
Abstract
Introduction
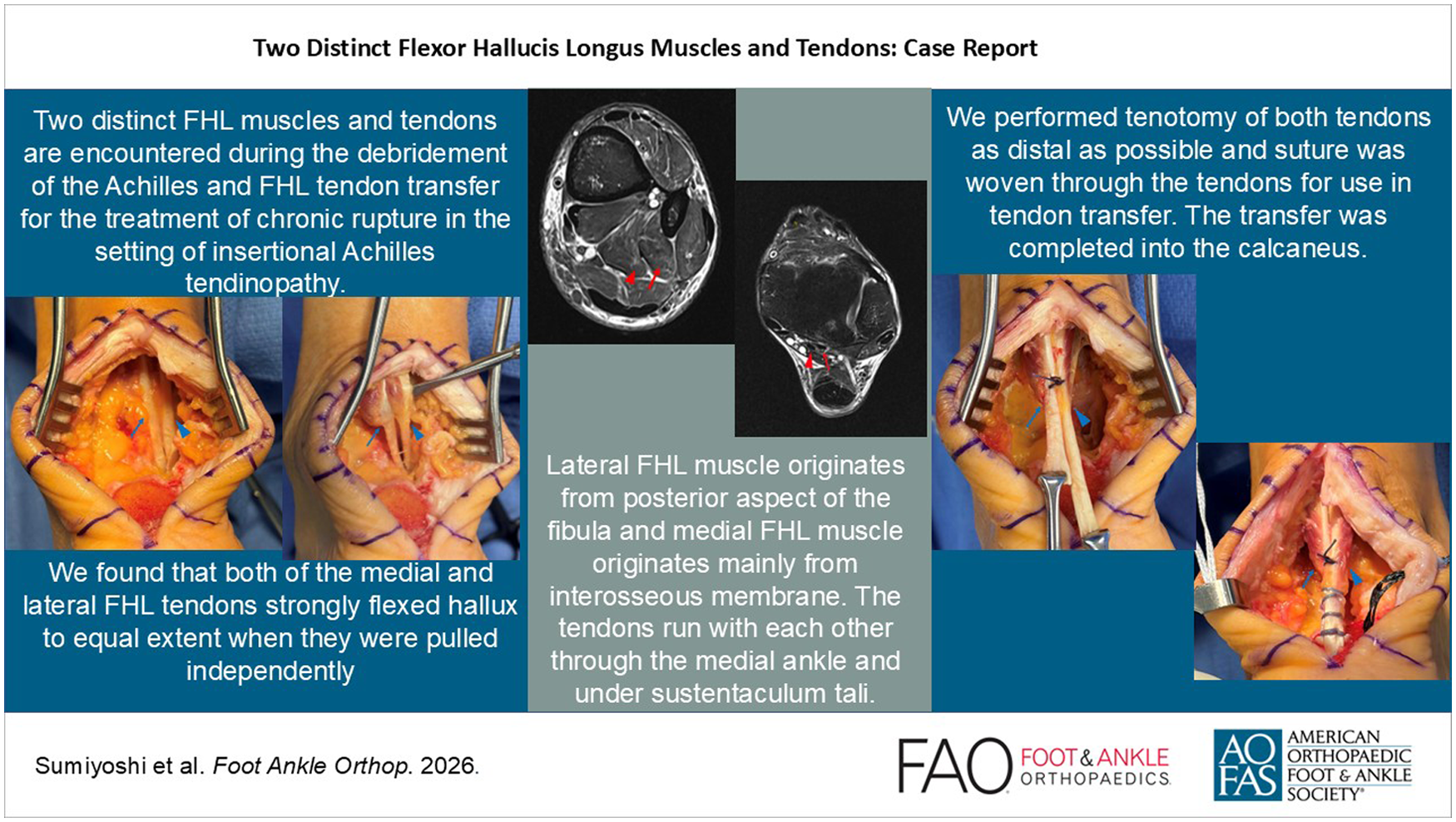
The flexor hallucis longus (FHL) tendon is a strong great toe flexor muscle in the deep flexor compartment of the leg. It originates from the distal two-thirds of the posterior fibula and interosseous membrane and inserts on the inferior surface of the distal phalanx of the hallux. The FHL often has tendinous slips to the lesser toes, and there are anatomical variations in its crossing to the flexor digitorum longus (FDL) in the plantar foot.5,12 It also contributes to flexion of the lesser toes.6,8 The FHL tendon is often harvested and used in secondary Achilles tendon reconstruction, to compensate for Achilles tendon weakness, especially in the older population. 9 The reported variations in FHL anatomy are generally distal to the sustentaculum tali.5,12 To our knowledge, anatomical variants or anomalies of the FHL tendon proximally to the subtalar joint are not previously clearly described. Here we present a case of 2 distinct FHL muscles and tendons encountered during the debridement of the Achilles and FHL tendon transfer for the treatment of chronic rupture in the setting of insertional Achilles tendinopathy.
Case Report
A 66-year-old woman presented with left Achilles pain for about 6 months. She was in her usual state of health and walking when she felt a sudden pain in her Achilles 6 months prior to presentation. She had attempted to resume her usual activities, but she remained limited. She had tried physical therapy, boot, and orthoses prior to evaluation. She had a remote history of ipsilateral plantar fasciitis for which she did physical therapy and wore an ankle foot orthosis (AFO), with symptomatic improvement. On physical examination of the left ankle, she had tenderness in Achilles insertion. Ankle range of motion was maintained, and Thompson test was negative. Motor examination showed 5/5 strength on dorsiflexion, plantarflexion, eversion, and inversion. On standing, she had neutral hindfoot and forefoot in alignment. She was able to perform bilateral heel raise with appropriate hindfoot inversion. Anteroposterior, lateral, and oblique weightbearing radiograph of the left ankle and foot (Figure 1) revealed an insertional calcification of the Achilles and plantar fascia, and Haglund deformity. A 3-tesla (T) magnetic resonance imaging (MRI) scan of the left ankle (Figure 2) showed insertional Achilles degeneration and swelling, near-complete tear of the Achilles at its insertion, Achilles insertional calcification, and Haglund deformity.
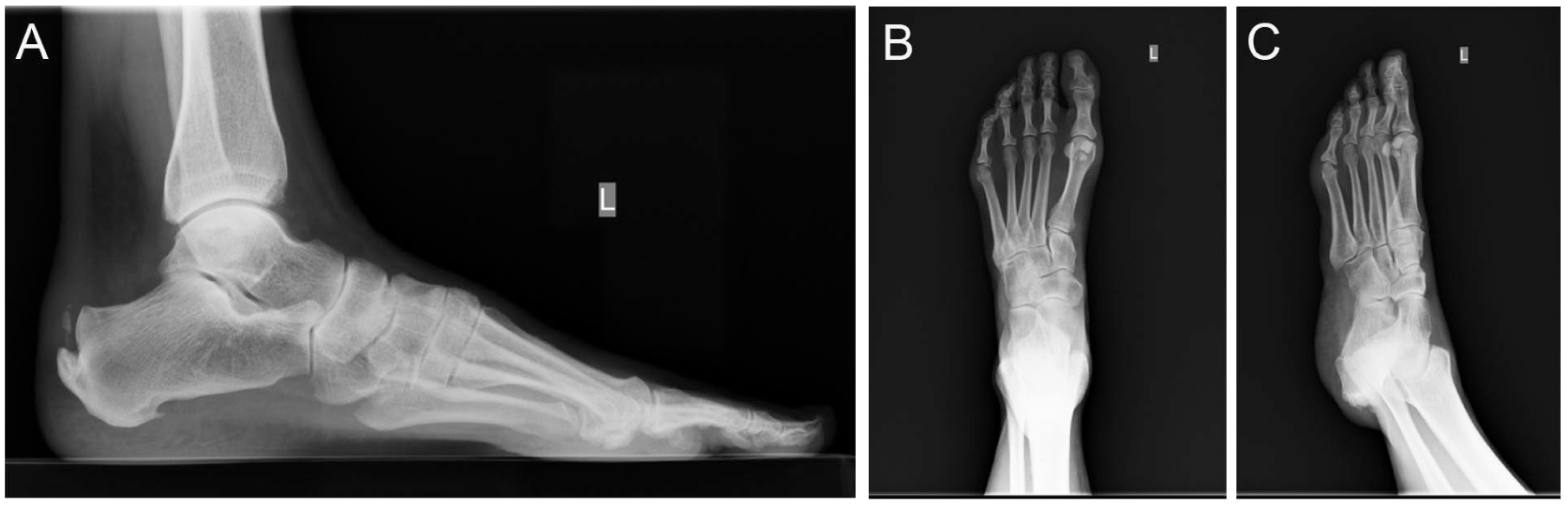
Preoperative weightbearing radiograph of the left foot, (A) lateral, (B) anterior-posterior, and (C) oblique views, shows insertional calcification of the Achilles and plantar fascia, and Haglund deformity.

Preoperative 3-T magnetic resonance image of the left ankle: (A) sagittal short tau inversion recovery (STIR) imaging, and (B) axial T2-weighted fat saturated imaging shows significant insertional Achilles degeneration and swelling. Red circle shows a near-complete tear of the Achilles tendon at its insertion to the calcaneus.
She presented having exhausted nonoperative options, and she wished to proceed with surgery because of inability to resume sports. A debridement of the insertion of the Achilles and its calcifications, Haglund’s resection, secondary repair, and FHL tendon transfer were planned.
A direct posterior approach was chosen for surgery, with the patient positioned prone. The distal portion of the Achilles showed near complete rupture with insertional enthesopathy and degeneration. When attention was turned to the FHL tendon for harvest, we found 2 distinct FHL muscles as well as tendons (Figure 3). When elevating and pulling up each FHL tendon with a retractor, each tendon strongly flexed hallux, with more limited flexion of the 2-5 toes (presumably through the master knot of Henry). After anatomical evaluation of each FHL tendon by visualizing the course of the tendon in relationship to tibia, talus, calcaneus, FDL, and the neurovascular bundle, we concluded that we have 2 distinct FHL tendons. Most importantly, we found that both of the medial and lateral FHL tendons strongly flexed the hallux to an equal extent when they were pulled independently, which further confirmed that they were both FHL tendons anatomically and functionally. We then performed tenotomy of both tendons as distal as possible and suture was woven through the tendons for use in tendon transfer. The transfer was completed into the calcaneus. Postoperatively, the wound healed without any issue, the patient was splinted in plantarflexion and continued nonweightbearing for 4 weeks in total, followed by graduated weightbearing with Achilles boot as our usual Achilles recovery protocol. At the subsequent follow-up visits, the patient did not have any weakness in hallux or lesser toes and returned to normal activity level without any complication after physical therapy.

Intraoperative picture of the left foot showing 2 distinct FHL tendons. (A) Intraoperative picture of the left foot after resection of the Haglund deformity, before harvesting the FHL tendons. Arrowhead shows the medial FHL muscle and tendon. Arrow shows the lateral FHL muscle and tendon. (B) Intraoperative picture showing clear muscle bellies of 2 distinct FHLs, lifted with a freer elevator. Arrowhead shows the medial FHL muscle and tendon. Arrow shows the lateral FHL muscle and tendon. (C) Intraoperative picture after resection of the 2 FHL tendons as distal as possible from the posterior incision. Arrowhead shows the medial FHL muscle and tendon. Arrow shows the lateral FHL muscle and tendon. (D) Intraoperative picture after fixation of the FHL tendons into the tunnel created in the calcaneus. Arrowhead shows the medial FHL muscle and tendon. Arrow shows the lateral FHL muscle and tendon. (E) Enlarged image of the 2 FHL tendons after fixation. Arrowhead shows the medial FHL muscle and tendon. Arrow shows the lateral FHL muscle and tendon. FHL, flexor hallucis longus.
Discussion
This case presents a rare anatomical variant characterized by 2 distinct FHL muscles and tendons, confirmed intraoperatively to function independently. The FHL is a strong flexor of the hallux and contributes to ankle plantarflexion. At its position between the posterior tubercles of the talus, it can cause ankle pain related to tendinopathy or with direct compression of the os trigonum. In regard to the FHL muscle and tendons, some new findings are reported in recent studies. Swanson et al 10 reported that the FHL muscle belly extended distal to the distal aspect of the tibia in more than 90% of the pediatric population between 8 and 18 years old, which is more distal than previously reported. 11 Michelson et al 7 reported that stenosing FHL synovitis can cause increased intraarticular loading in the hallux metatarsophalangeal joint and possibly contributes to hallux rigidus symptoms. Beyond its pathology, the FHL tendon is frequently used for tendon transfers, such as the Achilles or peroneus brevis.
The FHL tendon is known to give branches to the FDL and contributes to flexion of the lesser toes in addition to its primary function as a hallux flexor.4,6,8,12 Edama et al 5 reported classification of the connections of FHL tendon slip to the lessor toes through a cadaveric study of 116 legs. They reported that 33% of legs had a connection from the FHL to toe 2, 53% had connections from the FHL to toes 2 and 3, and 15% had connections from the FHL to toes 2-4 though the FDL tendons.
Our case had 2 distinct FHL muscles and tendons. Retrospectively, further evaluation of the MRI clearly showed the 2 distinct FHL muscles and tendons (Figure 4). Although those muscles were lying next to each other, the lateral FHL muscle originated from the posterior fibula, and the medial FHL muscle originated mainly from the interosseous membrane. The tendons run with each other through the medial ankle and under the sustentaculum tali. Even though MRI distinction is more difficult distally, the lateral FHL tendon appears to branch off to the FDL at the master knot of Henry, whereas the medial FHL tendon appears to directly insert into the distal phalanx of the hallux. As we used a more proximal incision for FHL tendon harvesting, the definitive relationship between the FHL and FDL tendons more distally is not fully known, limiting our ability to fully characterize the distal anatomical connections. However, there were a few findings that clearly differentiated these 2 FHL tendons from accessory slips or variant muscle contributions that were already known in the literature.

Preoperative magnetic resonance image of the left ankle. (A) Axial STIR image at the level of tibiotalar joint shows 2 distinct FHL tendons. Arrowhead shows the medial FHL muscle. Arrow shows the lateral FHL muscle. (B) Axial STIR image 60 mm proximal to tibiotalar joint shows that the lateral FHL muscle originates from posterior aspect of the fibula and medial FHL muscle originates mainly from interosseous membrane. Arrowhead shows the medial FHL muscle. Arrow shows the lateral FHL muscle. FHL, flexor hallucis longus; STIR, short tau inversion recovery.
One of the known anatomical variations in the posteromedial aspect of the ankle and foot is flexor digitorum accessorius longus, and its prevalence is reported to be 6% to 8%. 3 The muscle can arise from any structure in the posterior compartment and courses beneath the flexor retinaculum, through the tarsal tunnel, superficial to the neurovascular bundle, and typically inserts onto the quadratus plantae or flexor digitorum longus.1,3 Because of the location of its insertion, the flexor digitorum accessorius longus would not strongly flex the hallux like the 2 FHL tendons did in our case, even with the possible existence of indirect connections at the master knot of Henry. Furthermore, the flexor digitorum courses superficial to the neurovascular bundle; on the other hand, both of the 2 FHL tendons in our study are located deep and lateral to the neurovascular bundle throughout their course (Figure 4).
Another rare anatomical variation in the posteromedial ankle and foot is peroneocalcaneus internus (PCI) muscle, and its prevalence is reported to be 1%. 2 The PCI arises from the internal aspect of the fibula and descends posterior to FHL, displacing it anteriorly and medially, with the tendons running parallel. 1 The PCI inserts on a small tubercle on the medial aspect of the calcaneus, below the sustentaculum. 1 In our case, the 2 FHL tendons were located side to side each other throughout the course, and both of the FHL tendons attached to hallux, and strongly plantarflexed it. The 2 FHL tendons were clearly different from the PCI muscle because PCI inserts into the calcaneus below the sustentaculum, and it would not flex the hallux. 1
Conclusion
To our knowledge, this is the first case report of the 2 distinct FHL muscles and tendons in the literature. The anatomical and functional features of the 2 distinct FHLs clearly differed from other anatomical variations in the posteromedial aspect of the ankle and foot. We used both FHL tendons for the transfer to augment the Achilles chronic rupture repair with good clinical outcome without any complication. When encountering unexpected anomalous FHL anatomy during surgery, functional verification of the tendon’s function can help guide intraoperative decision making.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261433963 – Supplemental material for Two Distinct Flexor Hallucis Longus Muscles and Tendons: Case Report
Supplemental material, sj-pdf-1-fao-10.1177_24730114261433963 for Two Distinct Flexor Hallucis Longus Muscles and Tendons: Case Report by Nobuhiko Sumiyoshi, Chielozor I. Okafor and Casey Jo Humbyrd in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval was not sought for the present study because this manuscript is based on a single case. Written informed consent for patient information and images to be published was provided by the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.