
Abstract
Background:
Surgical management of failed ankle fusion is challenging. The objective of this study is to present the clinical and radiographic results of tibiotalar fusion takedown via a lateral approach with conversion to transfibular, trabecular metal (TM) total ankle arthroplasty (TAA).
Methods:
Sixteen patients underwent an ankle fusion takedown with conversion to transfibular TAA: 9 patients had prior tibiotalar fusions, and 7 had tibiotalocalcaneal fusion. Patient demographics, complication profiles, and radiographic parameters were collected. Pre- and postoperative patient-reported outcome measures (PROMs) were analyzed with 12-Item Short Form Health Survey (SF-12), visual analog scale (VAS), and the Ankle Osteoarthritis Scale (AOS). Radiographic outcomes included coronal and sagittal alignment, tibiotalar plantarflexion (PF) and dorsiflexion (DF) range of motion, and incidence of periprosthetic radiolucency and/or implant subsidence.
Results
Average age was 56.8 (range, 25-75) years with 4.7 (2-11) years’ follow-up. There was significant improvement in VAS, AOS pain and disability, and SF-12 physical and mental component summary scores (all P < .05). There was 1 (6.3%) case of implant revision for periprosthetic fracture about the tibial component. There were 8 (50%) reoperations at an average of 20.9 ± 10.8 months following fusion takedown, 4 (25%) cases of fibular hardware removal, and 4 (25%) cases of medial gutter debridement. Average radiographic DF and PF postoperatively was 12.5 ± 5.6 degrees and 13.5 ± 9.1 degrees. There was no presence of periprosthetic cysts at final follow-up.
Conclusion:
Ankle fusion takedown with conversion to a TM ankle through a transfibular approach yielded significant improvement in PROMs and radiographic ROM, with a modest complication rate at average 4.7 years’ follow-up. Although technically challenging, transfibular TAA following ankle fusion takedown is a reasonable treatment option for symptomatic tibiotalar or pantalar fusion.
Level of Evidence:
Level IV, case series.
Introduction
Ankle fusion is a conventional procedure. It is effective at relieving pain but comes with the drawback of reduced ankle range of motion. Because of mitigation of joint contact pressure, adjacent joint degeneration is common after ankle fusion.1,2 Other complications include nonunion rates as high as 18%. 3 The majority of ankle fusions with a delayed union (71%) are likely to fail in 5 years. 4 Usual treatment options for failed ankle fusion include revision fusion and extension of fusion to adjacent joints, but 20% may still not heal and amputation may be needed for refractory cases. 5 Additionally, there are patients who may undergo an initial successful fusion who may not be satisfied with functional outcomes. Therefore, there has been growing interest in the efficacy of ankle fusion takedown (TD) and conversion to total ankle arthroplasty (TAA). In addition to pain relief, TAA is an attractive option compared with arthrodesis as it allows for better preservation of tibiotalar range of motion (ROM) with improved gait. Although TAA after primary fusion has historically been approached with caution because of concerns about implant stability, functionality, and long-term outcomes, recent studies have shown promising results.6 -10
Traditional anterior approach has been the standard for ankle replacement but has the risk of neurovascular compromise and wound healing issues. In complex individuals with previous fusions or traumatic injury, anterior skin compromise may preclude an anterior approach to treat failed ankle fusion. Transfibular TAA is believed to enhance visualization and facilitate soft tissue handling in complex cases given its unique approach. Although results are promising for takedown fusions using an anterior-based ankle system, there is a scarcity of literature looking at takedown fusions using a transfibular total ankle system.
The primary aim of this study was to assess implant survivorship and clinical and radiographic outcomes in patients who underwent conversion of prior ankle arthrodesis to transfibular TAA. We hypothesized that patients would have significant overall improvement in patient-reported outcomes and radiographic findings postoperatively.
Methods
Study Design and Patient Selection
This retrospective study was conducted using the senior author’s (L.C.S.) total ankle replacement database, a single-surgeon and co-designer series. Inclusion criteria consisted of patients 18 years or older undergoing conversion of ankle fusion to transfibular TAA using the Zimmer Trabecular Metal (Zimmer Biomet) prosthesis between 2013 and 2022. Indications for conversion to TAA included relief of pain and stiffness, with the goal of improving ankle range of motion and offloading stress on the adjacent, unfused hindfoot and/or midfoot joints. Institutional review board approval was obtained prior to data collection. This study was designed and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement on strengthening the reporting of observational studies. 11
Retrospective chart review of the electronic medical record identified patient demographics, comorbidities, perioperative data, and radiographic information (Table 1). Demographic variables included age at the time of the index procedure, sex, and body mass index. Comorbidity data collected included the American Society of Anesthesiologists (ASA) score, history of tobacco use, diabetes, and/or malignancy. Perioperative data encompassed the length of follow-up, laterality, underlying etiology of ankle arthritis (classified as posttraumatic, primary osteoarthritis, or inflammatory arthritis), and history of prior ankle and/or hindfoot surgeries.
Patient Demographics and Surgical History (N = 16). a

Abbreviations: ASA, American Society of Anesthesiologists; BMI, body mass index.
Values are reported as mean (range) or n (%).
The length of follow-up was defined as time from surgery to the latest postoperative visit where patient-reported outcome measures (PROMs) and weightbearing ankle radiographs were collected. Adverse events and reoperations were reported using the Canadian Orthopaedic Foot and Ankle Society (COFAS) Reoperation Coding System (CROCS). 12 Reoperation was defined as surgery performed on the ipsilateral ankle after the index surgery that did not require removal of the metal components. Revision was defined as removal of one or both of the metal components, conversion to arthrodesis, or amputation.
Patient-Reported Outcomes
PROMs included the 12-item Short Form Health Survey (SF-12) physical (PCS) and mental component summary (MCS) scores, Ankle Osteoarthritis Scale (AOS), and visual analog scale (VAS) for pain. All PROMs included are validated measures that have been applied to numerous foot and ankle pathologies.13 -15 The SF-12 and AOS are scored ranging from 0 to 100. VAS is scored from 0 to 10. A higher score indicates impairment for VAS and AOS, whereas a lower score indicates impairment for SF-12.
Radiographic Outcomes
Radiographic assessment included weightbearing anteroposterior (AP), mortise, and lateral view radiographs of the ankle obtained at latest follow-up. All radiographs were analyzed by a foot and ankle fellowship-trained fellow and an orthopaedic surgery resident, with final review by the senior author.
Postoperative tibiotalar plantarflexion and dorsiflexion range of motion (PF, DF) were measured by tibiopedal excursion on standing flexion-extension radiographs.16,17 The AP radiograph was used to measure the tibial coronal alignment angle (alpha angle [α]), whereas the lateral radiograph was used to measure the tibial sagittal alignment angle (beta angle [β]) and talar sagittal alignment angle (gamma angle [γ]).18 -21 Tibial and talar periprosthetic radiolucency was assessed on lateral weightbearing radiographs with the 12-zone classification scheme described by Barg et al. 18 The zones were categorized as normal, lucency (<2-mm radiolucent line), cyst (>2mm radiolucency), or not accessible (ie, superimposed fibular hardware).
Surgical Technique
Patients were positioned supine with the operative extremity elevated. When possible, removal of prior ankle fusion hardware was performed through the same lateral transfibular approach. In patients with an anterior plate and screw construct, additional anterior exposure was performed through the previous surgical incision.
TAA was performed in all patients using the Zimmer Trabecular Metal Total Ankle through a transfibular approach based on the manufacturer’s technique guide (Figure 1). 22 Fibular osteotomy was performed to provide exposure of the ankle joint. Once final components were implanted, the fibular osteotomy was reduced and fixed with a precontoured locking plate. Autogenous bone graft from the tibia or ipsilateral iliac crest was applied to the osteotomy site to promote healing. Additional procedures were concomitantly performed as needed to achieve appropriate alignment and stability (Table 2).

Weightbearing plain films of a 69-year-old man who underwent fusion takedown to transfibular total ankle arthroplasty (TAA). Anteroposterior (AP) and lateral radiographs demonstrate his initial presentation with painful subtalar arthritis in the setting of previous tibiotalar arthrodesis (A and B). He underwent fusion takedown with conversion to transfibular TAA and subtalar fusion (C and D).
Concomitant Procedures (N = 16).
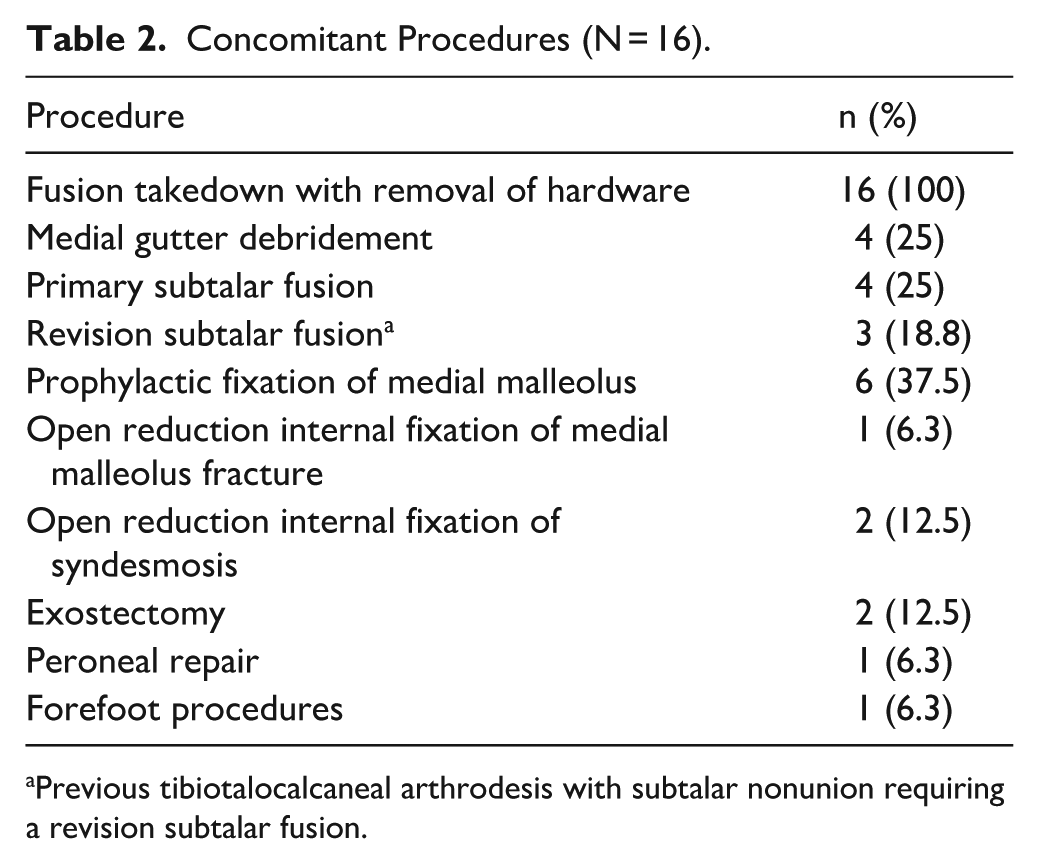
Previous tibiotalocalcaneal arthrodesis with subtalar nonunion requiring a revision subtalar fusion.
Postoperatively, patients were immobilized in a well-padded short leg splint with the ankle in neutral. Following suture removal at 2 weeks, patients were transitioned to a removable night splint and controlled ankle motion (CAM) walking boot. At this time, weightbearing deep knee bends and Achilles stretching was initiated, as described previously. 23 No weightbearing ambulation was permitted in the first 6 weeks. After 6 weeks, weightbearing with ambulation was permitted, with progression to full weightbearing in a walking boot over the course of 4 weeks. At 12 weeks postoperatively, patients transitioned out of the boot to a cloth brace, which they weaned as tolerated.
Statistical Analysis
Descriptive statistics for characteristics of patients and clinical measurements were presented as means and SDs, and frequencies for categorical variables. Paired t tests were used to compare mean preoperative and latest postoperative radiographic alignment measures and PROMs. A variable with P value <.05 indicates a significant difference between 2 groups. All analysis was performed using SAS 9.4 (SAS Institute Inc).
Results
A total of 16 ankles (16 patients; 9 ankle fusion, 7 tibiotalocalcaneal fusion) met the inclusion and exclusion criteria and were included in the current study with an average follow-up of 4.7 (range, 2-11) years. All patients had presented with pain and stiffness of the ankle and adjacent joints. Of the 7 patients who had previously underwent tibiotalocalcaneal fusion, 1 patient presented with subtalar nonunion and 1 patient presented with tibiotalar nonunion. There were no nonunions in the 9 patients who previously underwent tibiotalar fusion.
The study cohort consisted of 62% females, with an average age of 56.8 (range, 25-75) and body mass index of 30.6 (range, 20-47). A quarter of patients (n = 4) had a diagnosis of diabetes, and 15 (93.8%) patients had an ASA score of 2 or 3 (Table 1). All but 1 patient underwent additional concomitant procedures at the time of fusion takedown
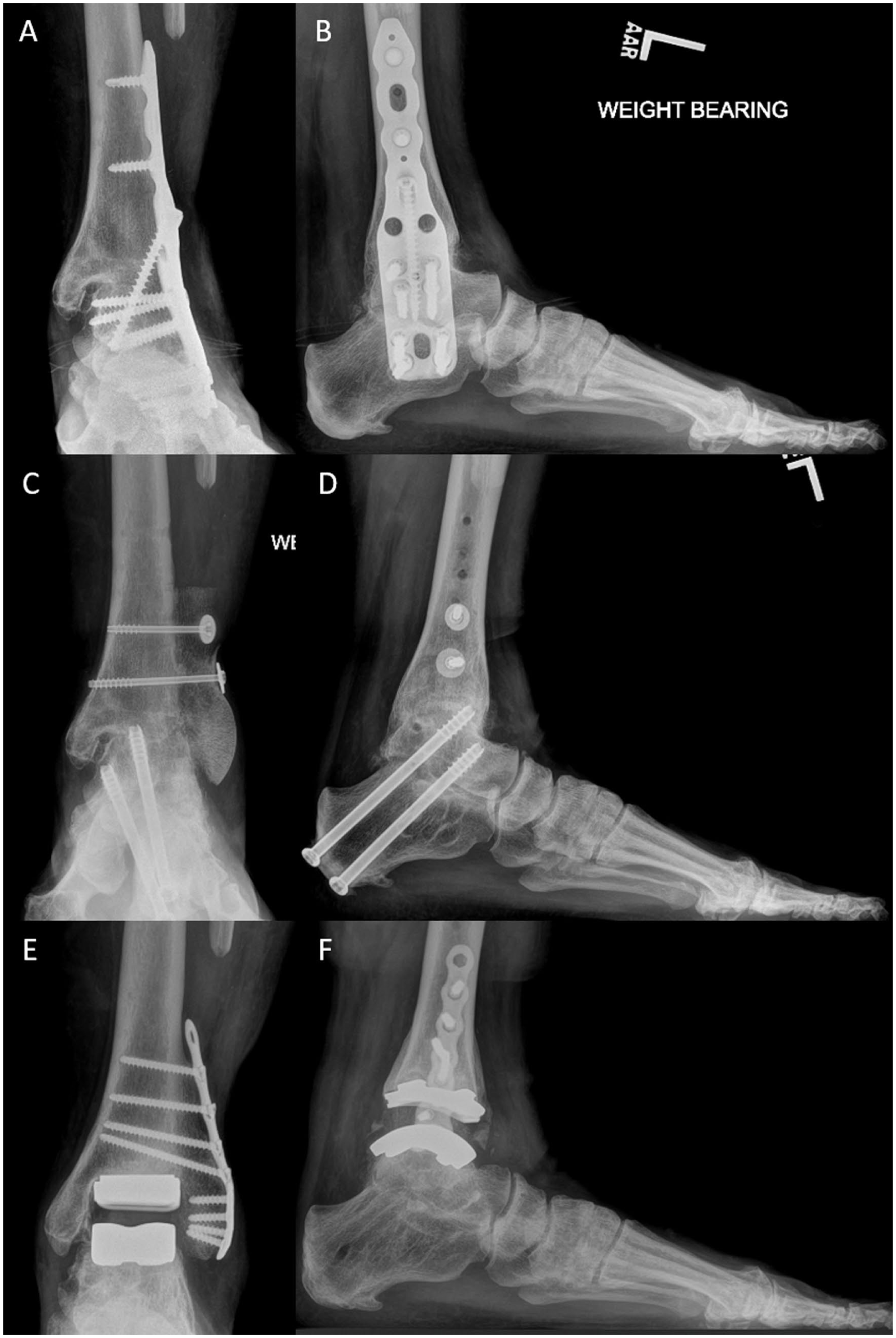
Weightbearing plain films of a 55 year-old woman with previous history of multiple ankle surgeries in the setting of posttraumatic arthritis who underwent conversion of ankle arthrodesis to transfibular total ankle arthroplasty (TAA). Anteroposterior (AP) and lateral radiographs demonstrate her initial presentation with painful subtalar nonunion in the setting of a failed tibiotalocalcaneal arthrodesis (A and B). She underwent a staged revision; the first stage consisted of hardware removal, revision subtalar fusion, and fibular reconstruction using a femoral head allograft (C and D). At 7 months she successfully underwent conversion to transfibular TAA. Weightbearing films obtained 30 months following conversion to TAA demonstrate satisfactory alignment and implant retention (E and F).
There was significant mean improvement in all PROMs at final follow-up (Table 3). Average SF-12 PCS increased from 36.0 ± 4.2 to 42.2 ± 6.6, SF-12 MCS increased from 46.7 ± 8.1 to 54.2 ± 8.3, VAS pain improved from 7.0 ± 1.8 to 3.3 ± 1.4, AOS pain improved from 55.4 ± 19.1 to 25.0 ± 20.2, and AOS disability improved from 57.6 ± 17.2 to 41.1 ± 20.9 (all P < .05).
Patient-Reported Outcome Measures (PROMs).
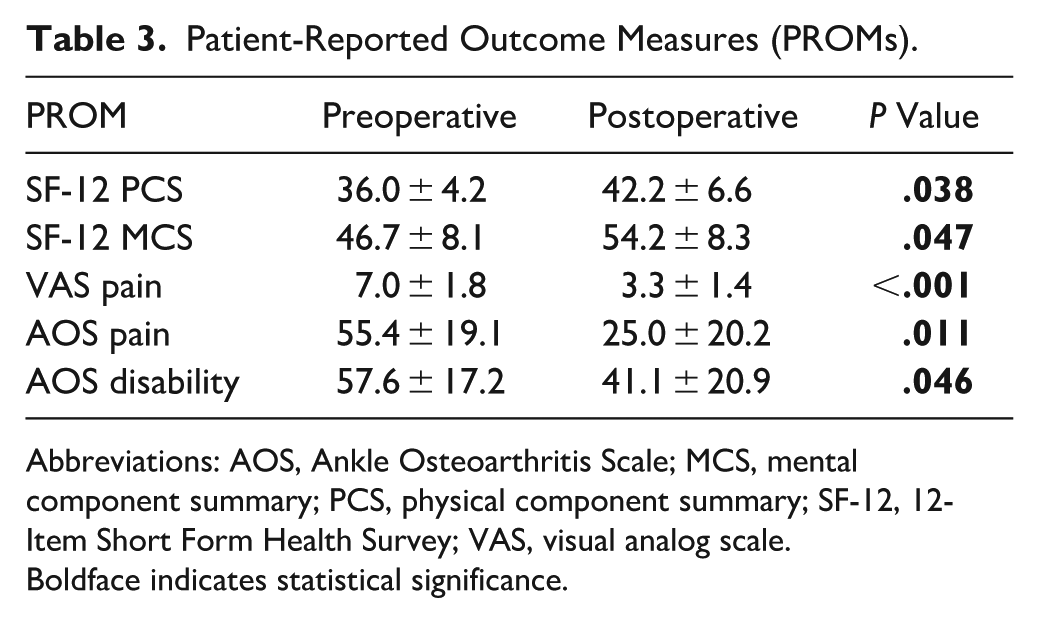
Abbreviations: AOS, Ankle Osteoarthritis Scale; MCS, mental component summary; PCS, physical component summary; SF-12, 12-Item Short Form Health Survey; VAS, visual analog scale.
Boldface indicates statistical significance.
Radiographic coronal and sagittal tibiotalar alignment is recorded in Table 4. Postoperatively, the mean tibiotalar dorsiflexion and plantarflexion were 12.5 ± 5.6 degrees and 13.5 ± 9.1 degrees, respectively. In terms of periprosthetic radiolucency, a single zone of radiolucency (<2 mm) was observed in 12 (75%) ankles at final follow-up, most commonly about the anterior and posterior tibial tray. No periprosthetic cysts (radiolucency >2 mm) were observed in any cases.
Radiographic Outcomes and Range of Motion (N = 16).

Adverse events occurred in 9 patients (56.3%); 1 patient (6.3%) underwent implant revision, 8 patients (50%) underwent a total of 10 reoperations. Reoperations were performed at an average of 1.5 years and included: isolated removal of fibular hardware (n = 4), medial gutter debridement (n = 4), irrigation and debridement with polyethylene liner exchange (n = 1), and tendon Achilles lengthening (n = 1). The one patient who underwent implant revision had sustained an acute, traumatic periprosthetic fracture requiring revision of the tibial component at 10 weeks postoperatively.
There was 1 incidence of delayed incisional healing that prompted delayed suture removal at 4 weeks. Another patient had a superficial infection that resolved after course of oral antibiotics.
Discussion
Symptomatic, failed ankle fusion remains a challenging clinical scenario in which revision options are limited. To our knowledge, this is the first study investigating takedown fusion with conversion to transfibular total ankle arthroplasty. In this series of 16 ankles, patients were found to have significant improvements in patient-reported outcomes and improved tibiotalar ROM at an average of 4.7 years follow-up. Half of the patients required at least one reoperation, and overall implant survivorship during the study period was 93.7%.
The decision to undergo transfibular TAA over conventional anterior approach requires a comprehensive assessment of patient risk factors and previous surgical history. Data for transfibular total ankle arthroplasty is favorable in the primary setting; however, there is a scarcity of evidence in the takedown setting.20,24 Previous studies have reported favorable results in subjective and functional patient outcomes following takedown fusion with conversion to an anterior ankle system, including the Agility (DePuy) Salto Talaris (Smith & Nephew), Scandinavian Total Ankle Replacement (STAR, Enovis), Infinity (Stryker), Inbone (Stryker), and Hintegra (DT MedTech) prostheses.7 -9,25 -27 Our study adds to this growing body of literature with a novel method of management.
An advantage of this study is the inclusion of pre- and postoperative clinical and radiographic outcomes at a minimum of 2-years follow-up. At an average of 4.7 years following fusion takedown with conversion to TM TAA, there was significant improvement in pre- to postoperative PROMs. Furthermore, mean postoperative VAS, AOS pain, AOS disability, SF-12 PCS, and SF-12 MCS scores are consistent with the 5-year results of a series of 130 cases of primary transfibular TAA. 24 Our findings suggest that although fusion takedown with conversion to TAA may be more complex of a procedure, patients with painful, failed tibiotalar fusions can achieve reasonable symptomatic and functional improvement.
All patients regained varying degrees of radiographic ROM following fusion takedown with conversion to TM TAA, from 0 degrees of tibiotalar motion preoperatively. Furthermore, it was observed that ROM increased over the course of follow-up, which is consistent with previous published findings.7,28 These findings suggest that patients can reasonably expect to have improved tibiotalar dorsiflexion and plantarflexion following conversion of tibiotalar arthrodesis to TAA within the first 2 years.
Implant survivorship in this series was 93.7%, with 1 patient requiring implant revision. Although this may be slightly lower than that of primary TM TAA,29,30 these findings are within the range of implant survivorship reported in previous takedown studies by Schuberth et al 8 (88%) and Lundeen et al 7 (98%). The patient who underwent revision had sustained a traumatic fall at 10 weeks postoperatively, resulting in a periprosthetic tibial fracture through a bone void from previous hardware removal. This necessitated revision of the tibial component, and the patient recovered well postoperatively.
It is important to counsel patients that risk for surgical reoperation is relatively high. In a systematic review of 919 primary TM TAA cases across 7 countries, Fa-Binefa et al 30 reported that about a quarter of patients experienced adverse events postoperatively, and 18% of patients required surgical reoperation within a follow-up period of 3 years. In contrast, half of the patients in this current series required surgical reoperation at an average of 1.5 years following fusion takedown. This finding is likely attributed to the complex surgical history and revision nature of the patients in this current series. Indications for surgical reoperation, however, are similar to that of primary TM TAA, with removal of symptomatic hardware and gutter debridement for impingement being the most common reoperations.29,30
Results of the current study should be interpreted in light of several limitations, including its retrospective design, the use of a single-surgeon database, and limited sample size. Future prospective studies with larger cohorts and longer follow-up are recommended to further validate these findings. Furthermore, we acknowledge that fusion takedown and conversion to TAA is a challenging procedure with a moderate reoperation rate, and should be performed by experienced surgeons.
Conclusion
Although technically challenging, fusion takedown with conversion to transfibular, trabecular metal total ankle arthroplasty is a reasonable treatment option for symptomatic ankle arthrodesis, yielding improvements in clinical and functional outcomes at an average of 4.7 years’ follow-up. Although implant survivorship in this series was high, patients should be counseled on a moderate risk for surgical reoperation.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261422697 – Supplemental material for Outcomes Following Conversion of Ankle Fusion to Transfibular Total Ankle Arthroplasty
Supplemental material, sj-pdf-1-fao-10.1177_24730114261422697 for Outcomes Following Conversion of Ankle Fusion to Transfibular Total Ankle Arthroplasty by Mark Arthur, Thomas Wood, Morgan Motsay, Jonathan Day, Zijun Zhang and Lew Schon in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from Mercy Medical Center Institutional Review Board (Approval ID: 1648405-15).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lew Schon, MD, reports general disclosures of Zimmer: IP royalties; paid consultant; paid presenter or speaker; research support. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.