
Abstract
Introduction:
Breastfeeding disparities persist for African American lactating people despite known health benefits and targeted breastfeeding promotion. In Chicago, services are rapidly decreasing in the communities with the greatest need, creating fragmented perinatal care and subpar breastfeeding support. Our study aimed to engage a community advisory board to understand the needs of African American lactating people in Chicago, define challenges, and brainstorm ideas to redesign an application prototype and mobile health intervention to advance health equity.
Methods:
A qualitative descriptive design guided by the design thinking processes augmented with the Public Health Critical Race Praxis approach was utilized for this study. Virtual design studios (16) were conducted that focused on breastfeeding in the context of design thinking with a race-conscious lens.
Results:
Ten African American community members (six lactation professionals and four parents) joined the community advisory board. Thematic analysis revealed three themes: no such thing as antiracist care for us, limited breastfeeding support for African American people, and support African American people to challenge racism and advocate for themselves.
Discussion:
This study bolsters equity through authentic engagement with a community advisory board in the development of breastfeeding support that meets the needs of African American lactating people in Chicago. The design thinking process and Public Health Critical Race Praxis framework provided an avenue to effectively consider the historical context that drives bias and identify solutions. More research is needed to understand the needs and challenges of lactating people in other geographical regions.
Keywords
Introduction
In Illinois, breastfeeding initiation rates have remained high for White (91%) and Hispanic (95%) people compared with African American people (84%). A gap in exclusive breastfeeding continues through 3 months, with a substantial decline to 45% for White and 23% for African American people. 1 These low rates of continued breastfeeding present a major public health concern as infant feeding has a direct impact on the health and mortality of infants and birthing people. Breastfeeding is significantly associated with decreased risk of sudden unexplained infant death (SUID) and respiratory infections for infants. Benefits for lactating people include decreased risk of cardiovascular disease and breast cancer. 2 This evidence highlights breastfeeding as an effective preventive measure to improve the health of infants and birthing people, specifically for African American people, as they are approximately 2.5 times more likely to die after childbirth compared with White people, 3 and African American infants are 2 times more likely to die from SUID compared with White infants. 4 Interventions that address the racial disparity in breastfeeding are essential for the health of birthing people and infants.
Several complex factors have been found to impact the breastfeeding behavior of African American people. Persistent racism, skewed marketing of formula, and lack of support have significantly influenced infant feeding decisions.5–7 Cultural beliefs regarding breastfeeding are rooted in the history of mistreatment of African American lactating people being forced to become wet nurses for their slave owners’ children while neglecting their own infants.5,8,9 After slavery, many African American people chose to leave the wet nurse designation behind and adopt the behaviors of White people.6,8 Infant formula marketing pushed the idea of formula as a status symbol of the elite and the freedom to decide how to feed infants, which further contributed to the abandonment of breastfeeding. 5 Historical legacies of brutality and lack of personal autonomy have contributed to a negative connotation for breastfeeding that has been passed down for generations and resonates with many in the African American community today.5,8
Despite the historical context, some African American people do breastfeed but face challenges. Breastfeeding support services are lacking in the communities where the greatest disparities in breastfeeding exist. 10 Numerous hospital closures and lack of funding for community health organizations have impacted the quantity and quality of perinatal care for some African American people in Chicago, leaving them with fragmented and subpar breastfeeding support. 10 Limited access to appropriate support has led lactating people in other communities to do their own breastfeeding research using the internet and connecting on social media, 11 illustrating the need for readily accessible breastfeeding support. Social media and automated texting tailored to breastfeeding education for African American birthing people may be an effective and convenient way to provide lactation support. 12 More research on technology use and lactation support is needed. In this article, we describe the engagement of a community advisory board to understand the needs of African American lactating people in Chicago, define barriers, and brainstorm ideas to gather insight for redesigning a breastfeeding application prototype and mobile health intervention to advance health equity.
Methods
This study used a qualitative descriptive design. The design thinking process augmented with the Public Health Critical Race Praxis (PHCRP) approach was utilized to understand the needs of African American lactating people and address challenges (Fig. 1). Design thinking provides a solution-based method to address complex problems such as the persistent racial disparity in breastfeeding outcomes. This five-step process focuses on an iterative process to understanding human needs (empathy), framing the problem (define), creating solutions (ideate), and applying a practical model (prototype) to investigate (test). 13 In this article, we report on the first iteration of the design thinking process from empathy through ideate strengthened with the PHCRP.
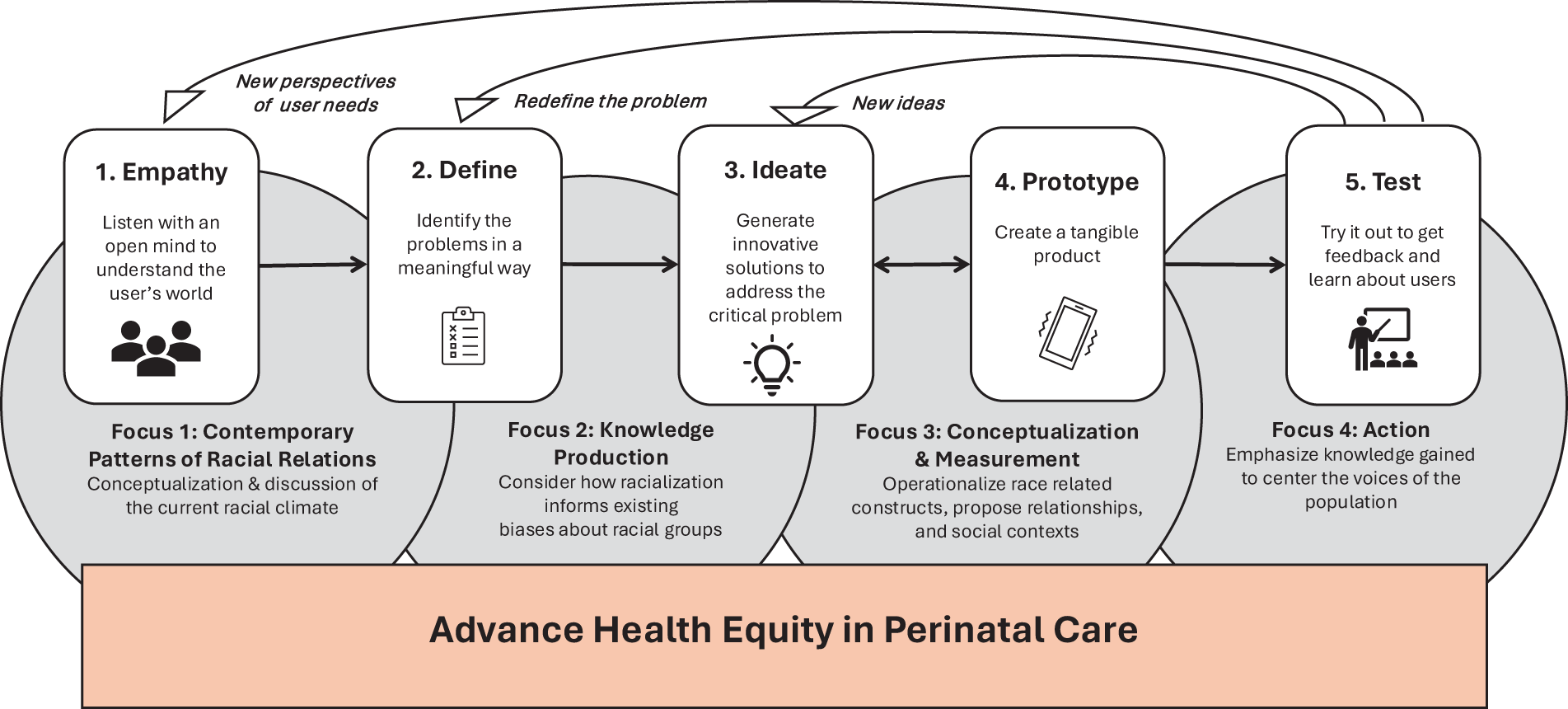
Design thinking process augmented with the Public Health Critical Race Praxis.
The PHCRP methodology integrates the critical race theory principles into public health-oriented racial equity research to confront the structural mechanisms precipitating and perpetuating health inequities. 14 This approach pulls from antiracist efforts while upholding the scientific integrity of modern research methodologies that include four phases (contemporary patterns of racial relations, knowledge production, conceptualization and measurement, and action).14,15 Since it was introduced in 2010, the PHCRP has guided a limited number of women’s health-related studies.16,17 Researchers have explored the impacts of structural racism in the United States, including policing practices and medical discrimination, on adverse birth effects 16 and African American women’s health outcomes. 17
Setting and Sample
A virtual setting was used to convene advisory board members for design studio sessions. Inclusion criteria were: (1) self-identify as an African American parent or breastfeeding support professional in Chicago, (2) ≥18 years of age, (3) interest in improving access to breastfeeding support, and (4) commitment to maintain a 1-year relationship with the research team. Flyers listing the inclusion criteria and describing the advisory board were distributed to community organizations, local hospitals, and members of the Chicago Regional Breastfeeding Task Force. The goal of recruitment was to enroll 10 African American parents (5) and providers (5) from disparate settings to represent each user of the breastfeeding application. People responding to the flyers were contacted for an interview to learn more about potential members and assess commitment as a collaborative partner to provide a diverse perspective regarding the needs of African American lactating people.
Data Collection
The study was approved by the Rush University’s Institutional Review Board. Data were collected from February 2022 through September 2022 via virtual design studio sessions using Zoom. Research-focused studio models are structured for real-world projects and commonly used in architectural education. Studios allow an opportunity to gain evidence for solutions to design problems regarding appearance, feeling, and function, providing an environment for reciprocal resolution building in the design process. 18 In design studio environments, participants respond to challenges that mimic real-world practice or push limits of current design standards that generate new ideas, shifting ordinary design to an extreme context. Data collection via design studios is guided by design thinking principles and has been found useful for addressing complex issues with solutions refined in an iterative process, providing evidence to inform subsequent design. 18 Thus, the design studio model was adopted to engage advisory board members in discourse to identify lactation care barriers and brainstorm solutions suitable for mobile application integration. Members were invited to join the advisory board, sign a member agreement and intake form, confidential disclosure agreement, and informed consent. Advisory board members were divided into two groups for the design studio sessions to minimize the power differential among providers and parents. Group A included breastfeeding and maternal care professionals, while group B included parents. Members received a $25 gift card for each design studio attended.
Eight 1-h virtual design studio sessions centered on breastfeeding experiences, needs, barriers, and solutions (Table 1) were conducted for both groups (16 total) with 3–6 members attending each session. Using a collaborative design approach, the sessions prioritized solving lactation care barriers for end users and professional stakeholders rather than perfecting the mHealth technology. 19 Group norms were established in collaboration with advisory board members to provide an inclusive space for sharing thoughts without fear of judgment and a brave space with encouragement to challenge discussion in a positive way through actively engaging in the conversation with cameras on. Each design studio session began with a member check-in to learn more about each other, build trust, and contribute to a psychologically safe environment members feel comfortable in for reciprocal interaction. The PI, an African American nurse researcher and mother, facilitated all design studio sessions. Research staff assisted with the moderation of the sessions taking notes and soliciting feedback for clarification. All sessions were audio- and video-recorded.
Design Studio Sessions and Semi-Structured Interview Guide
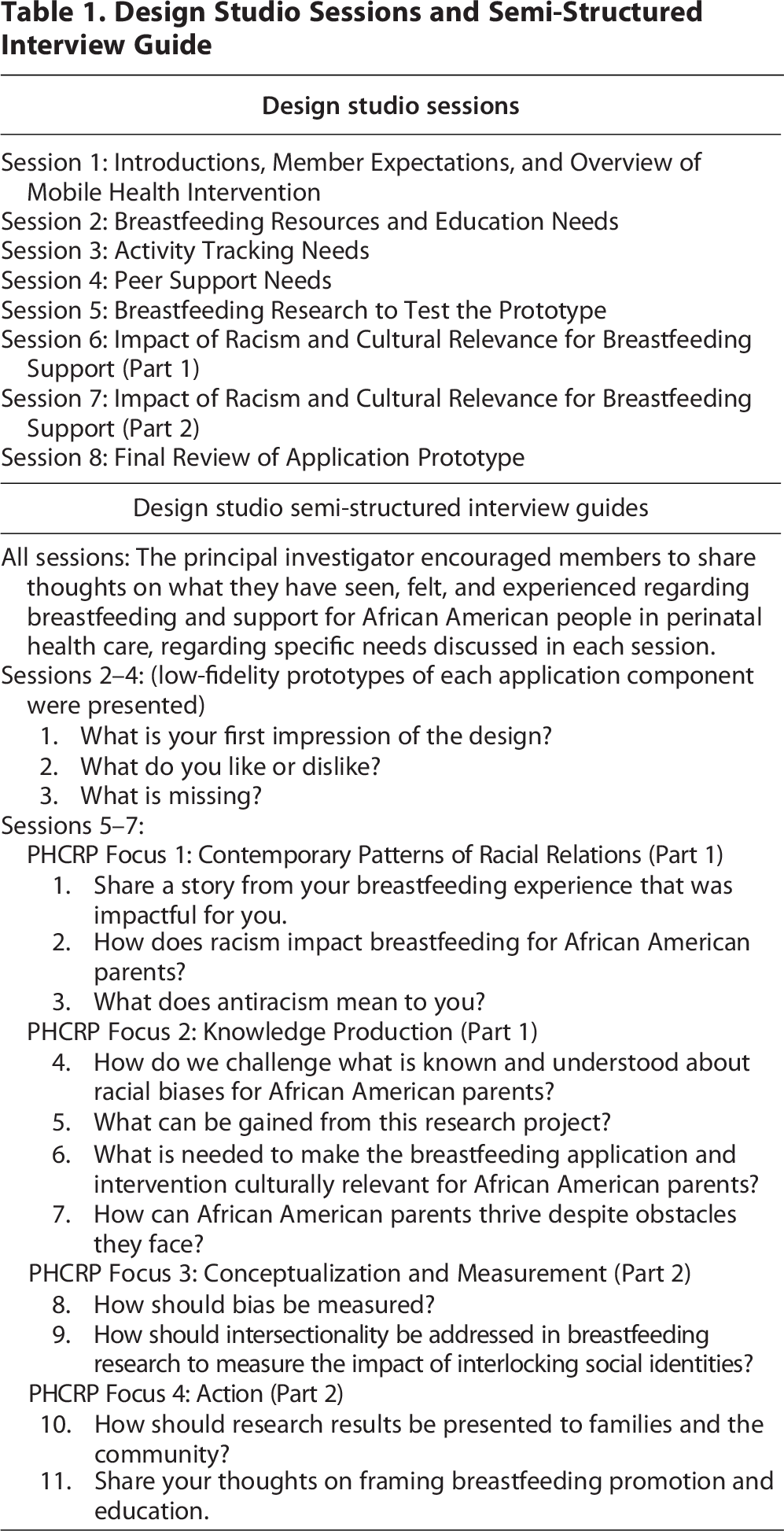
An overview of the mobile application, research ideas, and guiding frameworks was provided in the first session. Semi-structured interview guides (Table 1) used during the design studio sessions were mapped by the design thinking process and PHCRP. In alignment with design thinking, we employed empathy methods during each session, with mindful listening, keeping an open mind 13 to understand lactation needs and barriers of African American parents. Members were encouraged to share stories during sessions 2–4 to provide a first-hand account of relevant perspectives of user needs related to lactation care experiences (empathy and define) and suggested solutions (ideate). To ensure evidence was grounded in a race-conscious orientation, the PHCRP14,15 guided specific questions developed by the PI on the semi-structured interview guide discussed during sessions 5–7 (Table 1). This allowed dedicated sessions to discuss racism and its impact on breastfeeding behavior. The PI reviewed the PHCRP tenets,14,15 with the advisory board providing explanations for terms used in the interview guide that were mapped to the praxis in preparation for deeper bidirectional discourse regarding culturally relevant breastfeeding research.
Data Analysis
Descriptive statistics were used to analyze sample characteristics. Audio recordings of studio sessions were transcribed verbatim by two research assistants. The PI verified all transcripts. Thematic analysis of narrative data was used to understand this group’s perspective regarding the breastfeeding needs of African American lactating people, define barriers, and brainstorm ideas to gain insight for redesigning a breastfeeding application. Team dynamics bridged maternal–child health clinical and research experience among three nurses and one International Board-Certified Lactation Consultant (IBCLC) employed as a breastfeeding peer counselor to enhance methodological rigor through a collaborative approach to data analysis. The PI (author 1), research coordinator (author 2), and breastfeeding peer counselor (author 3) independently engaged with data by watching all recorded sessions and reading transcripts to become familiar with the depth of the content and identify relevant findings from general discussion and stories shared. 20 Reflexive notes were recorded to track iterative meeting logistics, decisions, and personal reflections including individual thoughts, interpretations, and questions to establish trustworthiness of the thematic analysis process. 20 Independent quotes were collectively reviewed by the research team and grouped by design thinking and PHCRP concepts focused on breastfeeding needs, barriers, and solutions. Coded data were discussed using a deductive approach to reflect patterns, giving meaning to data 20 via empathy maps to get a deeper understanding of advisory board members’ lactation needs. Advisory board members’ thoughts, feelings, needs, and behaviors were mapped to identify themes that define barriers and view suggested solutions. 21 An audit trail of raw data, session notes, transcripts, codes, themes, and reflexive notes was maintained and reviewed by two senior team members (authors 4 and 5) to confirm the validity of final themes. Finally, consensus was reached with shared decision-making of final themes through member checking with five advisory board members. 20
Results
Sixteen lactation professionals and seven parents responded to the recruitment flyers with interest in joining the research advisory board. Virtual interviews were conducted with 13 potential members who met the inclusion criteria. Five lactation professionals were excluded due to living outside the Chicago area, and five did not respond to interview invitations. Seven lactation professionals and five parents were invited to join the research advisory board. Ten members (six lactation professionals and four parents) joined the advisory board and completed enrollment. All members self-identified as non-Hispanic African American, and their gender as women with personal breastfeeding experience. Three lactation professionals were registered nurses, with two having certifications in maternal-newborn nursing. Other professions included coordinators for research; the special supplemental nutrition program for women, infants, and children; and a doula program. Half of the lactation professionals (three) reported current work with lactating people in the hospital setting and three in a community setting with four members having current IBCLC status and one certified lactation consultant status. The majority (three) of parents were currently breastfeeding a child 9 months of age and older at the time of data collection, and one had breastfed two children for 18 months.
Through empathy mapping, three themes emerged to define barriers. The first two themes focused on defining barriers, which included no such thing as antiracist care for us and limited breastfeeding support for African American people. While brainstorming ideas for a practical solution to barriers, the third theme, support African American people to challenge racism and advocate for themselves, emerged. To highlight the voice of advisory board members, direct quotes are italicized in quotation marks with additional quotes listed in Table 2.
Themes and Exemplar Quotes
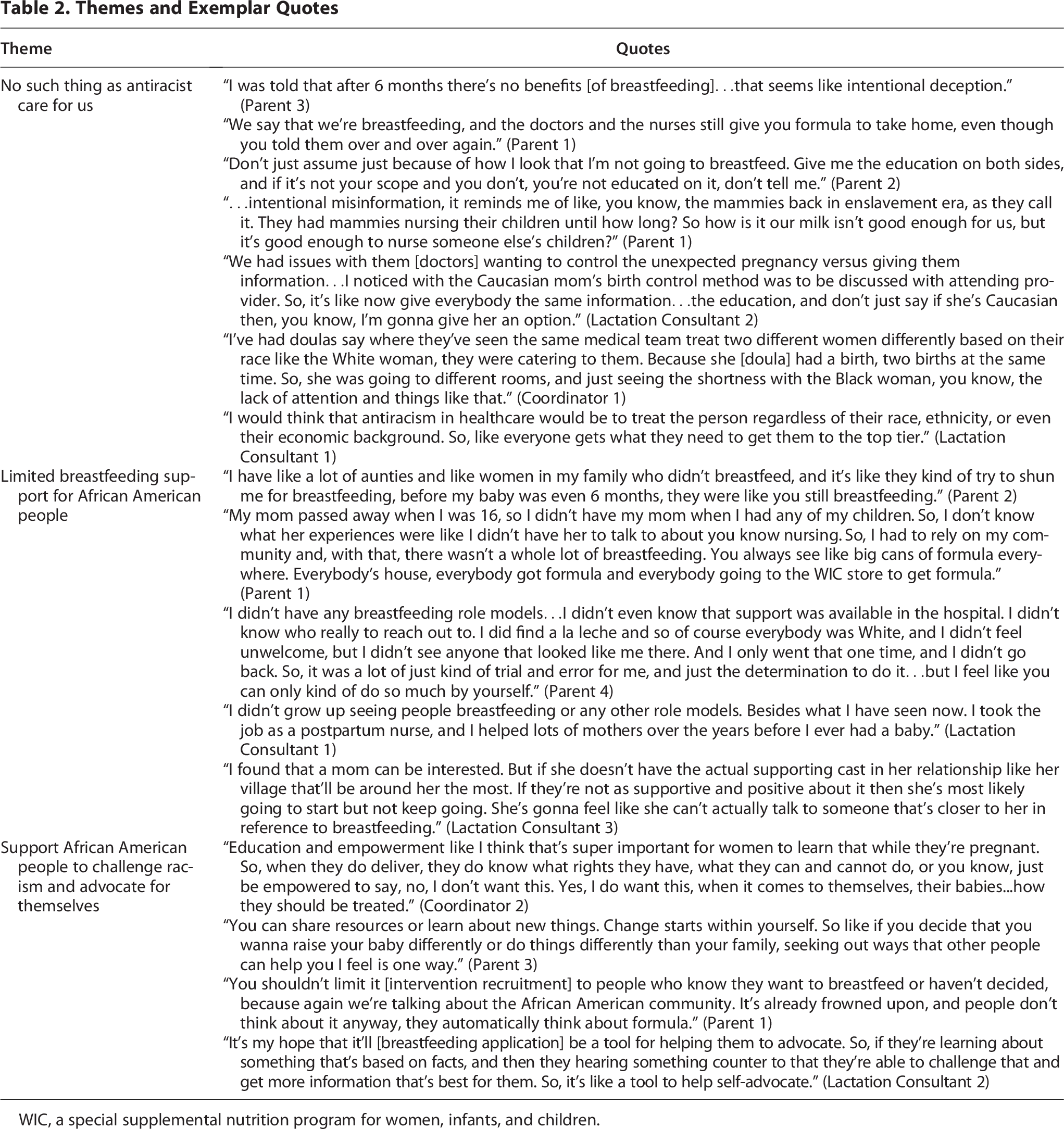
WIC, a special supplemental nutrition program for women, infants, and children.
Barrier 1: No Such Thing as Antiracist Care for Us
As members discussed how racism impacts breastfeeding among African American people, the mood changed from an upbeat to a solemn tone in the design studio sessions. The current racial climate regarding infant feeding was described as “unsupportive providers” and “assumptions that African American women are not interested in breastfeeding.” One parent expressed feeling “…they would just assume that I was gonna formula feed. So that’s another reason why I feel like it’s racial too.” This sentiment was also expressed by lactation professionals who noted that there was a significant lack of education provided to African American lactating people, which contributes to their limited knowledge about breastfeeding. This type of bias was experienced so frequently that many members felt providers were “oblivious that they’re actually doing it.”
The impact of bias was reinforced as lactation professionals noted providers would “promote birth control and order Depo” for low-income patients before discharge from the hospital without educating them that “it decreases [breast milk] when given before the milk supply has a chance to even be established.” It was “definitely an eye opener” to know that this was “common at more than just one hospital in this area.” In addition, misinformation was an issue as a parent described her frustration with unsupportive providers not only from her obstetrician assuming she would not breastfeed but also from a pediatrician. This led to the notion that “they’re intentionally making sure that our babies aren’t as healthy” and questioning “is there such a thing as antiracism.”
Barrier 2: Limited Breastfeeding Support for African American People
The collective experience of limited access to breastfeeding support for African American people was a significant issue discussed, which highlights the challenges that parents must successfully navigate to reach their breastfeeding goals. In addition to being faced with few lactation consultants within their communities for help with breastfeeding, some people also dealt with unsupportive families. This lack of resources, education, and connection with other breastfeeding people “has interfered with black people really knowing the benefits to breastfeeding” and makes it “hard to be encouraged to do so.” As a result, some members described efforts to rely on their “community” for breastfeeding support, which led to formula feeding exposure and concerns about inclusiveness. Nonetheless, a parent found support among her religious community as she noted, “I’m Muslim. We are encouraged to feed [breastfeed] our babies. We have certain classes for women and that will be a part of rearing our children…we want to give our children the absolute best for them.”
Solution: Support African American People to Challenge Racism and Advocate for Themselves
Members shared the collective notion that “knowledge is power for African American women.” As a result, members felt enthusiastic about allowing all African American people, regardless of parity, to participate in breastfeeding research. It was also highlighted that “race is something we can’t change,” so a solution is needed to help them realize the risks and challenges they may face as an African American person. Emphasis was placed on recruitment for research from a breastfeeding peer counselor and advocacy during pregnancy so that parents are better prepared to “use their voice” to champion the care they receive and have “time to talk with their village about what they’re learning.”
In the African American community, “language is important,” so they clearly understand the message presented and can relate to the information and learn to “advocate for themselves.” In this discussion, some members suggested that “the risks of not breastfeeding” should be presented to make human milk feeding the gold standard. While some professionals thought it was important to include language on the risks of formula feeding in the framing of the breastfeeding conversation, others felt there should be more focus on “positive reinforcement and praising the small victories” to encourage lactating people to sustain the duration of their breastfeeding efforts. This was a contrast to discussions in the parent group as it was stated, “I personally don’t think that they should even put risk on it at all [formula feeding].” Better language would be to include “fun facts” or “tidbits” to introduce information about the positive and negative facts about breastfeeding.
Discussion
This study centered on African American experiences to understand lactation care needs and gain insight to inform the redesign of a breastfeeding application prototype and mobile health intervention to advance health equity in breastfeeding support. The design thinking process augmented with the PHCRP provided the framework to guide bidirectional conversations with African American lactation professionals and parents in Chicago regarding needs, barriers, and a potential solution grounded by a race-conscious lens. This user-centered framework allowed us to systematically identify barriers specific to the advisory board members regarding unsupportive racial environments and limited access to adequate resources for lactation care. For a solution, advisory board members emphasized the need to prepare African American parents to use their voice and champion the care and support they receive. These results underscore the necessity of inclusive, participatory research to intentionally center the needs of people who have been marginalized and will be used to inform the improvement of a breastfeeding support application helping to move research from experiences to innovation that will better position technology for potential to reduce disparities in maternal health.
Like other research, our findings demonstrated that African American people and health care providers continuously report experiencing racism, bias, and discrimination that significantly impacts lactation care and outcomes that perpetuate low breastfeeding rates. Many African American people are exposed to biased care by health care providers based on the assumption that they prefer formula feeding. 7 The current racial climate in Chicago was identified as having no such thing as antiracist care and breastfeeding support for African American people was limited with misinformation preventing informed decision-making. Lactation consultants in this study identified biased care practices related to inadequate education about medroxyprogesterone acetate (Depo-Provera) administration prior to hospital discharge. Drawing on extensive clinical experience, advisory board members described a recurring pattern: African American parents who received the injection within 24–48 h after birth frequently experienced milk supply issues within weeks, despite adhering to all other evidence-based lactation recommendations. In contrast, White parents in their institutions were more consistently counseled about the potential impact of early administration before 6 weeks postpartum on lactation, thereby enabling truly informed decision-making. This disparity exemplifies how racialized knowledge production reinforces systemic biases with direct implications for health equity. 15 While these consultants’ clinical observations link early medroxyprogesterone acetate use to reduced milk supply, the timing of administration remains professionally contested. 22 A systematic review concluded that existing studies were of low methodological quality and insufficient to validate concerns regarding early postpartum initiation and milk production. 23 Nonetheless, both the World Health Organization 24 and the Academy of Breastfeeding Medicine 25 recommend delaying use until 6 weeks postpartum. Given that medroxyprogesterone is disproportionately utilized by African American individuals, 26 these findings call attention to the critical need for transparent clinical conversations that acknowledge the timing controversy, present all available evidence, and center patient autonomy in contraceptive decision-making. More evidence is also needed that includes a majority sample of African American individuals in medroxyprogesterone research.
Despite barriers faced, advisory board members identified a need for creating structural opportunities that support African American parents to directly challenge systemic racism and strengthen pathways for self-advocacy. Instead of focusing on empowering African American people, which implies the need to give them power to do something, the significance of supporting the very basic human right to make informed decisions stood out as key information to guide refinement of the breastfeeding application. This study also aligns with the call by Black Mamas Matter Alliance to include holistic care principles for the reenvisioning of maternal health research to achieve health equity. 27 We followed an ethical research design that included principles to address gaps in care, accessibility, trauma-informed concepts, and parent centeredness with a culturally informed design to highlight the voices of African American people. 27
Language used to frame breastfeeding was identified as an important factor to help birthing people relate to the information. However, there was disagreement between lactation professionals and parents about using language that includes the risk of not breastfeeding. While professionals thought it was important to frame education based on the risk of not breastfeeding to promote it as the gold standard, parents preferred to hear both the positive and negative facts about breastfeeding without using the word risk. This negative language highlights the preference of providers without considering the lived experiences of African American parents. Interventions designed from a top-down perspective intended for all birthing people do not meet the needs of diverse communities. More research is needed to explore the impact of educating on the risk of not breastfeeding as the standard practice compared to a focus on positive framing of breastfeeding benefits.
The small sample size is a limitation of this study and does not allow generalizability. Data were collected from adults living in the Chicagoland area, and the breastfeeding experiences of teens and parents in other geographical regions of the United States may be different. Although the advisory board included more lactation professionals than parents, they met separately to address the potential power differentials in perspectives that can influence communication. Nonetheless, the strength of this study includes being guided by the design thinking process and PHCRP, which focuses on human-centered design that is well-suited to develop interventions alongside users based on their needs rather than for them. This collaborative partnership with community members outside the academic environment is critical to achieving health equity. In addition, the PHCRP provided a race-conscious lens for data collection and analysis.
Health Equity Implications
Breastfeeding is an essential part of health for birthing people but is rarely seen as a reproductive or public health strategy to improve maternal morbidity and mortality. Thus, more research is needed that focuses on perinatal lactation to address the persistent disparities in breastfeeding support and education. 28 This study used the design thinking process augmented with the PHCRP to center the voices of African American people to identify a solution-based framework that addresses the persistent racial disparity in breastfeeding. This framework should continue to be used as the foundation for perinatal health equity research, as it provides an avenue to effectively consider the historical context that drives bias and demonstrates the extensive effects of discrimination on the health outcomes of birthing people. Evidence from this study bolsters racial equity through authentic engagement with an advisory board to gain insight into their reality, identify barriers, and create a potential solution to address racialized care practices. To eliminate breastfeeding inequities, health care systems must prioritize interventions that uphold the autonomous decision-making of African American parents, thereby confronting institutional racism and fostering self-determined advocacy. Thus, our findings will be used to continue this iterative process in design thinking to enhance a breastfeeding support application prototype with multiple components focused on improving lactation support through convenient access to professional and peer support, community resources, and education with culturally relevant language directed toward parent preferences. More research is needed to test the usability of a comprehensive breastfeeding support application to meet the needs of African American lactating parents.
Authors’ Contributions
U.T.J.: Conceptualization (lead), funding acquisition, methodology, investigation (lead), software, formal analysis (lead), writing—original draft, review, and editing (lead), visualization (lead), and supervision. M.K.C.: Project administration, investigation (supporting), formal analysis (equal), and writing—original draft, review, and editing (equal). T.H.: Formal analysis (equal) and writing—original draft, review, and editing (equal). P.S.: Conceptualization (supporting), validation (equal), formal analysis (supporting), writing—review and editing (equal), and visualization (equal). W.A.J.: Conceptualization (supporting), formal analysis (supporting), validation (equal), writing—review and editing (equal), and visualization (equal).
Footnotes
Author Disclosure Statement
The authors have no relevant financial or nonfinancial interests to disclose.
Funding Information
This research was funded by the Gordon and Betty Moore Foundation through Grant GBMF9048 to Rush University to support the work of U.T.J.