
Abstract
Background:
Metal implants, the gold standard for osteotomy fixation in foot surgery, do have inherent problems. A relatively high percentage of patients undergoing hallux valgus correction require secondary surgery for metal implant removal. Although available since the 1980s, bioabsorbable implant use in foot surgery has been limited because of concerns of osteolysis and inferior strength. Magnesium screws are bioabsorbable implants without the inherent risks associated with other bioabsorbable implants. We prospectively compared outcomes of MAGNESIX to metal implants in hallux valgus deformity correction.
Methods:
A prospective, randomized study comparing radiographic and clinical outcomes between hallux valgus corrections fixated with magnesium (24 feet) or titanium (25 feet) screws, with an average follow-up of 44 and 35 months, respectively. Clinical outcomes were assessed using the American Orthopaedic Foot & Ankle Society (AOFAS) forefoot score and radiographic parameters measured on weightbearing radiographs pre-operatively and at final follow-up. All complications were documented.
Results:
Both magnesium and titanium cohorts showed statistically significant improvements in radiographic parameters (P < .05) and AOFAS scores (P < .05), with no statistically significant difference between cohorts.
All post-operative radiographs in the magnesium cohort had visible gas formation at 6 weeks, resolving by 12 weeks, and all screws fully resorbed on final radiographs with no evidence of osteolysis (more than 1 year). Four recurrences occurred in the magnesium cohort vs 3 in the titanium cohort. A single case of hallux varus was noted in the magnesium group and 1 incidence of screw removal for symptomatic hardware in the titanium group.
Conclusion:
We found no difference between bioabsorbable magnesium screws and titanium screws for fixation in hallux valgus surgery, although small between-group differences may not have been detectable given the relatively small sample size. Magnesium screws appeared safe with no allergic reactions or wound complications and may offer added benefits of not interfering with advanced imaging, decreasing the need for hardware removal and likely easier revision surgery.
Level of Evidence:
Level II, randomized controlled trial.
Introduction
More than 150 surgical procedures have been described for the correction of a hallux valgus (HV) deformity.1,2 Most osteotomies used to manage hallux valgus deformities are fixed with stainless steel or titanium metallic implants. 3 These metals have good mechanical strength, biocompatibility, and corrosion resistance. 3 However, metallic implants are associated with stress shielding, metal debris production, growth restriction, implant loosening, migration, hypersensitivity reactions, and may be associated with persistent pain.3 -5 They also interfere with advanced imaging such as computed tomography (CT) and magnetic resonance imaging (MRI) scans.3,4 Another concern is that foot and ankle implants are more commonly associated with soft tissue irritation because of their subcutaneous location and use in weight-bearing areas, which then requires removal. 6
Coughlin 14 reported that 15% of patients undergoing hallux valgus correction required a second surgery for implant removal. This was confirmed by Bard et al 15 in their systematic review, which reported that up to 16% of cases required hardware removal. Metal hardware removal can be technically difficult owing to bony ingrowth, stripping of screw heads and implant breakage. Significant bone removal to access the metal hardware may compromise the integrity of the bone itself, making revision hallux valgus surgery difficult. Magnesium screws do not require removal as they resorb and are replaced by cancellous bone.
In contrast, biodegradable materials have reduced interference with imaging, a Young’s modulus closer to bone and reduced need for implant removal.3,5,7 Most commonly used bioabsorbable polymers include poly-
Biodegradable metallic implants made of iron (Fe), zinc (Zn) or magnesium (Mg) have all been researched. 4 Pure magnesium, which has been used in vivo since the early 20th century, is a naturally occurring element in the body with mechanical properties similar to cortical bone and leads to alkalinization of its surrounding environment during degradation, which is antibacterial, osteoinductive and pro- osteoblastic.3,4,6,7 The degradation products may even have an analgesic effect. 7 Magnesium-based implants biodegrade via corrosion rather than hydrolysis, corrosion having a blunted inflammatory response minimising osteolysis. 6 The rate of this corrosion reaction is critical for its clinical use; if it occurs too quickly, the implant may lose its initial strength before bony union and may produce locally toxic amounts of hydrogen gas. 1
Historically, pure magnesium was used for cardiac implants; however, animal-based research reported a significant velocity of hydrogen gas formation, leading to local tissue displacement and reduced mechanical stability.3,11 Specific alloying elements (such as yttrium and zirconium) have improved the mechanical characteristics and degradation properties of magnesium-based implants. 4 Several animal studies have confirmed the excellent safety profile of magnesium alloy implants. 3 The MAGNEZIX screw (Syntellix AG) was the first magnesium-based bone implant to be approved for in vivo human use in 2013.1,9 It is composed of magnesium (>90%), yttrium, rare earth metals, and zirconium (MgYREZr).1,9 Up to 50% degradation of the implant occurs by 12 weeks, and full degradation occurs over 1-2 years.6,8 -10
The current available literature regarding the use of magnesium screws in foot surgery is largely limited to small case series and short term follow-up.2,4,6,8,10 The aim of this study is to prospectively compare MAGNESIX (Syntellix AG) and titanium screws for the fixation of metatarsal and proximal phalanx osteotomies used in the management of hallux valgus, with regard to clinical, radiologic and functional outcomes.
Materials and Methods
This prospective, randomized study was approved by our institution’s ethics committee. All consenting patients over the age of 18 years who underwent a primary hallux valgus correction procedure during the study period between January 2019 and December 2020 were included. Any patients declining to participate and those having revision surgery were excluded. Patients were randomized into each cohort by blindly selecting either a MAGNESIX (Syntellix AG) or titanium (Paragon 28 Inc) screws envelope from a box.
Forty patients were randomized; 19 patients (24 feet) were included in the magnesium cohort and 18 patients (25 feet) in the titanium cohort. Three patients were lost to extended follow-up because of emigration or loss of contact. Six patients in both the magnesium and titanium cohorts had bilateral simultaneous procedures. One patient was included in both the magnesium cohort and the titanium cohort, as the patient was randomized into both cohorts by having staged correction of bilateral hallux valgus deformities.
Average age was 59 (range: 42-79) years in the magnesium cohort and 58 (range: 25-77) years in the titanium cohort. There were no males in the magnesium cohort and 3 (17%) males in the titanium cohort. Average follow-up time was 44 (range: 13-74) months for the magnesium cohort and 35 (range: 12-75) months for the titanium cohort. Patients presented with a spectrum of comorbidities as reported in Table 1.
Breakdown of Medical Comorbidities Seen in Each Cohort.

Patients completed the American Orthopaedic Foot & Ankle Society Hallux metatarsophalangeal-interphalangeal (AOFAS MTP-IP) score pre-operatively and at their latest post-operative visit. Weight-bearing radiographs of the operated foot (feet) were done pre-operatively and at 6 weeks, 12 weeks and final follow-up post-operatively. The hallux valgus angle (HVA), intermetatarsal angle (IMA) and distal metatarsal articular angle (DMAA) were measured. Radiographs were assessed for union, hardware failure, hydrogen gas formation, resorption of hardware and osteolysis.
Surgeries were carried out by 2 fellowship-trained foot and ankle surgeons. Each surgical plan was decided pre-operatively based on clinical and radiographic parameters. All cases were done under sterile conditions, under tourniquet cover with general and regional anaesthesia. Table 2 provides a summary of the different procedures done in each cohort.
Summary of the Number of Times Each Surgical Procedure Was Performed in Each Cohort. a

The procedures done with magnesium are in bold (ie, scarf, BOAT, chevron, Akin). Procedures done with titanium implants are not in bold (ie, Lapidus, POW). Note: Some procedures were often combined, ie, Lapidus, chevron, and Akin; hence surgical procedures done are higher than included patients.
Magnesium and titanium screws were used to fix scarf (2 screws), best of all technique (BOAT) (2 screws), chevron (1 screw), medial closing wedge chevron (MCWC) (1 screw) and Akin (1 screw) osteotomies. Fixation was done with either a 2-mm titanium screw (Paragon 28 Inc) or 2-mm MAGNESIX screw (Syntellix AG). Additional procedures were done as deemed necessary (Table 3).
List of the Procedures Done in Addition to Hallux Valgus Correction in Each Cohort.
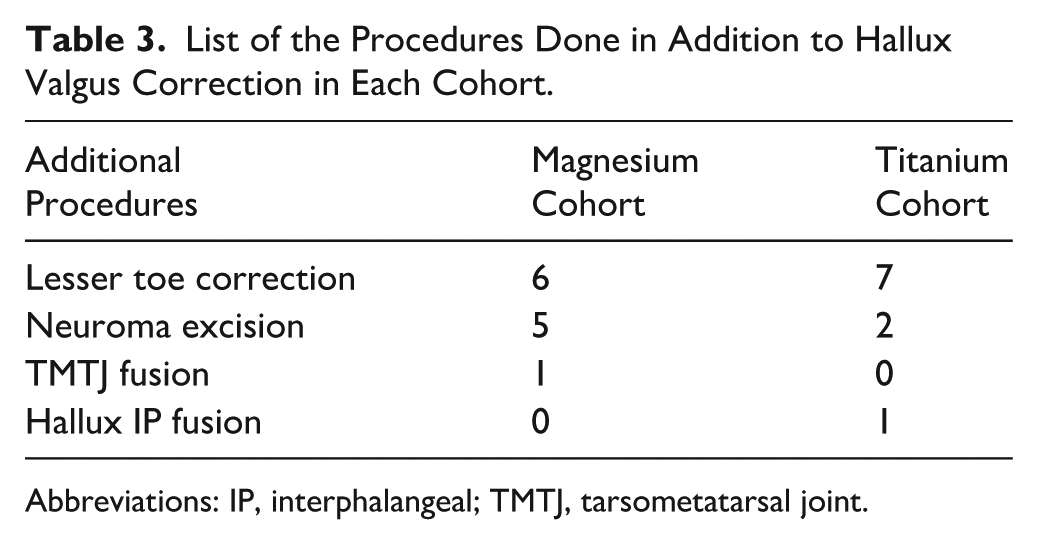
Abbreviations: IP, interphalangeal; TMTJ, tarsometatarsal joint.
All wounds were routinely closed in a layered fashion using absorbable sutures. Patients were placed in a heel-wedge shoe day 1 post-surgery and allowed to weight-bear as tolerated. Patients were instructed to keep the foot elevated for the first 2 weeks. At 6 weeks, patients were allowed to transition into supportive shoes and referred to physiotherapy for rehabilitation.
Statistical Analysis
A paired samples t test was conducted separately for the magnesium and titanium groups to assess whether there was a statistically significant improvement in patient-reported outcome scores from pre-operative to post-operative measurements. An independent samples t test was performed between the 2 groups to determine whether the improvement differed significantly between the magnesium and titanium screw groups. Independent samples t tests were performed on the amount of correction for each radiographic parameter (HVA, IMA, DMAA) to evaluate whether there was a statistically significant difference in mean radiographic correction between the 2 independent (magnesium and titanium) cohorts.
Results
Average amount of radiographic angular correction from pre- to post-operatively in the magnesium cohort was 12 degrees for the HVA, 8 degrees for the IMA and 5 degrees for the DMAA, and in the titanium cohort 15 degrees for the HVA, 6 degrees for the IMA and 6 degrees for the DMAA. The radiographic correction was statistically significant in both the magnesium and titanium screw cohorts (P < .05). The mean pre- and post-operative radiographic measurements are reported in Table 4. No statistically significant difference between the 2 cohorts was seen.
Comparison of Radiographic Parameters (Average and Ranges) and AOFAS Scores Pre- and Post-operatively in the Magnesium and Titanium Screw Cohorts.

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society; DMAA, Distal Metatarsal Articular Angle; HVA, hallux valgus angle; IMA, intermetatarsal angle.
Both the magnesium and titanium cohorts showed significant improvements (P < .05) in AOFAS scores from pre-operative (mean of 55 [24-72] for magnesium and mean of 50 [28-80] for titanium) to post-operative scores (mean of 92 [67-100] for magnesium and 93 [62-100] for titanium), with no statistically significant difference between the 2 cohorts (Table 4). Patients who had simultaneous bilateral surgeries had no significant outcome difference to patients who had single surgeries, and the patient who had 1 foot fixated with magnesium and 1 foot with titanium screws showed no difference in outcome between feet. Additional procedures did not significantly affect outcome scores compared with isolated hallux valgus correction.
We observed 4 recurrences in the magnesium cohort vs 3 recurrences in the titanium cohort, which was not statistically significant. One case of hallux varus was seen in the magnesium group.
All patients in the magnesium cohort had visible gas formation on radiographs at 6 weeks, which resolved by 12 weeks with all magnesium implants being resorbed on final radiographs (after more than 1 year) (Figure 1). We had no wound complications, infections or hardware-related complications in either cohort. One patient in the titanium cohort required screw removal for symptomatic hardware, with no removals required in the magnesium cohort.

The progression of radiographs from pre-operative, 6 weeks post-operative and the final images in patients who underwent Lapidus, chevron and Akin procedures. Please note the gas formation in both patients at 6 weeks that is completely resolved and replaced by remodelling bony trabecular at final imaging. (A) Right hallux valgus correction with 3-year follow-up. (B) Bilateral hallux valgus correction with 4-year follow-up.
Discussion
In this modest-sized randomized trial with medium-term follow-up, both magnesium and titanium screws produced statistically significant improvements in radiographic correction (HVA, IMA and DMAA) and AOFAS scores, with no statistically significant between-group differences. Complication profiles were similar, with comparable recurrence rates and no implant failures in either cohort; the magnesium group had no hardware removals, whereas 1 symptomatic screw removal occurred in the titanium group. All magnesium cases demonstrated transient peri-implant gas formation/radiolucency at 6 weeks that resolved, and final radiographs showed complete screw resorption without osteolysis, replaced by remodeled trabecular bone. Taken together, these findings indicate that magnesium screws appear to be a safe and effective alternative to titanium fixation for hallux valgus osteotomies, while offering practical advantages such as avoiding long-term imaging artefact and eliminating the need for routine hardware removal.
Despite being available since the 1980s, bioabsorbable implants have been avoided in foot surgery due to concerns of osteolysis and inferior strength as compared to their metal counterparts.4,8 -10 More recently, studies have shown that magnesium alloy biodegradable screws show biocompatibility and osteoconductivity with osteogenic potential and no reported allergic reaction.9,12,13 Sahin et al 5 reported that magnesium screws offer the same mechanical stability as titanium screws in the fixation of chevron osteotomies in saw bone models. These osteoanabolic characteristics, degradation via corrosion rather than hydrolysis, modulus of elasticity similar to bone and mechanical stability purport it as an exciting prospect for fixation of osteotomies in foot surgery. 4
Metal implants are the gold standard for fixation of osteotomies in foot surgery. The problems with using metal implants include the interference with advanced imaging modalities (CT and MRI), necessity for removal due to pain and stress shielding of bone due to its higher modulus.3,4,6 Even if the implant has not been absorbed completely, it can be cut through with an oscillating saw during revision surgery, if needed. 16 Fu et al 13 in a meta–analysis comparing titanium and magnesium screws in distal metatarsal osteotomies reported a 2.9% removal rate in the titanium group (none in the magnesium group) with similar rates of infection. Our study had no failure or removal of the magnesium screws and 1 hardware removal in the titanium cohort.
Recent publications have reported on the use of MAGNEZIX (Syntellix AG) screws in orthopaedic surgery as well as comparing it to titanium screws in the treatment of hallux valgus deformities. No significant differences were found between the 2 types of fixation.2 -4,6,8,13 However, these reported outcomes were limited in that few studies were comparative and majority were pilot studies of small cohorts with short follow-up. Windhagen et al 8 performed the first prospective, randomised control study comparing chevron osteotomies fixed with biodegradable magnesium screws vs titanium screws in a small group of 26 patients (13 patients in each cohort). No difference in clinical and radiographic parameters was noted. Their 6-month follow-up, however, is too soon for the implant to have resorbed and comment on possible implant-related degradation problems. Plaass et al 4 looked at clinical and radiologic outcomes following chevron osteotomy fixation in 40 patients using bioabsorbable magnesium screws. With a very short average follow-up of only 5 months, they reported significant improvements in all parameters. Klauser 2 reported on the largest case series with 100 patients undergoing metatarsal osteotomies for hallux valgus surgery using magnesium screws and retrospectively compared them to 100 patients who had titanium screws used for the same procedure. The author reported 1 breakage in the magnesium screw cohort and 1 screw removal in the titanium group. 2 The study concluded magnesium screws were similar to titanium screws, but with only a 3-month follow-up it is too short to derive conclusive outcomes. 2 Our prospective comparative analysis of titanium vs magnesium screws with a mean follow-up of 35 and 44 months respectively is, to our knowledge, the longest follow-up study in the literature.
Choo et al 3 compared scarf osteotomies fixed with magnesium screws to a control group using titanium screws. The AOFAS improved from 65.8 to 89.5 in the magnesium group and 63.8 to 83.6 in the titanium group; both groups showing statistically significant improvements at 1 year and no statistically significant difference between groups. 3 Atkinson et al 6 compared a short scarf osteotomy for hallux valgus fixed with magnesium (11 patients) and titanium (25 patients) screws at a median of 19 months and demonstrated no functional difference. Wendelstein et al 12 retrospectively compared magnesium screws to other fixation methods and reported that the magnesium cohort had the highest satisfaction rate and most improved IM angle correction at 1 year. Our study had similar good clinical and functional outcomes, as reported by the significantly improved AOFAS scores in both cohorts (from 55 to 92 for magnesium and 50 to 93 for titanium cohorts).
Animal studies suggest magnesium alloy screws should be completely degraded by 1-2 years.9,10 Plaass et al 10 compared MRI features in distal metatarsal osteotomies fixated with magnesium (8 patients) or titanium (6 patients) screws at 3 years. Magnesium screws showed significantly less artefacts, no implant-related cysts, profound bone healing, and a hypointense structure similar to cortical bone had replaced the implant. 10 We confirmed on plain radiographs that all magnesium implants were fully resorbed and replaced with bone at final follow-up with no implant-related cysts. 10 Hydrogen gas production during magnesium screw degradation can be mistakenly interpreted as lysis or infection in early follow-up radiographs. 1 Our magnesium cohort all had hydrogen gas formation and radiolucencies on 6-week radiographs, which all resolved at 12 weeks. Radiolucent lines can develop around the implant in the first 6 months and must not be mistaken for implant loosening.1,2 We did not identify any gas or hardware-associated lucencies in any of our final post-operative radiographs1,7 We confirm the safety of the magnesium-based implants as we had no allergic reactions, wound breakdowns, or infections.
The current study provides evidence that hallux valgus deformity correction is maintained following complete degradation of the implant. We included a diverse severity of hallux valgus deformities and various procedures required to correct them. Previous studies focused primarily on a single metatarsal osteotomy (chevron or scarf), generally reserved for mild to moderate deformities. Although the Lapidus and proximal opening wedge (POW) osteotomy themselves were not fixed with magnesium implants, the associated distal fixations were. This adds to the resistance to mechanical stress required by the implants and as such reinforces the notion of similar mechanical stability of magnesium screws. Our data support the literature that magnesium screws are suitable for fixation of osteotomies in hallux valgus surgery and we provide clinical and radiographic data confirming its similarity to titanium screws.
Although this study was not undertaken as a financial analysis, some inference can be made. The price of a magnesium screw was US$216.47 and a titanium screw US$205.43; a difference of US$11.04. On average, 2 screws were used per case, which is a difference of US$22.08 more when using MAGNESIX (Syntellix AG) screws. This is a minor cost implication and if hardware removal of metal screws is taken into consideration the financial implication of using MAGNESIX (Syntellix AG) screws is negligible. Hallux valgus revision surgery is commonly performed for symptomatic hardware, recurrence of deformity or degeneration of the hallux MP joint; because of this, magnesium screws are an attractive option, with qualities listed above making revision easier, reduced risk of symptomatic hardware and minimal increased cost.
The strengths of this study are that we provide a randomized, prospective study with the longest follow-up and most diverse study in terms of hallux valgus severity. We do acknowledge our limitations include a limited number of patients (20 patients per cohort) with a diverse array of procedures, limiting the ability to extrapolate data for each individual procedure itself. Some patients as described above had bilateral procedures and each foot was used independently, perhaps adding some bias. The use of CT scan evaluation at final follow-up would have improved the understanding of what occurs after the magnesium implants resorb; although it appears that absorbed screws are replaced with remodelling bony trabeculae, this needs to be confirmed on CT scan. The AOFAS (MTP-IP) scoring system is not a validated scoring system; it was used in this study to compare to previous similar studies found in the literature but studies going forward would in fact benefit from using validated scoring systems.
Conclusion
We found bioabsorbable magnesium screws to be similar to titanium screws for the fixation of osteotomies used for correcting hallux valgus deformities, although small between-group differences may not have been detectable given the relatively small sample size. Magnesium screws were safe with no allergic reactions or wound complications and have the added benefits of not interfering with advanced imaging, eliminating the need for hardware removal and potentially easier revision surgery.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251408829 – Supplemental material for Magnesium Bioabsorbable vs Titanium Screws in Hallux Valgus Surgery: A Prospective, Randomized Medium-term Trial
Supplemental material, sj-pdf-1-fao-10.1177_24730114251408829 for Magnesium Bioabsorbable vs Titanium Screws in Hallux Valgus Surgery: A Prospective, Randomized Medium-term Trial by Nikiforos P. Saragas, Michael de Buys and Paulo N. F. Ferrao in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Approval from the University of the Witswatersrand Human Research Ethics Committee (Clearance Certificate no: M181140).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.