
Abstract
Background:
To determine whether a combined endoscopic suprafascial and infrafascial approach with medial and lateral portals is a safe and effective technique for the endoscopic treatment of chronic plantar fasciitis with plantar heel spur pain.
Methods:
An interventional, prospective study was conducted. A total of 61 patients with plantar fasciitis with plantar heel spur pain underwent an endoscopic plantar fasciotomy with plantar heel spur resection, using a combined suprafascial and infrafascial approach between January 2018 and August 2022. Preoperative Foot and Ankle Ability Measure (FAAM), 36-Item Short Form Health Survey (SF-36), and visual analog scale (VAS) scores were measured. The measurements were repeated at 6 weeks, 3, 6, and 12 months postoperatively and at the final follow up. Preoperative and 1-year postoperative film parameters (Meary angle, calcaneal pitch angle, medial cuneiform–fifth metatarsal height) were compared.
Complications were recorded at each encounter.
Results:
The mean follow up time was 2.6 ± 1.1 years. At the 6-week postoperative visit, the mean change in FAAM-ADL, FAAM-Sport, SF-36 physical component summary, SF-36 mental component summary, and VAS were 26.0,19.0, 44.8, 61.2, and −5.8, respectively. These changes were statistically significant (P < .001). These findings were sustained and generally improved at all other follow-up points: 3, 6, and 12 months postoperatively and final follow-up. The average period until the recovery of activities of daily living and sport activities were 2.6 and 8.6 weeks, respectively. There were no significant differences between the pre- and 1-year postoperative radiographic values (P > .05). No cases resulted in medial arch collapse. Five cases (8%) had an injury to the first branch of lateral plantar nerve.
Conclusion:
Endoscopic plantar fascia release and plantar heel spur resection using a combined suprafascial and infrafascial approach resulted in the improvement of postoperative FAAM, SF-36, and VAS scores and involved a low incidence of postoperative complications.
This is a visual representation of the abstract.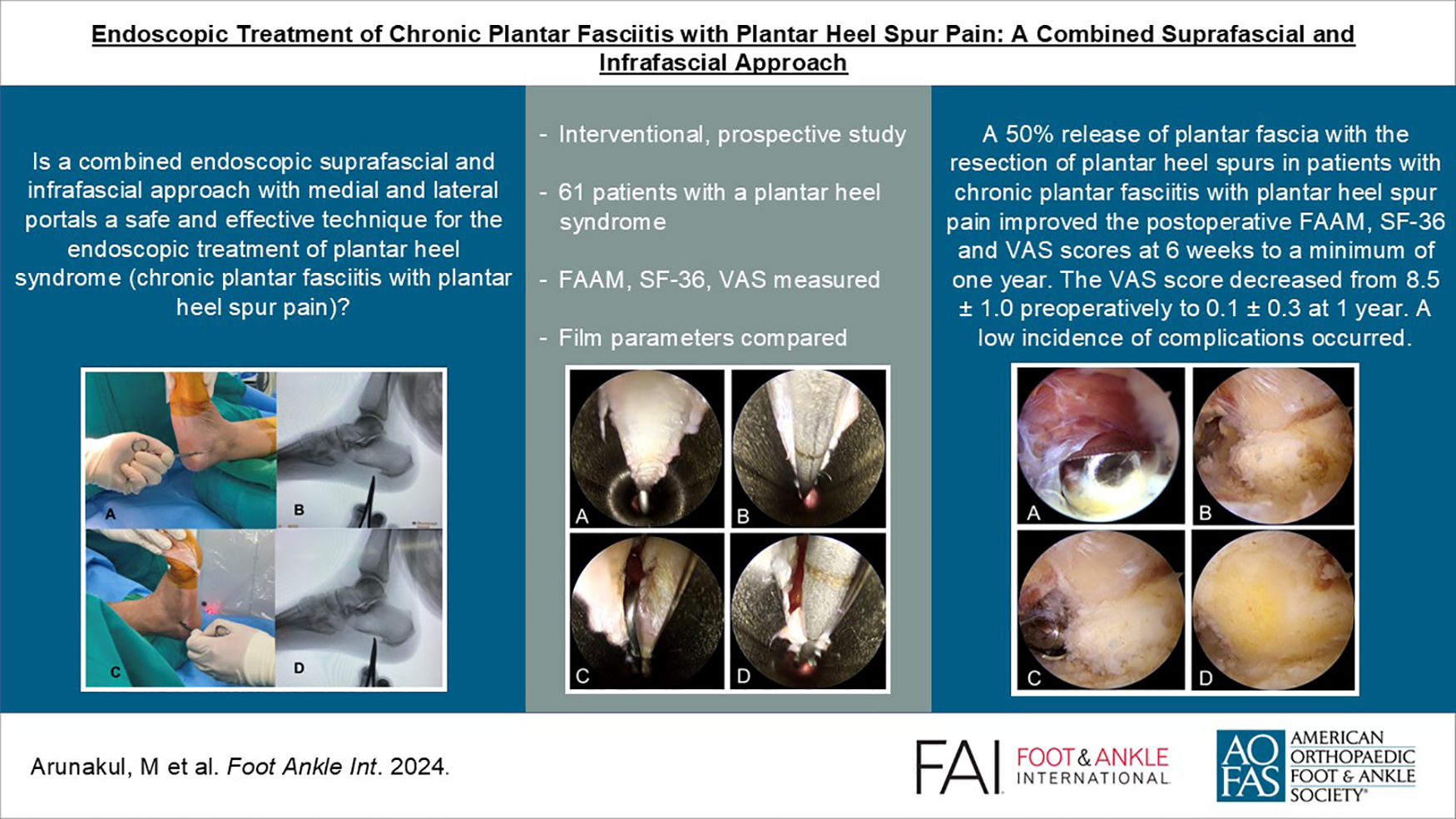
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.