
Abstract
Background/Purpose
To investigate the relationship between anatomical variation of the toe flexor muscles and the resulting variation of toe flexion angle from tendon excursion.
Methods
Six cadaveric lower extremities preserved by Thiel’s embalming method were evaluated. The toe flexor muscles were distracted individually and toe flexion angles measured. The anatomic variation were observed by gross anatomical dissection.
Results
The toes with tendinous slips of flexor hallucis longus (FHL) showed similar flexion angles between the FHL and flexor digitorum longus. However, there were differences observed regarding toe flexion and tendon excursion of the flexor digitorum muscle and quadratus plantae due to the anatomic variations.
Conclusion
The anatomical variation of the toe flexor muscles should be taken into account when evaluating toe function and applying exercise therapy for foot disorders.
Keywords
Introduction
The toe flexor muscles play a key role in postural control and propulsion.1–4 Toe flexor strength is important for lower limb physical performance. 5 Increasing toe flexor strength contributes to improvement in physical performance. 6 Reduced toe flexor strength increases the risk of falling in the elderly.7,8 Understanding toe flexor muscle function is relevant to both physical performance and risk of falling.
Anatomical variation of the toe flexor muscles in the chiasma plantae has previously been reported.9–21 The flexor hallucis longus muscle (FHL), the flexor digitorum longus muscle (FDL), and the quadratus plantae (QP) blend in various fashion in the chiasma plantae. 20 The FHL most often have tendinous slips which form the long flexor tendons to the lesser toes along with tendons of the FDL. The insertion of the QP to the long toe flexor tendon and of the flexor digitorum brevis (FDB) to lesser toes also vary anatomically.20,22,23
The FDL and FHL are utilized for tendon transfer surgeries for foot disorders such as flatfeet. The tendinous slip of the FHL should compensate the function of the lesser toes following FDL tendon transfer. Less understood is the function of the tendinous slip of the FHL. There is limited information regarding the function of the other toe flexor muscles, particularly the quantitative relationship between tendon excursion and toe flexion angles.
The focus of this study was to investigate anatomical variations of the toe flexor muscles and how those variations influence toe flexion angles due to tendon excursion using Thiel-embalmed cadavers.
Materials and methods
Specimens
Six intact human cadaveric lower extremities preserved using Thiel's embalming method were utilized. The Thiel's method of preservation can preserve the flexibility of the joints and soft tissue. 24 All the specimens were male donors, and the mean age of the specimens was 84.8 (range, 73–94) years. This study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and all subsequent revision. The protocol of the study was accepted by an ethics review board of our university. (Approval number 28-2-23).
Specimen preparation
Plantar skin, subcutaneous fat, and the plantar aponeurosis were removed exposing the FHL tendon, the FDL tendon, FDB, and the QP. Reference markers were carefully placed on each tendon in order to quantify tendon excursion. The skin and subcutaneous tissue along the length of the toe flexor tendons proximal to the ankle joint for approximately 5 cm was removed, and the FHL and FDL tendons were exposed. Kirschner wires were inserted in the distal phalanges of each toe to be used as reference to measure toe flexion. The ankle was fixed in the neutral position by Kirschner wires. The tibia was fixed on a wooden board with Steinman pins. The lower leg was positioned vertically in an inverted position with the knee flexed.
Measurement of toe flexion angle during simulated muscle contraction
A digital high resolution video camera was fixed at a distance of one metre perpendicular to a line connecting the second toe and the centre of the calcaneus. To simulate muscle contraction, the muscles were grasped with locking forceps and manually distracted for 5 and 10mm for the FDB, the quadratus plantae medial (QPM), and the quadratus plantae lateral (QPL). The tendons of the FHL and FDL were distracted for distances of 5, 10, and 15 mm (Figure 1). For each incremental tendon excursion, the toe flexion movement was simultaneously recorded by the camera. The FHL and FDL tendon were pulled at the proximal level of the ankle joint. The initial position of the toes prior to all tests were horizontal to the floor. 25
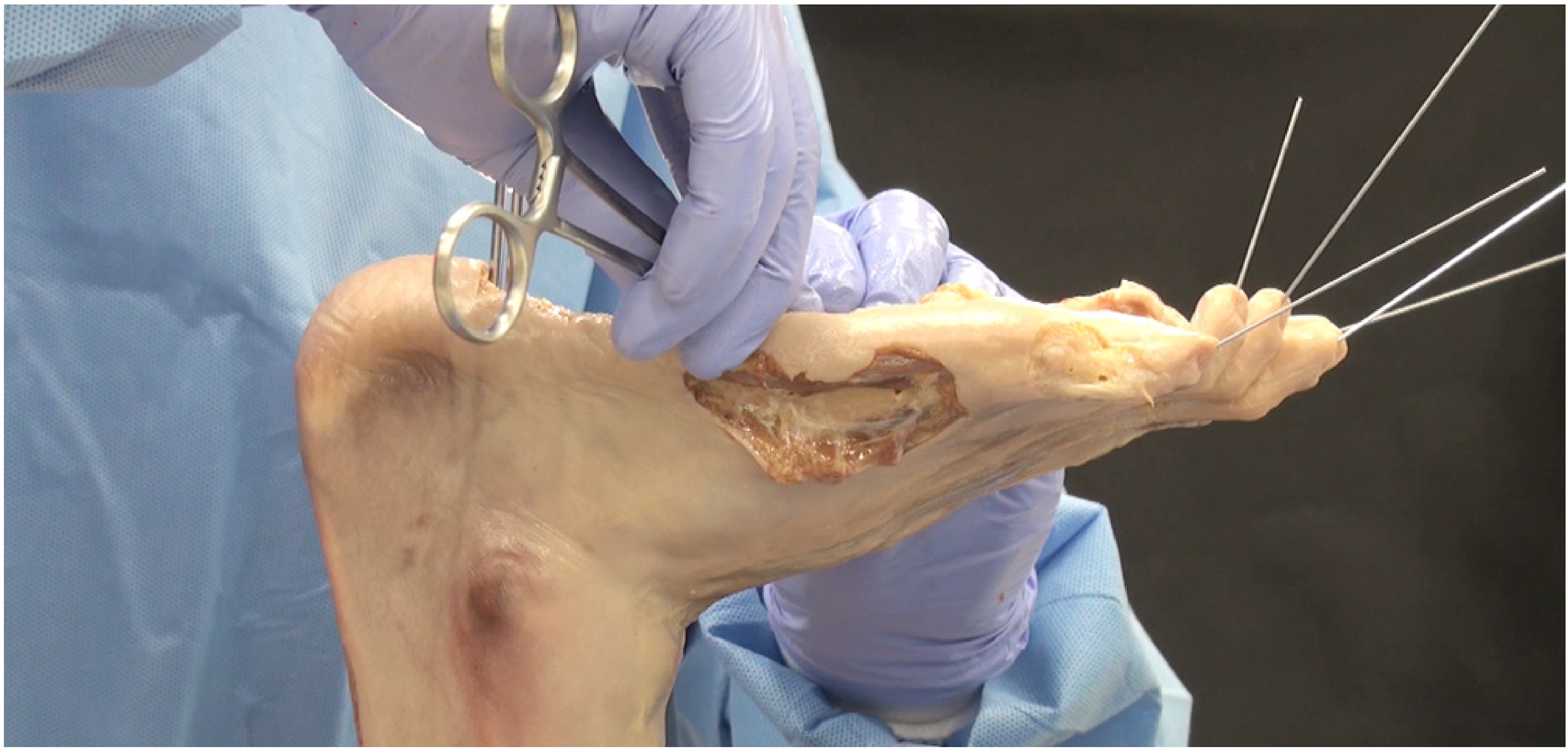
Measurement of toe flexion angle by simulated muscle contraction. The second to fifth toes flexed when the flexor digitorum brevis muscle was manually distracted 5mm with locking forceps.
Movie files were imported into a personal computer and images for each excursion level saved. A computerized data analysis software (Image J, U.S. National Institutes of Health, Bethesda, MD, USA) was used to evaluate the angles of the wires inserted in each toe. The flexion angle differences from the initial position were calculated at each excursion level. 25
Anatomical variation of the toe flexor muscles
The anatomical variations of the toe flexors were observed and recorded for each specimen after the experimental method. In accordance with the classification system, 17 we identified the anatomical variations of FHL and FDL's interconnections along with the tendinous slip pf the FHL. Type I is described as proximal to distal connection of the FHL to the FDL, Type II a proximal to distal connection of the FDL to the FHL, Type III a crossed connection, and Type IV as no connection between the tendons.
An additional subdivision was performed categorizing the connection to the lesser toes, based on an insertion in (type a) the second toe, (type b) the second and third, (type c) the second to fourth, and (type d) all lesser toes. 17
Insertion of the QPM and QPL to the long toe flexor tendon was identified. We also observed any existence and morphological characteristics of the FDB tendons to the lesser toes.
Statistical analysis
All statistical analyses were evaluated using IBM SPSS version 22.0. Two-way repeated measures analysis of variance was used to compare the changes of toe flexion angles between muscles and displacement of tendon excursion. The analysis performed for comparing the FHL and FDL. Bonferroni post hoc test was used when main significance was identified. Statistical significance was set at p < 0.05.
Results
Anatomical variation of the toe flexor muscles
Observations of the anatomical variation of the toe flexor muscles are recorded in Table 1. The tendinous slip of the FHL was observed in all specimens. No tendinous slip from the FDL (Type II) or connection type between FHL and FDL (Type III) were observed. All specimens were classified as Type I. Regarding the tendinous slip of the FHL, the FHL inserted to the second and third toes (type b) in five specimens, and inserted to the second, third, and fourth toes (type c) in one specimen.
Anatomical variation of the toe flexor muscles for each specimen.

The FDB inserted to the second to fifth toes in five specimens. In two specimens of this group fifth tendon was very thin and marginal. For the remaining specimen, the FDB inserted to the second to fourth toes.
The QPM was not evident in one specimen, and the QPL missing in another specimen. Most often the QPM and QPL inserted to the fourth tendon. The second and third toes were often attached by the QPM, and the third toe was often attached by the QPL. There was no QP insertion to the second toe in one specimen or to the fifth toe in three of the six specimens.
Toe flexion angle during simulated muscle contraction
Results of five type b specimens are recorded in Figure 2. We observed that for the second and third toes, changes in toe flexion angle were not significantly different between the FHL and FDL. However, there were significantly smaller angle changes in tendon excursion of the FHL vs. the FDL for the fourth and fifth toes. For the fourth toe, flexion angles increased distracting the FHL for 15 mm rather than the 5 and 10 mm levels. Results of a type c specimen (Specimen F) are shown in Figure 3. In the toes with the tendinous slip of the FHL (2nd, 3rd, 4th toes), changes in toe flexion angles were comparable for both the FHL and FDL.

The changes of toe flexion angles in individual toes in type b subjects (n = 5). *p < 0.05 vs. FDL, †p < 0.05 vs. 5 mm of FHL, ‡p < 0.05 vs. 10 mm of FHL.

The changes of toe flexion angles in individual toes in one type c subject.
The changes of toe flexion angles for 10mm tendon excursion of the FDB, QPM, and QPL are shown in Figure 4. The relationship of toe flexion for these muscles varied. For the 5th toe, reduced toe flexion motion was demonstrated by distracting the FDB in four specimens (Specimen C, D, E, F in Figure 4A). Those toes where the QPM inserted had increased flexion, and those toes without the QPM had relatively reduced flexion angles (2nd toe of Specimen E and 5th toe of Specimen F in Figure 4B). The QPL also flexes toes in which it is inserted except the second toe. The second toe was flexed by pulling the QPL regardless of insertion of the QPL. Reduced toe flexion angles were observed in the 5th toe which had no insertion of QPL (Specimen B, D, F in Figure 4C).

The changes of toe flexion angles with 10mm tendon excursion of the three muscles for each specimen. A. the flexor digitorum brevis, B. medial head of the quadratus plantae, C. lateral head of the quadratus plantae.
Discussion
This study investigated anatomical variation of the toe flexor muscles and how that may relate to toe flexion angles for associated tendon excursion. All subjects had the tendinous slip of the FHL. Subdivision of the slip was type b and type c. From previous publications, type b was the most common anatomical variation followed by type a. 20 As in the previous reports, type b was most common of our specimens, but type a was not present and there was one example of a type c anatomy. Distraction of the FHL resulted in toe flexion similar to that of the FDL in toes with a tendinous slip (Figure 2). The tendinous slip of the FHL is conjectured to have a role flexing the lesser toes with insertion of the FHL tendinous slip from an anatomical viewpoint.16,18 From our findings, when the tendinous slip of the FHL is attached to the second and the third toe (type b), the toe flexion relationship for FHL excursion was similar to FDL excursion. For the one type c specimen (Specimen F) there was increased flexion of the fourth toe which presented with the tendinous slip of the FHL. This study demonstrated that the tendinous slip of the FHL has a significant flexion function for the lesser toes with insertion of the slip. Those toes without the tendinous slip of the FHL demonstrated reduced toe flexion. The magnitude of toe flexion was relatively more at the 15mm excursion compared to both the 5mm and 10mm levels. This partial flexion of the toes without the tendinous slip of the FHL might occur due to connective tissue between the tendons.
We also investigated the relationship of simulated muscle contraction on lesser toe flexion for three foot intrinsic muscles; the FDB, QPM, and QPL. In general, the FDB is believed to attach on the middle phalanges of all the lesser toes. However, previous studies reported 37–45% feet had this classic anatomy.22,23 The variations were located in the lateral two toes, and no deviations were observed in the second and third toes. 22 The tendons of the FDB to the fourth and fifth toes were absent or thinned relative to the other toes.22,23 There were inconsistencies concerning the insertion of the QPM and QPL. In one anatomical study, 16 the QP had two heads in 80%, one medial head in 10%, one lateral head in 8%, and no heads in 2%. Of the long toe flexor tendons, the QP formed the second (97%), the third (98%), the fourth (99%) and the fifth tendon (51%). 20 We observed the intrinsic muscles to be similar to these findings. The tendon of FDB to the fifth toe was very thin or absent in three specimens. The QPM or QPL were absent in two specimens and the insertion to the second or the fifth long flexor tendon was not observed in four specimens.
During extension of the FDB, there was some flexion in the fifth toe for Specimen C, D, E, and F. Specimen E had no insertion of the FDB to the fifth toe. There was an insertion in Specimen F, however, the fifth tendon was thin and minimal. When the QPM was extended, Specimen E and F resulted in a very small degree of flexion in the second toe and the fifth toe, respectively. These two specimens had no insertion of the QPM to the second toe (Specimen E) and the fifth toe (Specimen F). Moreover, when the QPL was extended, Specimen B, D and F resulted in a small degree of flexion of the fifth toe. All these three specimens had no insertion of the QPL to the fifth toe. These findings revealed that anatomical variation of the foot flexor intrinsic muscles significantly influenced function of the lesser toes.
For two specimens, two muscles resulted in very minimal toe flexion. Specimen E for the fifth toe regarding the FDB and the second toe regarding the QPM. This specimen did not have an FDB insertion in the fifth toe or a QPM insertion in the second toe. It was also missing the QPL. For an individual that presents with a similar anatomy, they may have more difficulty improving toe flexion function through muscle training. Specimen F demonstrated very minimal flexion in the fifth toe during FDB, QPM, and QPL extension. In such a foot, flexion of the fifth toe may depend on the FDL and the flexor digiti minimi brevis muscle.
Data generated from this study could be useful when considering toe function following tendon transfer surgeries or muscle/tendon trauma about the lower leg. The FDL is often used for tendon transfer surgeries for foot disorders such as flatfeet. The loss of FDL after such surgery could be compensated by the tendinous slip of the FHL. However, the lesser toes without the FHL tendinous slip would lose function by FDL. Our data demonstrated that the magnitudes of toe flexion due to extension of the FDB, QPM, or QPL were similar to the FDL up to 10mm excursion. These intrinsic muscles may compensate flexion function of the lesser toes even if no FHL tendinous slip is present. Whereas, the number of FHL tendinous slip can be assessed clinically by the FHL branch test 25 if FHL tendinous slip is present. This study demonstrated that the tendinous slip of the FHL has a significant flexion function for the toes with FHL slips. Therefore, considering the anatomical variation of the toe flexor muscles could be useful for evaluating toe flexor function and applying exercise therapy.
There are limitations to this study. The sample size is small, and as a consequence, toe flexion motion specimens of a ‘type a’ anatomy could not be studied. We were able however to demonstrate the tendinous slip of the FHL had a significant role regarding lesser toe flexion. For this type anatomy we estimate the second toe is flexed by action of the FHL. Another limitation is the method of inserting wires in the distal phalanges of each toe to measure toe flexion. The flexion associated with the metatarsophalangeal joint and/or interphalangeal joint were not recorded.
In summary, this study determined the relationship between anatomical variation of the toe flexor muscles as they relate to toe flexion function. Toe flexion was similar for simulated muscle action of the FHL as to that of the FDL for those toes with the tendinous slip of FHL. Toe flexion resulting from the FDB, QPM, and QPL were not significantly different from the FDL up to 10mm of excursion. However, the numerous anatomic variations complicates the specific function of each muscle to individual toe function. Anatomical variation of the toe flexor muscles should be taken into account when evaluating toe function and applying exercise therapy for foot disorders.
Footnotes
Acknowledgements
The authors would like to thank all donors and their families for donating cadavers to our institution.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.