
Abstract
Background:
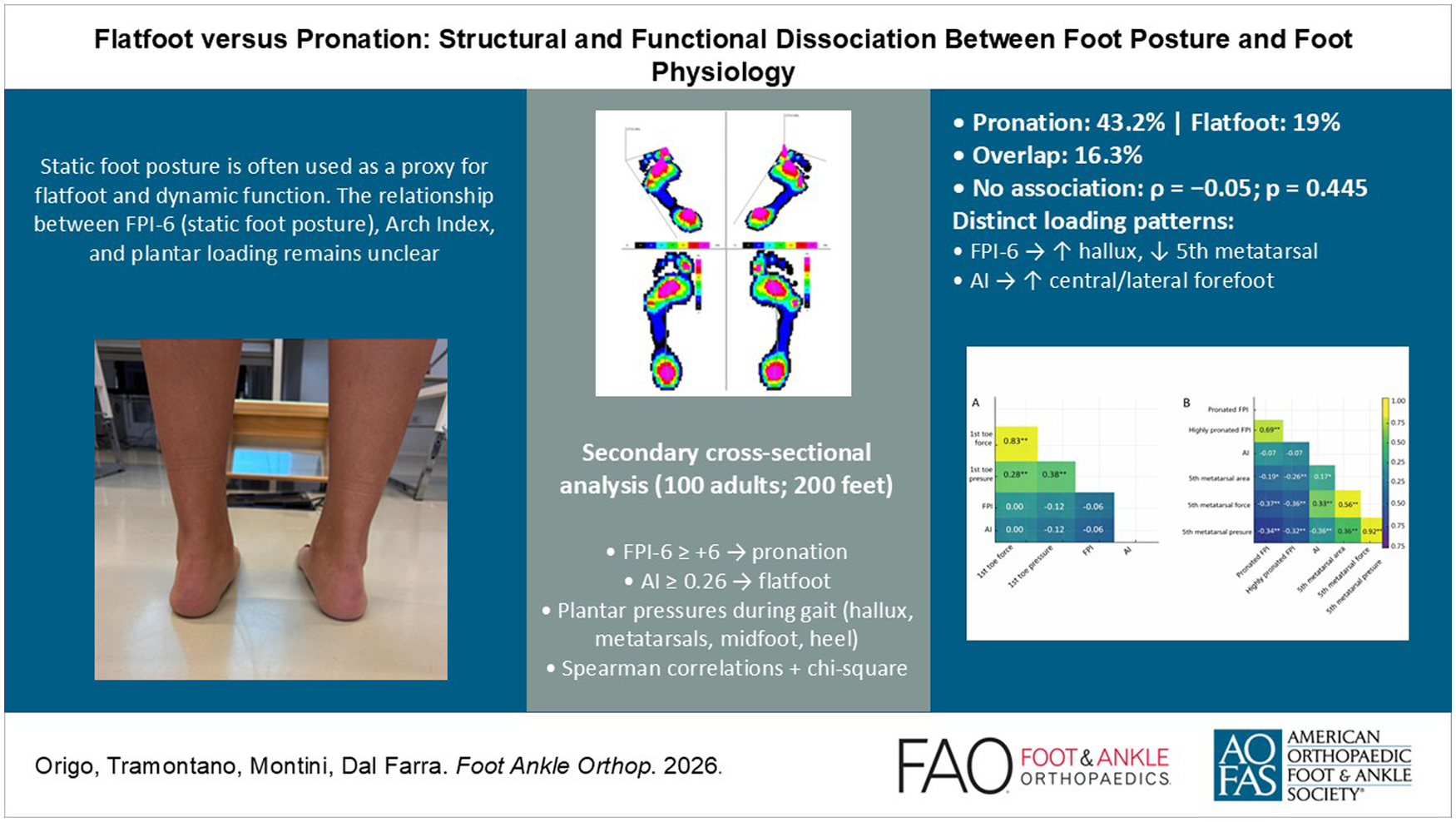
In clinical practice, static foot posture is frequently interpreted as a proxy for foot structure and function. The Foot Posture Index–6 (FPI-6) is a descriptive tool, often used to infer the presence of flatfoot and abnormal dynamic loading. However, the extent to which static pronation reflects structural arch collapse and functional plantar loading remains unclear.
Methods:
This secondary analysis examined the concordance between static foot posture (FPI-6), structural flatfoot assessed through the Arch Index (AI), and dynamic plantar loading during gait. Data were derived from a previously published cross-sectional data set including 100 healthy adults. Feet were classified as pronated when FPI-6 ≥ +6 and as flatfoot when AI ≥ 0.26. Dynamic plantar pressures were recorded during walking using a pressure platform, with regional peak pressures and vertical forces extracted for the hallux, metatarsals, midfoot, and heel. Associations between measures were explored using Spearman correlations and χ² tests.
Results:
Among 200 analyzed feet, 43.2% were classified as pronated by FPI-6, whereas only 19% met flatfoot criteria according to the AI. Overlap between classifications was limited, with only 16.3% of pronated feet also showing structural flatfoot. No statistically significant association could be detected between FPI-6 and AI (ρ = –0.05; P = .445).
Distinct dynamic loading patterns emerged, with higher FPI-6 scores associated with increased hallux loading and reduced fifth metatarsal loading, whereas higher AI values correlated with greater central and lateral forefoot loading. These patterns suggest limited concordance between static posture, structural morphology, and dynamic loading characteristics.
Conclusion:
In this asymptomatic sample, within the present data set, static pronation assessed with the FPI-6 was not significantly associated with structural flatfoot (P = .445) and showed limited concordance with dynamic plantar loading patterns. These findings should be interpreted with caution given the cross-sectional design and the potential nonindependence of bilateral observations. A multidimensional assessment integrating static posture, structural measures, and dynamic analysis may provide a more comprehensive framework for clinical evaluation.
Level of Evidence:
Level III, diagnostic, cross-sectional study.
Introduction
Accurate classification of foot posture is essential in both clinical practice and biomechanical research, as foot alignment is commonly used to characterize standing posture and to describe inter-individual variability in foot function. 1 Among the most widely used tools for static foot assessment is the Foot Posture Index–6 (FPI-6), which evaluates foot posture on a pronation-supination continuum through the observation of 6 anatomical features under weight-bearing conditions.1,2 Thanks to its ease of use, non-invasive nature, and variable inter-rater reliability reported in the literature, the FPI-6 has gained popularity in both research and clinical settings. 3
Although originally developed as a descriptive tool for static posture classification, the FPI-6 is often interpreted as a diagnostic indicator of flatfoot (pes planus), particularly when scores are equal to or greater than +6, despite limited empirical evidence supporting this inference. In this context, such thresholds should be considered as conventional reference values rather than definitive diagnostic criteria. Flatfoot is typically defined as a reduction in the medial longitudinal arch, often associated with increased midfoot contact area, sometimes with rearfoot valgus and in its flexible form, may coexist with ligamentous laxity or generalized joint hypermobility.4,5 It is important to distinguish between structural (rigid) flatfoot, characterized by a fixed reduction of the arch height even in non–weight-bearing conditions, and flexible flatfoot, in which the medial arch reappears when the load is removed or during toe-standing. The latter is common in children and many asymptomatic adults and generally represents a physiological variant rather than a pathological deformity. Foot pronation refers to a triplanar motion involving hindfoot eversion, forefoot abduction, and dorsiflexion, which may occur in both static and dynamic conditions. 6 These 2 constructs—flatfoot and pronation—are frequently conflated, yet they represent distinct biomechanical and diagnostic domains. Although pronation is a physiological component of gait, overpronation refers to an excessive or poorly controlled pronation, which may predispose to pathological loading patterns. Therefore, the distinction between overpronation and flatfoot is essential for clinical decision making. Confusing these entities may result in overdiagnosis and unnecessary treatment, particularly in asymptomatic or pediatric populations. A pronated foot does not necessarily imply structural arch collapse, just as a flatfoot deformity does not inherently present with excessive pronation during gait.6,7 A systematic review concluded that FPI-6 scores correlate only weakly with radiographic or morphological markers of arch flattening, and do not reliably reflect dynamic plantar loading patterns. 7 This extends our prior report showing weak/limited associations between FPI-6 and dynamic barefoot assessment. To objectively capture medial arch morphology, the Arch Index (AI) has been validated as a footprint-based metric. It is calculated as the ratio between the midfoot contact area and the total contact area, excluding the toes. AI values ≥0.26 are commonly used as reference thresholds for identifying structural flatfoot, although their interpretation should be considered in the context of methodological and population-specific variability.8,9 This index, however, does not account for neuromuscular adaptations or dynamic compensatory mechanisms. Functional assessment through baropodometric gait analysis allows for investigation of plantar pressure distribution across different foot regions, offering insights into dynamic loading and propulsion strategies.10,11 These parameters are critical for identifying functional overload syndromes and evaluating therapeutic interventions. Nonetheless, the relationship between static alignment, structural deformity, and dynamic function remains complex. It should be noted that more recent clinical frameworks, such as Progressive Collapsing Foot Deformity (PCFD), provide a broader and more comprehensive characterization of complex foot pathologies. The present study does not aim to define or diagnose PCFD, but rather to explore relationships between specific measurable dimensions in an asymptomatic population. The present study, based on a secondary analysis of previously published data, aims to examine the concordance between static pronation (FPI-6), structural flatfoot (Arch Index), and dynamic plantar loading. 12 We hypothesize that high FPI-6 scores do not consistently correspond to either structural arch collapse or pathological midfoot overloading, thereby supporting the need for a multidimensional diagnostic approach.
Methods
Study Design and Participants
This study is a secondary analysis of a previously published cross-sectional data set, reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.12,13 The original investigation was conducted between May 2021 and May 2022 and included 100 healthy adults recruited from an academic and clinical setting. The current analysis was designed to further explore the relationship between static pronation (FPI-6), structural flatfoot (AI), and dynamic plantar loading patterns.
No new data were collected for the present study. All analyses were performed on pseudonymized data originally obtained from the data set (protocol number: SIOM-AA0017). Inclusion criteria for the original study were as follows: age ≥18 years, absence of musculoskeletal disorders or lower limb injuries in the past 6 months, and ability to walk independently. Exclusion criteria included a history of foot surgery, neurological disease, or systemic rheumatologic conditions. All participants provided written informed consent before data collection. The original protocol was approved by the Institutional Review Board and complied with the ethical principles of the Declaration of Helsinki.
Foot Posture Assessment
Static foot posture was assessed using the FPI-6, a validated observational tool. In the original data set, 2 trained raters independently assessed the FPI-6. Inter-rater reliability was excellent (intraclass correlation coefficient = 0.97, 95% CI: 0.948-0.983). Given this high level of agreement, a consensus/average score per foot was used for the present analysis. Each foot was scored individually on 6 anatomical criteria under relaxed bipedal stance. Scores ≥+6 were classified as pronated.1 -3
Arch Index Calculation
AI was calculated from baropodometric footprints obtained during quiet standing. Static footprints were acquired on the same pressure platform with subjects standing quietly for ~5-10 seconds, arms alongside the body and gaze forward; toes were excluded from the contact area before computing AI as midfoot/total area. AI was defined as the ratio between the midfoot area and the total footprint area, excluding the toes. Values ≥0.26 were considered indicative of structural flatfoot. 4
Dynamic Plantar Pressure Analysis
Plantar loading patterns were evaluated during barefoot walking at self-selected speed on a pressure platform. Dynamic plantar pressures were collected using the Novel EMED n50 platform (2 sensors/cm²) and processed with EMED Professional Software, as in the primary study. Peak pressures and vertical forces were extracted for the hallux, metatarsals I-V, and midfoot regions, following standard foot masking protocols.11,12 Participants performed multiple barefoot passes; footprints with full contact were selected; 3 mid-gait steps per foot were averaged. Regions of interest included hallux, metatarsals I-V, midfoot, and heel. Peak pressure and total vertical force were extracted per region using a standard mask.
Statistical Analysis
Descriptive statistics are reported as mean ± SD or n (%). Spearman rank correlation coefficient (ρ) assessed associations between continuous variables (FPI-6, AI, regional loads). χ² test assessed the independence between dichotomized classifications (FPI ≥6 vs <6; AI ≥0.26 vs <0.26). Significance was set at P <.05. Given the multiple region-wise tests, analyses are exploratory; we report unadjusted P values and effect sizes (ρ). Each foot was considered as a separate observational unit to capture potential side-specific variability, as pronation and flatfoot are clinically defined at the level of the individual foot and may differ within the same subject. Although this approach is commonly adopted in foot biomechanics research, bilateral feet from the same participant may exhibit within-subject correlation, which should be considered when interpreting the results.
Results
Sample Characteristics
The study included 100 adults (mean age 32.15 ± 7.49 years, with 61 men and 39 women). Demographic and clinical characteristics of the participants are reported in Table 1.
Demographic and Clinical Characteristics of the Participants (N = 100).
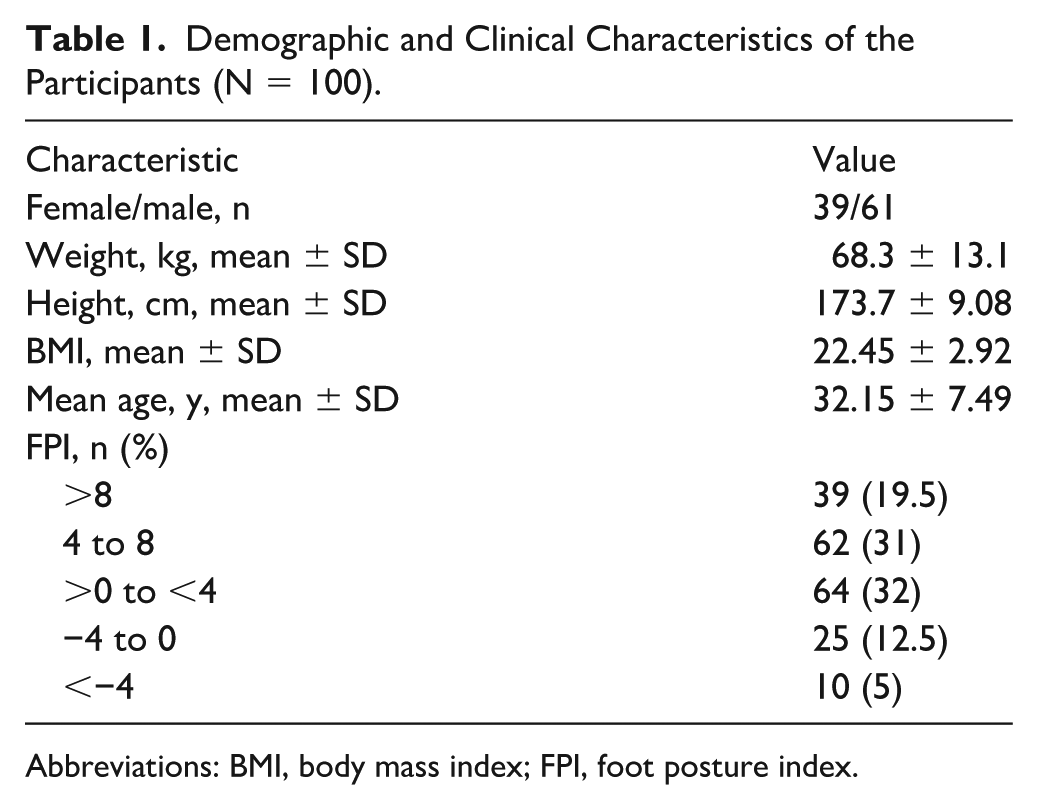
Abbreviations: BMI, body mass index; FPI, foot posture index.
Foot posture and arch morphology
Overlap was minimal, with only 14 of 86 pronated feet (16.3%) also classified as flatfoot according to the AI. FPI-6 and AI showed no statistically significant association within the present data set (Spearman ρ = –0.05, P = .445; χ² = 0.78, P = .378; OR 1.39, 95% CI 0.669-2.87). Further details concerning the analyzed feet are described in Table 2.
Descriptive Statistics of the Analyzed Feet.
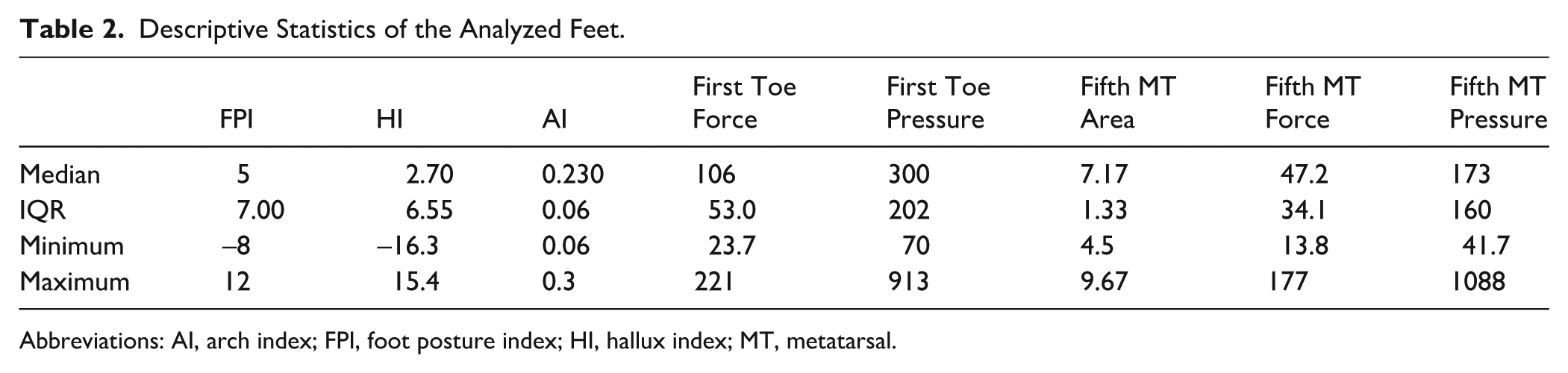
Abbreviations: AI, arch index; FPI, foot posture index; HI, hallux index; MT, metatarsal.
Dynamic plantar pressure analysis
Dynamic plantar loading patterns were analyzed. Higher FPI-6 scores were associated with greater hallux loading (ρ = 0.38, P < .001) and reduced fifth metatarsal loading (ρ = –0.34, P < .001). Conversely, higher AI correlated with greater lateral/central forefoot loading, including fifth metatarsal (ρ = 0.33-0.36, all P < .001). These associations indicate distinct loading strategies for pronation vs structural flatfoot. All results are reported in Tables 3 and 4 and illustrated in Figures 1 and 2.
Associations Between FPI and AI: Correlation and Categorical Analysis.
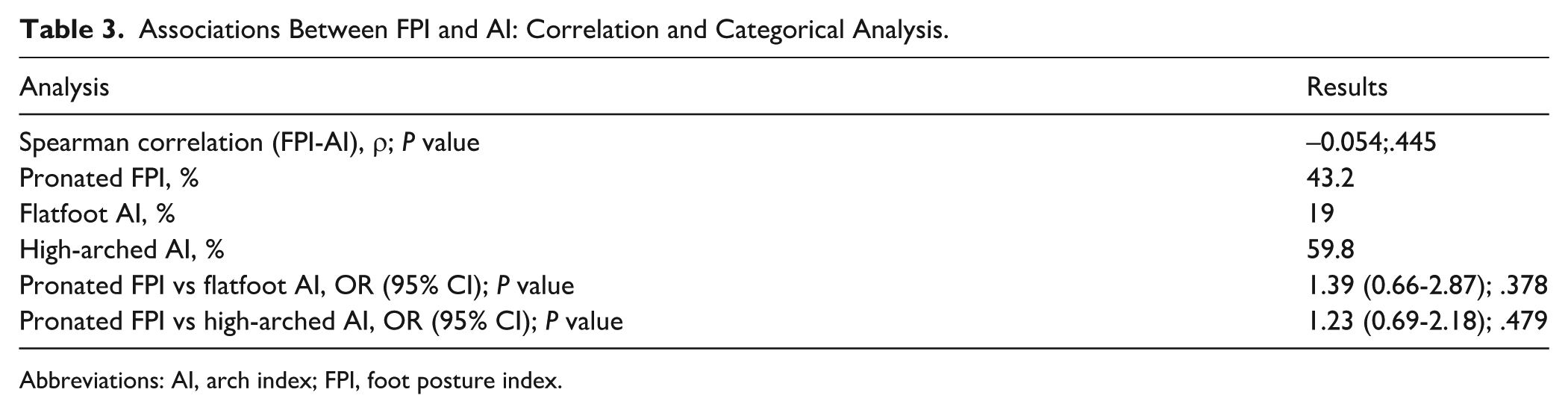
Abbreviations: AI, arch index; FPI, foot posture index.
Spearman Correlations Between Clinical Measures and Regional Plantar Loading Variables.
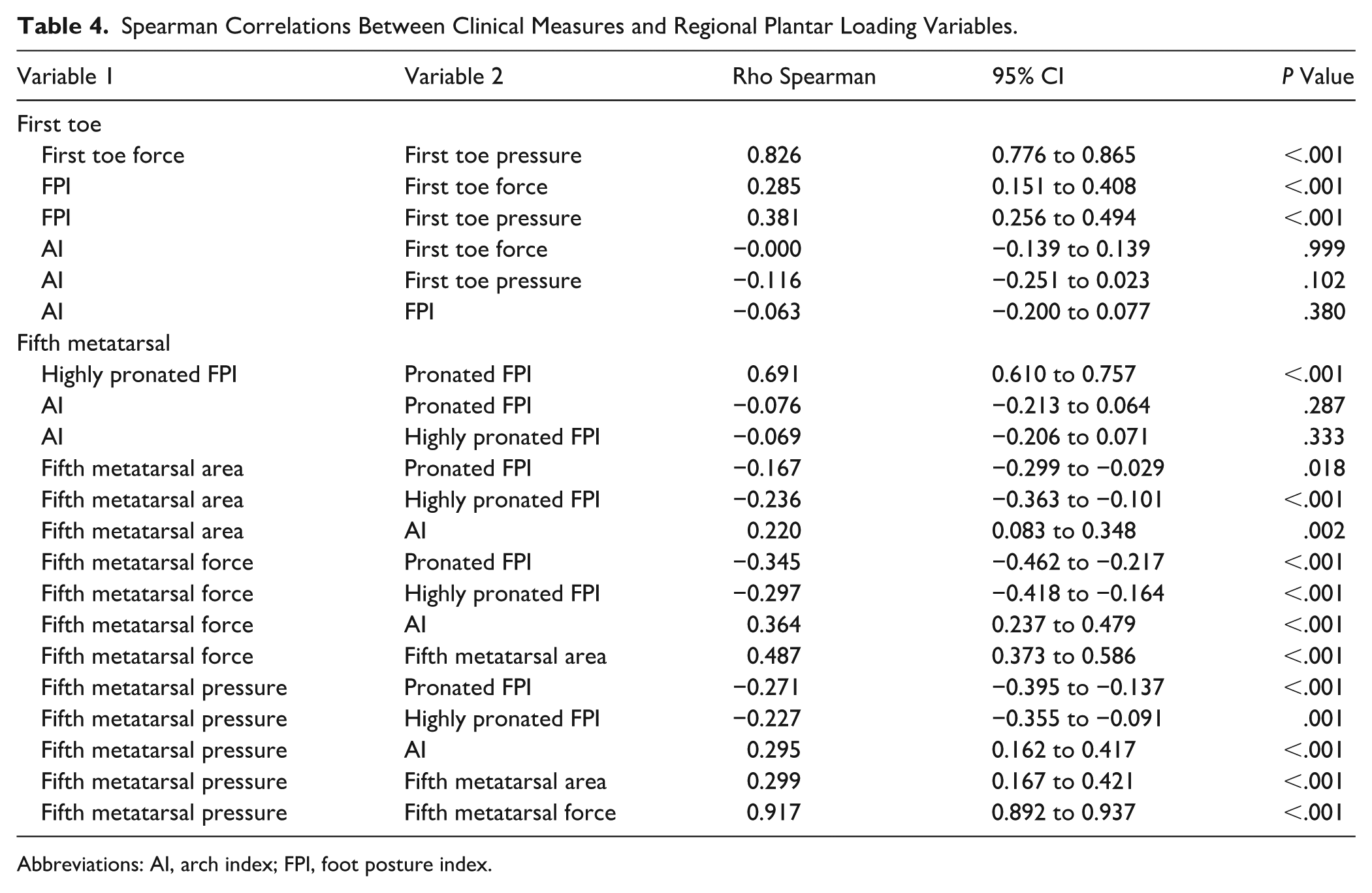
Abbreviations: AI, arch index; FPI, foot posture index.
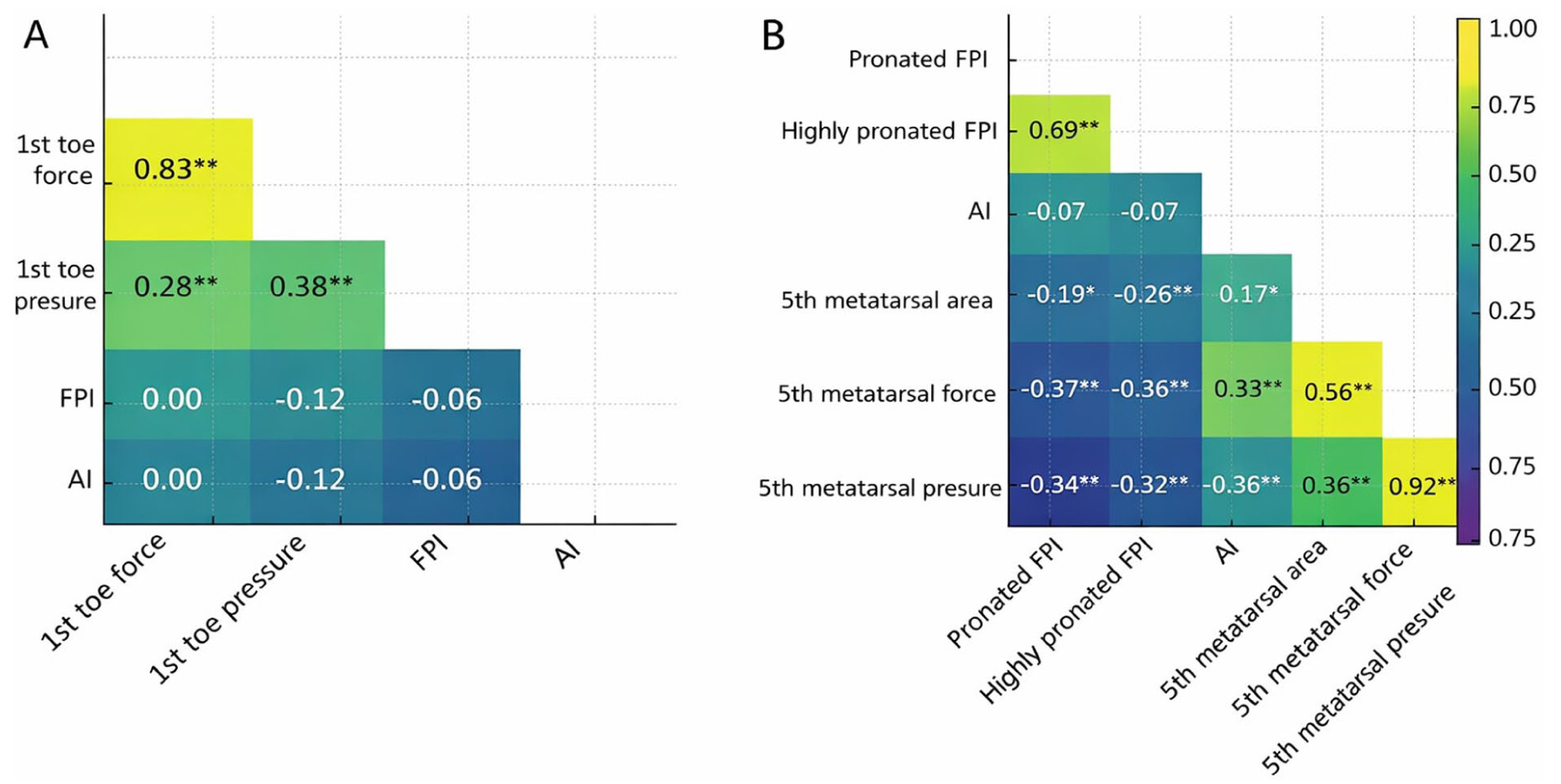
Heatmaps of Pearson correlation coefficients illustrating the relationships between clinical measures (FPI, AI) and regional plantar loading variables. Panel (A) refers to the first toe, whereas panel (B) refers to the fifth metatarsal. Variables include force, pressure, and, for the fifth metatarsal, contact area. Each cell displays a correlation coefficient (r), with color gradients indicating direction and magnitude (yellow = positive; blue = negative). This visualization allows rapid identification of association patterns across multiple variables. Asterisks denote statistical significance (*P < .05; ** P < .01). AI, arch index; FPI, foot posture index.
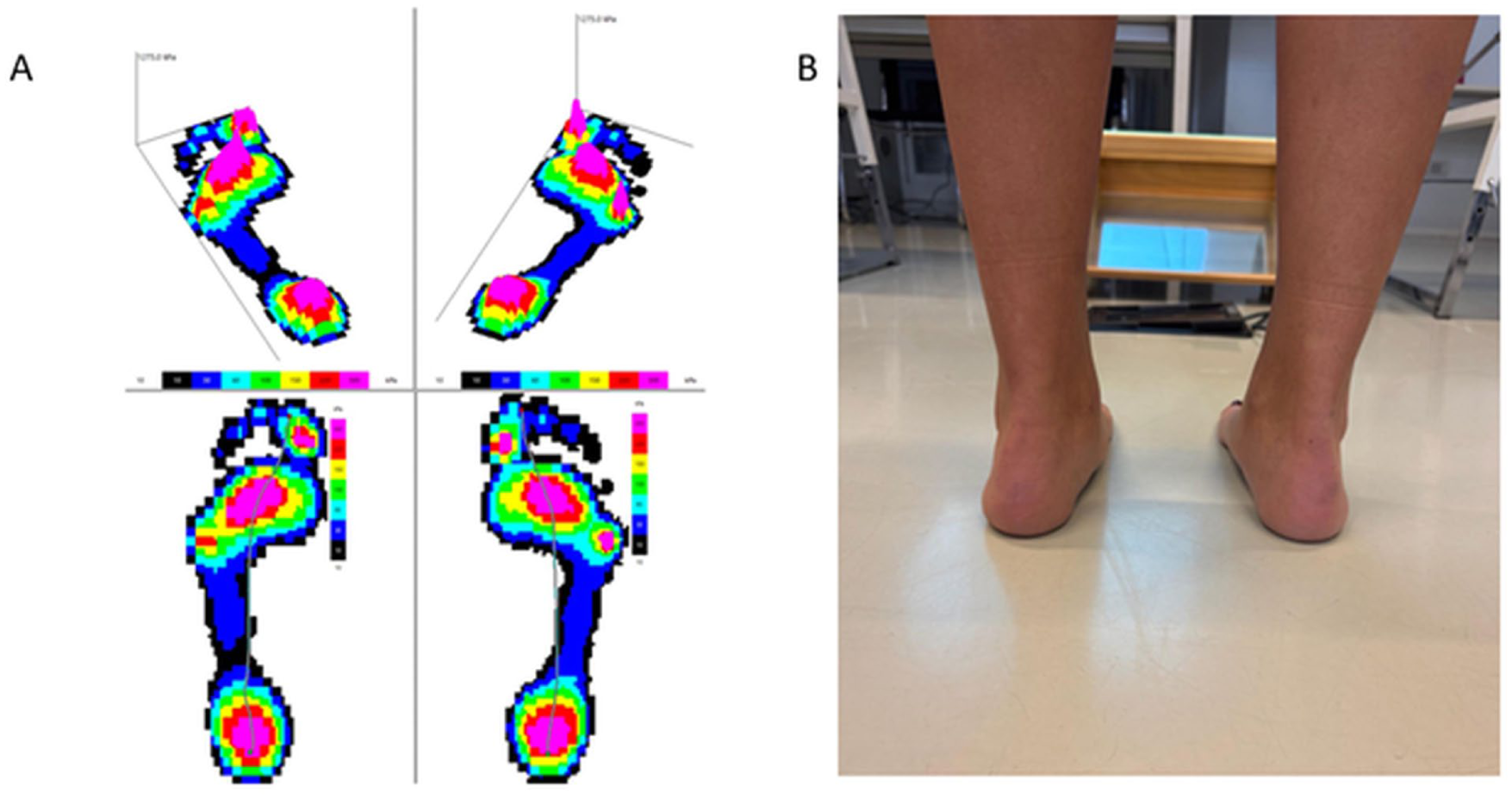
Representative example demonstrating the dissociation between dynamic plantar loading and static foot posture. (A) Pedobarographic assessment showing plantar pressure distribution during stance. Increased midfoot contact area is consistent with a flatfoot pattern. (B) Clinical posterior view of the same subject. The foot does not exhibit marked pronation despite the flatfoot pattern observed in the pedobarographic image. This figure illustrates how structural flatfoot and clinical pronation may not overlap.
Discussion
This study aimed to evaluate the concordance between static foot posture (FPI-6), structural flatfoot (Arch Index), and dynamic plantar loading patterns. The results showed limited concordance between these domains. Although 43.2% of feet were classified as pronated according to the FPI-6, only 19% met flatfoot criteria based on the Arch Index, with minimal overlap between classifications (16.3%). In addition, no statistically significant association could be detected between FPI-6 and AI within the present data set (ρ = –0.05, P = .445).
These findings extend previous observations suggesting that static foot posture, structural morphology, and dynamic function represent related but not interchangeable dimensions of foot assessment. Prior studies have shown that individuals with flat-arched feet may exhibit normal gait kinematics, whereas pronated postures may coexist with structurally preserved arches.14,15 Our results are consistent with this framework and support a cautious interpretation of static posture measures when used in isolation. This limited concordance is also illustrated by the representative example shown in Figure 2.
From a clinical perspective, these findings have implications for the interpretation of foot posture assessments. The use of FPI-6 as a proxy for flatfoot may lead to misclassification, particularly in asymptomatic individuals or in cases of flexible foot posture. This may contribute to overestimation of flatfoot prevalence and potentially unnecessary interventions. From a research standpoint, conflating static posture with structural flatfoot may introduce heterogeneity in study samples and obscure associations between morphology, loading patterns, and symptoms. A multidimensional approach incorporating static alignment, structural measures, and dynamic assessment may therefore provide a more accurate basis for interpretation. These findings may have implications for clinical decision making, particularly in avoiding overinterpretation of static posture as a proxy for structural or functional impairment.
Our findings further support the view that static foot posture classification does not necessarily reflect structural arch morphology. These results highlight a potential source of diagnostic ambiguity. Interpreting FPI-6 scores as synonymous with flatfoot may lead to misclassification, particularly in individuals with flexible flatfoot or ligamentous laxity. 16 In such cases, the medial arch may appear reduced during stance but reconstitute when the load is removed or during heel rise. This flexibility may reflect a physiological adaptation rather than a pathological deformity and may coexist with increased pronation because of generalized ligamentous laxity or reduced passive stiffness of the medial arch structures. Recognizing this distinction may help avoid unnecessary orthotic prescription and support a more function-oriented clinical approach. The analysis of dynamic plantar loading further highlighted distinct functional patterns. Higher FPI-6 scores were associated with increased hallux loading and reduced fifth metatarsal loading, suggesting a medialized propulsion strategy. In contrast, higher Arch Index values were associated with increased loading in central and lateral forefoot regions. These divergent patterns further support the view that static pronation and structural flatfoot may reflect different biomechanical adaptations rather than a single underlying construct.17,18
In light of these results, overpronation may predispose to sesamoid disorders, whereas structural flatfoot may underlie central forefoot overload.19,20
It should be emphasized that plantar pressure assessment during barefoot walking at self-selected speed does not represent a comprehensive gait analysis and cannot be directly extrapolated to predictive or surgical outcomes. In this context, dynamic plantar pressure measurements should be interpreted as a functional proxy of loading patterns rather than a full representation of gait biomechanics.
Structural flatfoot showed a positive association with lateral forefoot loading. This pattern further suggests that arch morphology and pronation-related loading should not be assumed to represent the same biomechanical process.
Overall, these findings support a multidimensional framework for foot assessment, in which static posture, structural morphology, and dynamic loading are considered jointly rather than interchangeably.21 -24 In this context, static tools such as the FPI-6 may be useful for descriptive classification, but should not be used alone to infer structural flatfoot or dynamic function. 25 Furthermore, pronation—particularly in the context of complex clinical conditions such as PCFD—should be considered a multifactorial phenomenon involving structural, neuromuscular, and functional components, which cannot be fully captured by isolated measures such as FPI-6, Arch Index, or plantar pressure analysis alone.
These findings should be interpreted with caution, particularly considering the potential within-subject dependence of bilateral observations.
Limitations
Several limitations should be acknowledged. First, the cross-sectional design precludes any causal inference. Second, the Arch Index is derived from 2-dimensional footprint data and may not fully capture the 3-dimensional complexity of the medial longitudinal arch. Third, the use of an asymptomatic population allowed the investigation of biomechanical relationships in the absence of confounding factors such as pain or functional impairment but limits the generalizability of the findings to symptomatic conditions, including progressive collapsing foot deformity (PCFD).
Fourth, each foot was analyzed as a separate observational unit; however, bilateral feet from the same participant are not statistically independent and may introduce within-subject correlation (clustering effects). Future studies should consider clustered or multilevel analytical approaches to appropriately account for this dependency structure.
Finally, the analyses were exploratory and involved multiple comparisons; therefore, results should be interpreted with caution, with greater emphasis on effect sizes and consistency of patterns rather than isolated P values.
Conclusions
In this sample of asymptomatic adults, within the present data set, static foot posture assessed with the Foot Posture Index–6 (FPI-6) was not significantly associated with structural flatfoot as defined by the Arch Index (P = .445) and showed limited concordance with dynamic plantar loading patterns. These findings suggest that static posture, structural morphology, and functional loading represent related but distinct dimensions of foot assessment.
From a clinical perspective, interpreting pronation as synonymous with flatfoot may lead to misclassification, particularly in individuals with flexible or asymptomatic foot presentations. The present results support the need for a cautious and multidimensional approach to foot evaluation, integrating static, structural, and dynamic assessments.
Given the cross-sectional design, the use of an asymptomatic population, and the potential non-independence of bilateral observations, these findings should be interpreted with caution. Further research using clustered analytical approaches and including symptomatic populations is warranted to better clarify the clinical relevance of these relationships.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261451239 – Supplemental material for Flatfoot vs Pronation: Structural and Functional Dissociation Between Foot Posture and Foot Physiology
Supplemental material, sj-pdf-1-fao-10.1177_24730114261451239 for Flatfoot vs Pronation: Structural and Functional Dissociation Between Foot Posture and Foot Physiology by Daniele Origo, Marco Tramontano, Gabriele Montini and Fulvio Dal Farra in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
This study is a secondary analysis of a previously published cross-sectional data set. The original study protocol was reviewed and approved by the SOMA Institutional Review Board (SOMA Institute, Milan, Italy; protocol number: SIOM-AA0017) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. No additional ethical approval was required for the present secondary analysis, as no new data were collected and all data were analyzed in a pseudonymized form.
Consent to participate
Written informed consent to participate was obtained from all participants prior to data collection in the original study.
Consent for publication
All participants provided written informed consent for the use and publication of their anonymized data. No identifiable personal information is included in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data availability Statement
The data sets generated and analyzed during the current study are not publicly available because of ethical and institutional restrictions but are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.