
The data used in this study is available upon reasonable request upon the corresponding author at any time if required. Therefore, any person who need data it can obtain it from principal investigator through contact address (e-mail:
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Arbaminch University for the sake of questionnaire duplications and data collection purpose, and other budget was covered by the authors.
Ethics approval and consent to participate
Ethical clearance was obtained from the Arba Minch University College of Health Sciences and Medicine Institutional Research Ethical Review Board (IRRB) with reference number IRB/1217/2022. Written permission to support the research was obtained from the medical director of the hospital and health center from which the data were collected. Written and informed consent was obtained from participants after their willingness to participate in the study and after explaining all the objectives, risks, and benefits of being involved in the study. We did not seek written informed consent from the legally authorized representatives of minor subjects because all participants in our study were over the age of 18. Furthermore, in this study, even though some study participants have no formal education, they are able to read and write because they have received informal education from adult education programs, religious institutions, and other sources. Hence, all study participants participated after they gave written consent. The right of respondents not to participate in the study or withdraw from the study at any time was respected. All the information obtained from the mothers and their charts was held with confidentiality and used only for the intended purpose.
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from all study participants. In this study, even though some study participants have no formal education, they are able to read and write because they have received informal education from adult education programs, religious institutions, and other sources. Hence, all study participants participated after they gave written consent.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.