
Abstract
Background:
Endoscopic plantar fascia release (EPFR) is a common surgical option for recalcitrant plantar fasciitis. Although calcaneal spur excision (CSE) is frequently performed as an adjunct, its added clinical benefit remains unclear. This study compared outcomes of EPFR alone vs EPFR combined with CSE.
Methods:
This retrospective study included 23 patients (30 feet) who underwent endoscopic surgery for plantar fasciitis between 2017 and 2024. Patients were divided into 2 groups according to surgical procedure performed: EPFR (n = 22 feet) and EPFR+CSE (n = 8 feet). Pain and functional outcomes were assessed pre- and postoperatively using the visual analog scale (VAS), first-step VAS, American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot score, and Foot Function Index (FFI).
Results:
Both procedures were associated with significant postoperative improvement in pain and function (all P < .001). Mean VAS scores improved from 6.2 to 1.5 in the EPFR group and from 6.4 to 1.2 in the EPFR+CSE group. AOFAS scores increased from 66.4 to 95.3 and from 64.5 to 94.5, respectively. Postoperative FFI values decreased from approximately 107 to 30 in both groups. However, comparison between groups revealed no statistically significant differences for any parameter (VAS p = 0.24; AOFAS p = 0.23; FFI p = 0.61). No recurrence or complications were observed.
Conclusion:
EPFR, with or without CSE, was associated with clinical and functional improvement. With the numbers available, no additional benefit of CSE could be detected.
Level of Evidence:
Level III, retrospective comparative study.

Introduction
Plantar fasciitis is considered a chronic degenerative enthesopathy, one of the most common causes of heel pain that was first proposed by Wood in the early 19th century as a major cause of plantar heel pain. 1 It affects approximately 10% of the population and commonly observed in long-distance runners. Clinically, patients typically report heel pain with the first steps in the morning or after prolonged standing and significantly negatively impacts patients’ quality of life.2-4 The disease is characterized by collagen degeneration, microtears, and inflammatory responses resulting from repetitive microtrauma at the insertion site of the plantar fascia into the calcaneus. This suggests failed healing responses and chronic inflammation. Therefore, persistent, chronic, and repetitive overloading of the plantar fascia is a key factor in the occurrence of plantar fasciitis.5,6
The calcaneal spur is a frequently discussed structure in the pathogenesis of plantar fasciitis. Although detected in approximately 15% of the population, it does not always cause symptoms. However, the length of the spur, its relationship with the plantar fascia, and its pressure on the inferior calcaneal nerve may be one of the causes of plantar heel pain.2,7,8 Nonetheless conservative treatments, including rest, immobilization, stretching exercises, orthotics, nonsteroidal anti-inflammatory drugs, injections, extracorporeal shock wave therapy, dry needling, and laser therapy, respond in 85% to 90% of cases, the pain becomes persistent and chronic in a group of patients. In this case, surgical treatment is considered.
The main goal of surgical treatment is to reduce traction stress on the plantar fascia and relieve loading on the calcaneal enthesis. Surgical approaches include percutaneous, open, or endoscopic plantar fascia release (EPFR). Additionally, excision of the calcaneal spur, which is thought to cause chronic tension on the plantar fascia and irritation of the enthesis, calcaneal decompression, and inferior calcaneal (Baxter) nerve neurolysis are included.
In recent years, fluoroscopy- and endoscopy-assisted minimally invasive techniques have gained importance because of their low complication rates and rapid weightbearing. 7 However, there is no definitive consensus on which surgical procedure is superior. In the literature, although studies suggest that calcaneal spur excision (CSE) alone may be sufficient to relieve symptoms, there are also studies suggesting that EPFR in addition to spur excision provides faster functional recovery.2,3
The aim of this study was to compare the clinical and functional outcomes of EPFR alone with CSE in addition to EPFR in patients with plantar fasciitis resistant to conservative treatment. We hypothesized that additional CSE would not yield superior pain or functional outcomes compared with EPFR alone.
Patients and Methods
This was a retrospective nonrandomized study of patients who were diagnosed with plantar fasciitis and resistant to conservative treatment for more than 1-year follow-up from January 2017 to December 2024. Our institutional review board (Acibadem University ATADEK No: 2025-11/424) approved the study protocol. Data regarding patient age, sex, body mass index (BMI), diagnosis, date of surgery, and surgery procedure performed were collected. All medical records were obtained from hospital computer databases.
Inclusion criteria were patients who had heel pain with diagnosis of plantar fasciitis with no response to conservative treatment more than 1 year, radiographic images revealing a calcaneal spur, and magnetic resonance imaging (MRI) of the foot showing thickening of the fascia. Exclusion criteria were a history of heel trauma or calcaneal fracture, secondary heel pain including systemic inflammatory conditions, metabolic bone disease, or referred pain, based on clinical history and examination. Patients with normal radiologic examination results were excluded to avoid inclusion of nonspecific plantar heel pain and to ensure a homogeneous study population with radiographic findings consistent with chronic plantar fasciitis.
Radiologic examinations included standard preoperative nonweightbearing lateral foot radiography and foot MRI in all patients. Radiographs were used to confirm the presence of calcaneal spur and to exclude alternative osseous pathology. The indication for CSE was determined according to spur size measured on nonweightbearing lateral foot radiographs. CSE was added when spur length exceeded 5 mm, whereas patients with smaller spurs underwent EPFR alone. MRI was used to support the diagnosis of chronic plantar fasciitis by demonstrating plantar fascia thickening. 9
Patients were divided into 2 groups based on the surgical intervention performed: (1) EPFR only and (2) combined EPFR+CSE. Preoperative and postoperative outcomes were assessed using the visual analog scale (VAS) and first step VAS for pain, the American Orthopaedic Foot & Ankle Society (AOFAS) ankle-heel score, and the Foot Function Index (FFI) for function. All patients were followed for a minimum of 1 year.
Surgical Technique
All patients had been treated by the same highly experienced surgeon (B.K.) using a standardized endoscopic technique. The patient was placed supine on the operating table and general anesthesia was administered. A supportive pad was placed under the ipsilateral hip and a pneumatic tourniquet cuff was wrapped around the thigh, followed by skin disinfection. The surgical drape was then completed in a sterile manner. Three portals were utilized: one medial, one lateral, and one plantar portal at a nonweightbearing area. The endoscopic obturator (EndoBlade Soft Tissue Release System, Arthrex Inc) was advanced bluntly from medial to lateral between the plantar fascia and plantar fat tissue. The obturator cannula was advanced up to the lateral subcutaneous tissue, and the position of the lateral portal was determined from the skin bulge. A lateral portal was opened, and a crescent-shaped clear cannula was placed over the obturator from lateral to medial. The endoscope device was advanced through the cannula from the lateral portal, and the plantar fascia was visualized. Then, the plantar fascia was released endoscopically from lateral to medial with a triangular knife. The release was intentionally limited to approximately 30% to 50% of the medial portion of the plantar fascia to avoid over-release. 10 Following the release of the plantar fascia, a working area was created from the plantar portal using a shaver and a radiofrequency device between the plantar fascia and the flexor digiti minimi to expose the calcaneal spur. After confirming under fluoroscopy that the instruments were in contact with the calcaneal spur, the calcaneal spur was removed with a burr device (Figure 1). Complete excision of the calcaneal spur was reconfirmed using fluoroscopy. After the portals were closed with primary suture, dressing was applied. An elastic bandage was applied to the affected foot and elevated to reduce swelling.

Preoperative radiologic imaging and endoscopic findings in a patient with chronic plantar fasciitis. (A) Preoperative lateral radiograph of the left foot showing calcaneal spur. (B) Sagittal T2-weighted MRI showing increased signal and thickening at the plantar fascia. (C, D) Endoscopic visualization of calcaneal spur and after resection of calcaneal spur with an arthroscopic burr. (E, F) Plantar fascia release from lateral to medial with a triangular knife.
Postoperative Care
All patients followed a standardized postoperative rehabilitation protocol, including early mobilization and progressive weightbearing. A wound dressing, elastic bandage, elevation, and ice compresses were applied after surgery. On the first postoperative day, patients were asked to wear medical short boots and walk with crutches. Patients were gradually instructed to wear normal, full-weightbearing shoes 4-6 weeks postoperatively. Postoperative outcomes were assessed using VAS and first step VAS for pain, AOFAS, and FFI for function. Clinical outcome measures and nonweightbearing lateral foot radiographs were assessed at a standardized 1-year postoperative follow-up visit in all patients. For longer-term follow-up beyond 1 year, patients who were unable to attend in-person visits were contacted by telephone, and outcome measures were obtained through structured interviews. Postoperative complications were actively monitored during routine follow-up visits. Clinical assessment focused on potential complications reported in the literature including medial longitudinal arch collapse, persistent heel pain, sensory disturbances suggestive of Baxter nerve irritation or injury, wound problems, infection, and recurrent heel pain. Arch integrity was assessed clinically by inspection and physical examination, and nerve injury was evaluated based on sensory examination and patient-reported symptoms.
Statistical Analysis
Normality of the data distribution was assessed using the Shapiro-Wilk test. Depending on the distribution characteristics, either the independent samples t test or the Wilcoxon rank-sum test was applied to compare values between groups. For within-group comparisons between preoperative and postoperative measurements, the paired Wilcoxon signed-rank test was performed. For independent and paired t tests, Wilcoxon rank-sum and Wilcoxon signed-rank tests, mean differences and their 95% CIs were reported. Results are presented as mean ± SD, and a P value <.05 was considered statistically significant. Given the retrospective study design, no a priori sample size or power calculation was performed, and the study population represents a convenience sample of all eligible patients treated during the study period.
Results
A total of 23 patients (10 females and 13 males) were included in this study. In patients with bilateral involvement, each operated foot was considered an independent case, resulting in a total of 30 feet analyzed from 23 patients (16 right and 14 left side). Of these, 22 feet underwent EPFR only, whereas 8 feet underwent EPFR combined with CSE (EPFR+CSE) with no complications peri- or postoperatively (Figure 2).
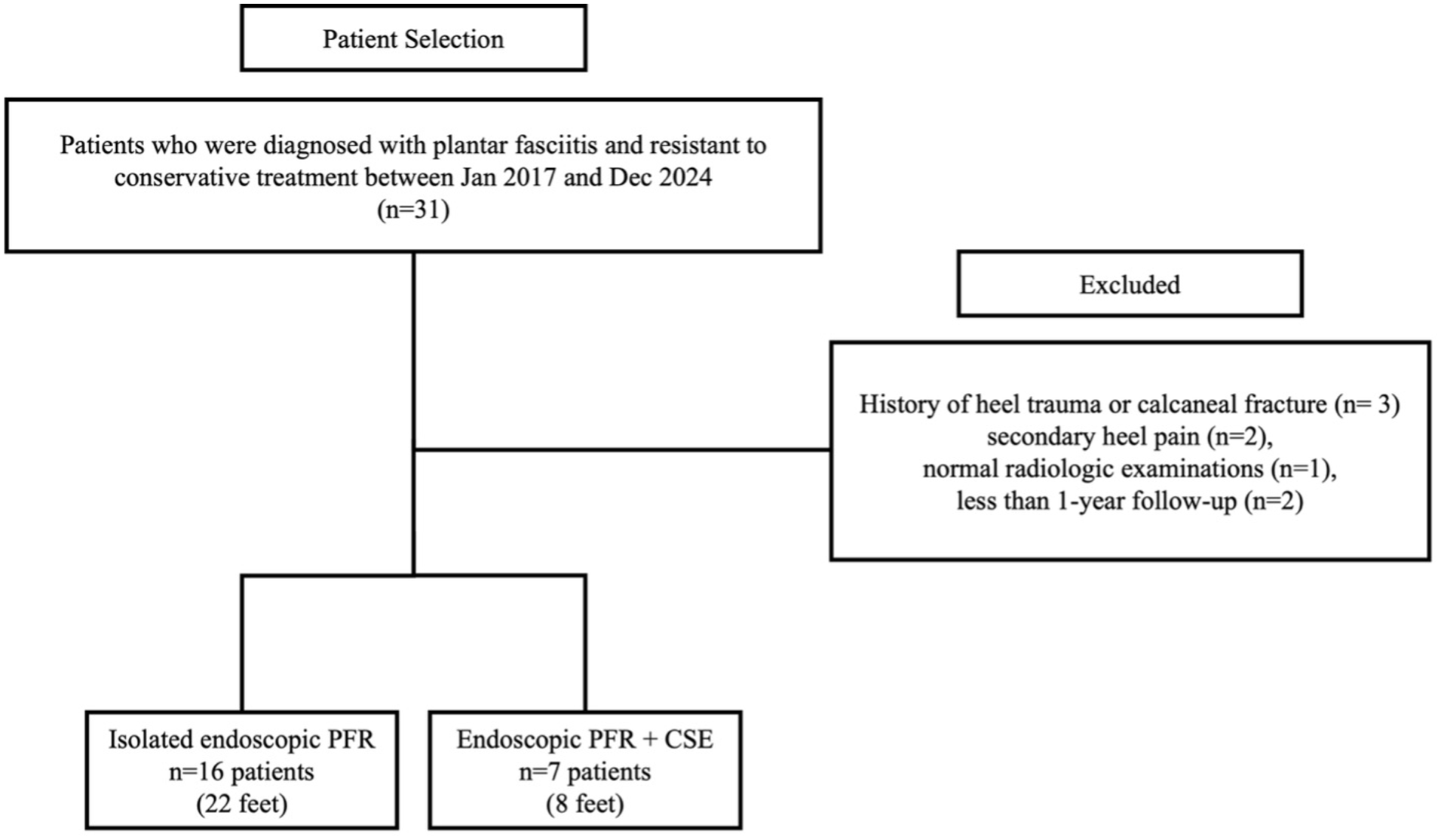
Flow diagram of patients included in the study. CSE, calcaneal spur excision; EPFR, endoscopic plantar fascia release.
The mean follow-up duration was 76.2 months. The groups were comparable in terms of baseline characteristics. Baseline characteristics, including gender distribution, age, BMI, and laterality of the operated side, were similar between the EPFR and EPFR+CSE groups (all P > .05; Table 1). Preoperative pain and functional outcome scores were also similar between groups, with no statistically significant differences observed (Table 2). No recurrence was detected in either group during the follow-up period.
Study Population Demographics and Characteristics.

Abbreviations: BMI, body mass index; CSE, calcaneal spur excision; EPFR, endoscopic plantar fascia release.
Preoperative Patient-Reported Outcomes.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; CSE, calcaneal spur excision; EPFR, endoscopic plantar fascia release; FFI, foot function index; PRO, patient-reported outcome; VAS, visual analog scale.
Both procedures resulted in significant postoperative improvements in pain and functional outcomes (P < .01 for all within-group comparisons). In both the EPFR and EPFR+CSE groups, significant improvements were observed in VAS pain, first-step VAS, AOFAS, and FFI scores. Detailed preoperative and postoperative values, along with mean differences and 95% CIs, are presented in Table 3.
Preoperative and Postoperative Patient Reported Outcomes.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; CSE, calcaneal spur excision; EPFR, endoscopic plantar fascia release; FFI, foot function index; PRO, patient-reported outcome; VAS, visual analog scale.
When postoperative outcomes were compared between groups, no statistically significant differences were observed in VAS pain, first-step VAS, AOFAS, or FFI scores between the EPFR and EPFR+CSE groups (Table 4). Although preoperative AOFAS scores were slightly lower in the EPFR+CSE group, this did not lead to superior postoperative outcomes.
Postoperative Patient-Reported Outcomes.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; CSE, calcaneal spur excision; EPFR, endoscopic plantar fascia release; FFI, foot function index; PRO, patient-reported outcome; VAS, visual analog scale.
Although no validated minimal clinically important difference (MCID) thresholds have been specifically established for postoperative VAS, or first-step VAS, AOFAS and FFI following surgical treatment of plantar fasciitis, previously reported MCID values for plantar heel pain provide a useful reference for clinical interpretation. Improvements observed in this study exceeded commonly reported MCID thresholds for VAS pain, first-step VAS, and the Foot Function Index, indicating substantial clinical benefit.11-15 No significant differences were identified between the EPFR alone and the additional CSE groups.
Discussion
This study demonstrates that EPFR with and without CSE are both associated with improved pain and functional outcomes, with no significant difference detected between the 2 approaches in this cohort. These findings suggest that EPFR alone provides clinical and functional benefits equivalent to the combined procedure, which suggests routine spur excision may be unnecessary in most cases.
The first step in treating plantar fasciitis is conservative treatment, which consists of physical therapy methods to reduce tension in the plantar fascia, plantar orthoses, and anti-inflammatory treatments. Eighty-five percent to 90% of patients respond to conservative treatments. Surgery is indicated for patients who do not respond to conservative treatment within 12 months. Surgical treatment options for plantar fasciitis include percutaneous, open, or EPFR; neurolysis or denervation; calcaneal osteotomy; spur excision; or drilling. These techniques can be applied alone, but combination treatment options are also available. There is no consensus on which method is superior.
To date, no validated MCID thresholds have been specifically established for postoperative outcomes following surgical treatment of plantar fasciitis. However, multiple studies have reported MCID values for commonly used outcome measures in patients with plantar heel pain, providing a meaningful framework for clinical interpretation. Prior literature suggests MCID values of approximately 8 to 13 mm for VAS pain, 18 to 19 mm for first-step VAS, and 6 to 12 points for the Foot Function Index.11-15 When these reference thresholds are applied, the magnitude of improvement observed in the present study (approximately 40-60 mm for VAS pain, marked reductions in first-step pain, nearly 30-point increases in AOFAS scores, and greater than 70-point improvements in FFI) clearly exceeds established MCID values, indicating clinically meaningful benefit following surgery. Importantly, despite these pronounced improvements, no statistically significant differences were detected between patients treated with EPFR alone and those undergoing EPFR with additional CSE, suggesting that routine spur excision does not confer additional clinical or functional advantage. These findings question the necessity of routine CSE during surgical management of plantar fasciitis, suggesting that the degenerative pathology of the fascia itself, rather than mechanical irritation from the spur, is the primary pain generator.
Nakajima reported favorable outcomes following fluoroscopic and endoscopic CSE without plantar fascia release in patients with recalcitrant plantar fasciitis and a calcaneal spur ≥2 mm, suggesting that isolated spur removal may be sufficient in selected cases. Although these findings may appear to contradict the present results, the 2 studies address different clinical questions. Whereas Nakajima evaluated the effectiveness of CSE as a standalone procedure in a noncomparative case series, the present study specifically investigated whether adding CSE provides additional benefit when EPFR is already performed. In this context, our findings do not refute the potential role of isolated CSE but rather indicate that routine spur excision does not confer incremental clinical or functional advantage as an adjunct to EPFR. 7
Cottom and Maker 16 described a minimally invasive endoscopic technique focusing on debridement of degenerative fascial tissue while preserving fascial continuity, emphasizing that symptom relief can be achieved without extensive release or aggressive spur excision. This concept aligns with the present findings, supporting the notion that the plantar fascia itself constitutes the primary pain generator, whereas the calcaneal spur may represent a secondary or incidental finding.
On the other hand, minimally invasive techniques have gained popularity. Because they reduce soft tissue trauma, allow earlier weightbearing, and yield outcomes comparable to open procedures. These methods have been reported to provide significant improvements in functional scores in patients who have not benefited from conservative treatment. In the literature, there are reported satisfactory outcomes with EPFR, with reduced postoperative morbidity and faster return to activity compared with open approaches. 17 Saxena 18 reported excellent to good outcomes following uniportal endoscopic plantar fasciotomy with release of approximately 50% of the medial band, particularly highlighting low rates of lateral column symptoms and rapid return to activity. These findings support the surgical philosophy adopted in the present study, where partial medial release was intentionally performed to preserve arch stability while achieving effective symptom relief. Although some studies proposed that removing the calcaneal spur may enhance symptom relief, our results indicate that spur excision provides no measurable clinical advantage when the plantar fascia is adequately released. 2 EPFR alone also offers practical surgical advantages like smaller incisions, a lower risk of nerve injury, and shorter operative time. By avoiding unnecessary spur excision, surgeons can further reduce perioperative trauma and facilitate rehabilitation.
One of the major strengths of this study is the long follow-up period, with a mean of 76.2 months (approximately 6.3 years). This allowed for reliable assessment of long-term outcomes in terms of pain, functional recovery, and recurrence. The number of studies reporting such long-term follow-up in the literature is quite limited.
There were also limitations. The main limitations of this study are its retrospective design, small sample size, and potential selection bias. Because the sample was limited to 30 feet and only 8 nonrandomized participants underwent the combined procedure, the study may be underpowered to detect smaller but clinically relevant differences between groups. Radiographic assessment of arch height or longitudinal foot alignment was not performed, as standing weightbearing radiographs were not routinely obtained and these parameters were outside the scope of the present study. Furthermore, postoperative MRI or ultrasonographic evaluation of fascial integrity was not performed. Outcome assessment relied on patient-reported outcome measures, which are inherently subjective, although these instruments are widely accepted and validated in plantar heel pain research. MCID thresholds applied in this study were derived from plantar heel pain populations rather than exclusively surgical cohorts, which may limit direct generalizability. Nevertheless, the study provides valuable preliminary data from a homogeneous cohort with standardized surgical and rehabilitation protocols. Future prospective, multicenter studies with larger cohorts are warranted to confirm these findings and explore whether specific spur morphologies or nerve involvement modify clinical outcomes.
Conclusion
In conclusion, endoscopic plantar fascia release was associated with significant symptom relief. No added benefit was detected with the concomitant excision of calcaneal spurs in this series.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261427476 – Supplemental material for Comparison of Endoscopic Plantar Fascia Release With and Without Calcaneal Spur Excision for Recalcitrant Plantar Fasciitis
Supplemental material, sj-pdf-1-fao-10.1177_24730114261427476 for Comparison of Endoscopic Plantar Fascia Release With and Without Calcaneal Spur Excision for Recalcitrant Plantar Fasciitis by Edip Yilmaz, Muge Kirac, Tahir Koray Yozgatli, Berhan Bayram, Tekin Kerem Ulku and Baris Kocaoglu in Foot & Ankle Orthopaedics
Footnotes
Author Note
The investigation was performed at Acibadem Altunizade Hospital, Department of Orthopedics and Traumatology, Istanbul, Turkey.
Ethical Considerations
Ethical Committee approval for this study was obtained from Research Ethics Commission of Acibadem University (No. 2025-11/424).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.