
Abstract
Introduction
Hallux valgus disease is a deformity in which various intrinsic and extrinsic factors play a role in its pathophysiology. The disease is characterised by the deviation of the first metatarsal medially and the first toe to the lateral. It is the most common deformity in the foot and is more common in females.1,2
There are over 130 different surgical techniques described in the last 100 years for hallux valgus surgery. Internal fixation is essential for the corrected deformity to be permanent. The indication for the surgery and surgical method to be applied are planned according to the severity of the deformity.3,4
The distal chevron osteotomy (DCO) technique is widely used to correct mild and moderate deformities. Initially, this technique was considered without internal fixation in the studies by Miller and Croce and Austin and Leventen.5,6 In their opinion, due to the shape of the osteotomy, the impaction of the cancellous fragment of the metatarsal head to the metatarsal shaft provided sufficient stability and no additional fixation was required. However, subsequent studies introduced various fixation materials such as K-wires, staples and screws to reduce displacement of the metatarsal head, resulting in a more controlled correction.7,8
Although titanium implants are typically preferred in hallux valgus surgery, the popularity of bioabsorbable implants such as magnesium has increased recently. These absorbable implants have some advantages over conventional metallic implants. They do not cause artefacts in radiological imaging, especially in magnetic resonance imaging.9,10 Compared to titanium and stainless steel, Young’s modules are more similar to normal bone and thus have lower levels of stress shielding.9,11,12 Their fixation stability is similar to titanium, and they do not cause implant removal due to their biodegradability.12,13 Implant removal has risks such as scarring, infection and neurovascular injury, adversely affecting health economics when a second surgery is required.14–16
In recent years, clinical studies on the use of bioabsorbable magnesium screws in the surgical treatment of hallux valgus have been published. 12 However, there is no comparative biomechanical study of titanium and magnesium screws. Therefore, this study aims to investigate and compare biomechanical properties of the fixation of DCO with two alternative fixation materials. The study hypothesises that the magnesium screw provides as much stability as the titanium screw in DCO.
Materials and methods
This study used 20 standard bone models of the left first metatarsal made of solid foam (Sawbones, Malmo, Sweden). The models were divided into two equal groups containing ten sawbones for fixation with a single headless magnesium or titanium screw. DCO was performed on all samples using the same technique and equipment. Titanium screw fixation was Group-1, and magnesium screw fixation was Group-2. Biomechanical tests were applied to five samples in each group, five in a cantilever configuration and five in a physiological configuration.
Osteotomy and fixation
DCOs were performed using the method in Rossi and Ferreira’s study.
17
The apex of the osteotomy was positioned just distal to the medial eminence, in the centre of the metatarsal head. The angle of the osteotomy was 60°. A 0.6 mm saw blade was used for the osteotomy, and the distal fragment was shifted 5 mm laterally.
17
Subsequently, the dorsomedial screw entry point on the proximal fragment was determined by measuring equidistance from the osteotomy apex. Screws were applied after drilling over the K-wire placed at an angle of 10–15° dorsoplantar and 30–40° mediolateral from this entry point. Thus, the fixation process was standardised by ensuring that the screw entry-exit points, angle and screw lengths were the same for all specimens (Figure 1). a) 60° distal chevron osteotomy with the apex in central of metatarsal head b) Determination of screw entry–exit points and temporary fixation with K-wire c) Dorsomedial entry point of the screw – dorsal view of fixation d) Lateral view after fixation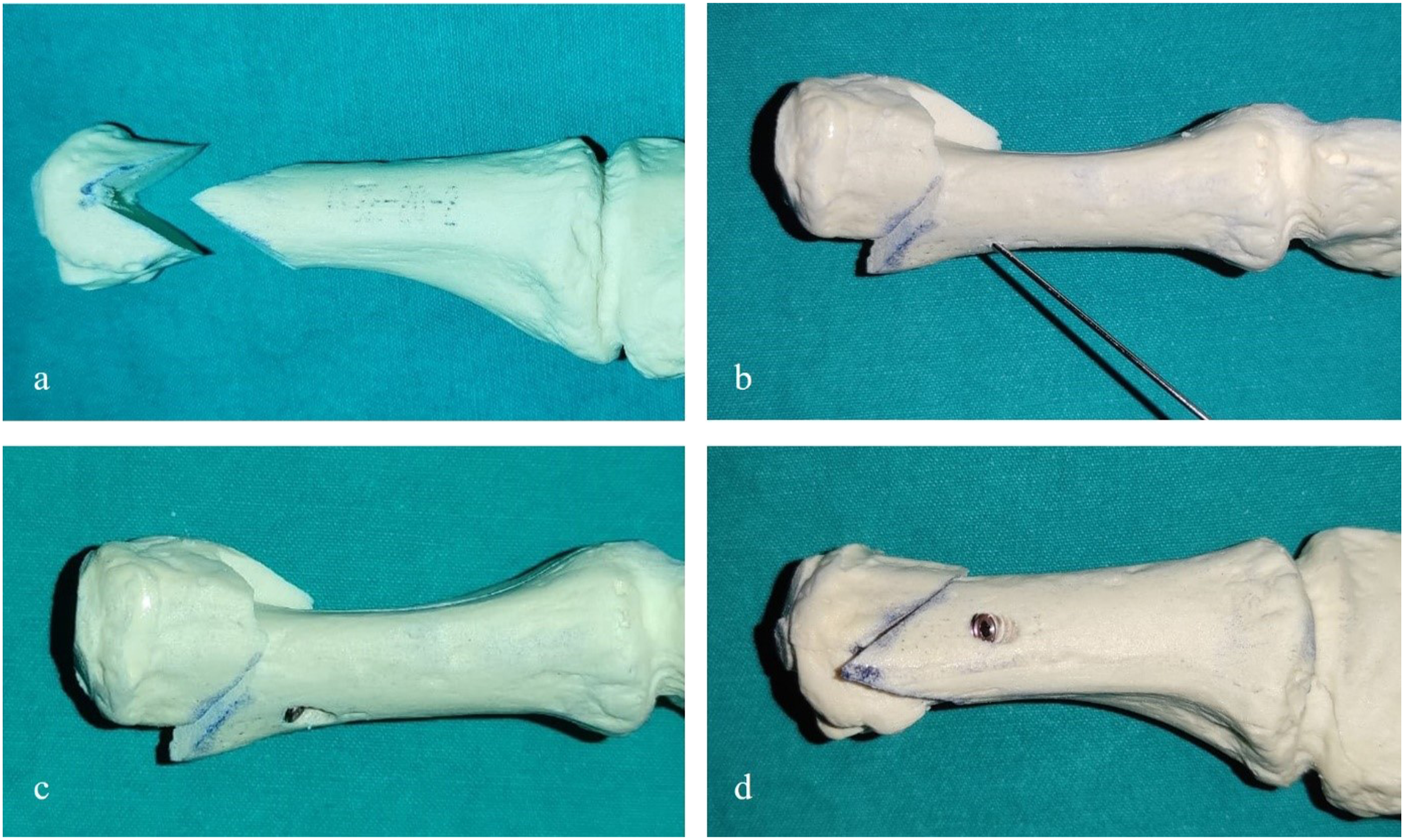
For the fixation, titanium and magnesium screws with the same design and sizes were provided. Group-1 was fixed with a 2.7 x 26 mm titanium screw (Ti-Al-V alloy/ TST Medical Devices – headless cannulated compression screw, Istanbul, Turkey), group-2 was fixed with a 2.7 x 26 mm magnesium screw (Mg-Ca-Zn alloy/ Resomet™ – bioresorbable headless cannulated compression screw, U&I Corporation, Seoul, South Korea) and then screw configurations were checked by taking AP and lateral fluoroscopy images (Figure 2). All this created equal and standardized conditions for biomechanical comparison. a) 2.7 x 26 mm magnesium and titanium screws used in fixation b) AP view of control fluoroscopy after fixation with magnesium and titanium screw c) Lateral fluoroscopy image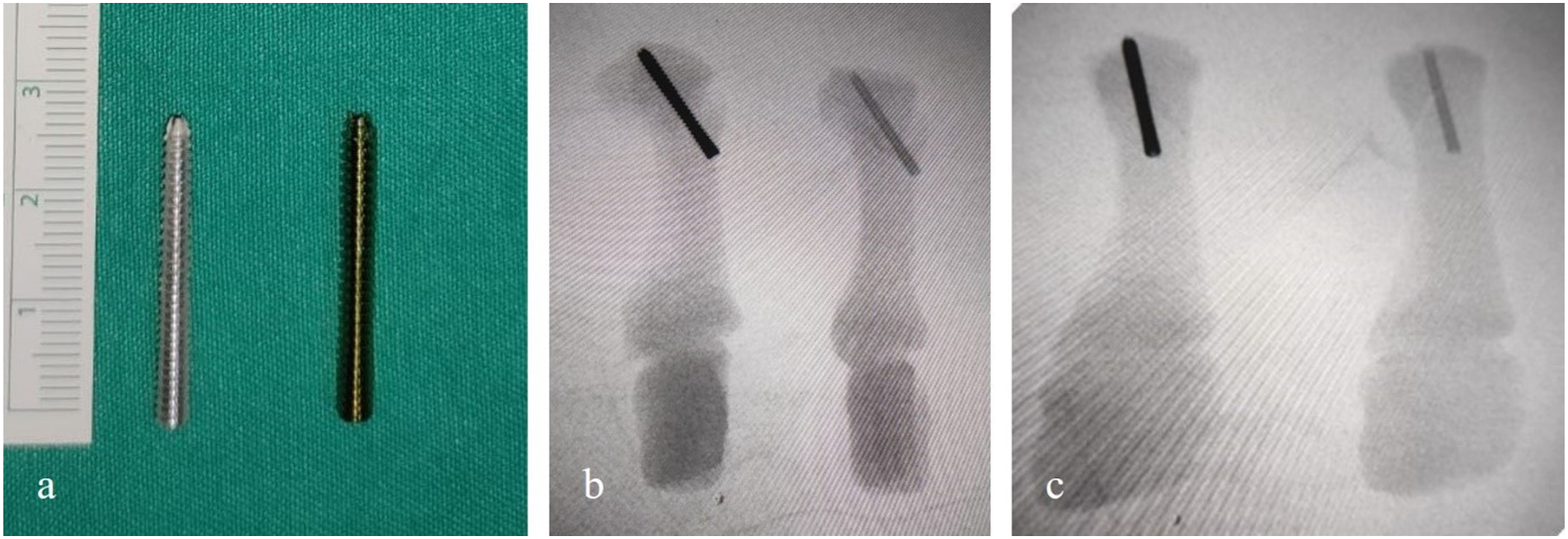
Biomechanical tests
Cantilever and physiological loading methods described by Favre et al
18
were applied to the Group-1 and Group-2 specimens. In each group, five specimens were used for cantilever loading (Figure 3), and five were used for physiological loading (Figure 4). Cantilever configuration at an angle of 15° to the horizontal line and the first metatarsal axis, and force to the metatarsal head in plantar to dorsal. The force at an angle of 13° to the axis of the first metatarsal in the physiological configuration.

The first metatarsal was placed in the cantilever configuration at an angle of 15° to the horizontal line and the first metatarsal axis. Pressure was applied to the metatarsal head in the direction of the plantar to the dorsal. Regarding the biomechanical evaluation of first metatarsal osteotomies, the cantilever configuration has been shown to function well and be frequently used. 19 This allowed analysis of the ground’s reactive force by simulating the anatomical position of the first metatarsal during standing.
Jacob 20 defined another test that evaluates the forces acting on the first metatarsal since the cantilever configuration is insufficient to evaluate the forces generated by muscle contractions during gait. Estimating the amount of ground reaction and muscle force acting on the first metatarsophalangeal (MTP) joint, he concluded that the force acts at an angle of 13° to the axis of the first metatarsal. Favre et al 18 used the loading test performed with this angle as a physiological configuration.
Cantilever or physiological loading tests of sawbones following osteotomy and fixation were conducted separately. Biomechanical analyses and data were performed using a computer connected to the interface of the electromechanical universal test machine (Figure 5) with a 20 kN tension/compression load cell at a velocity of 2 mm/min (TCS, Test Control Systems, Turkey). The applied preload was 5 N. Implant failure or sawbones fracture were defined as a failure and the loading continued until the failure occurred
21
in cantilever or physiological positions. During testing, data on loading (N), displacement (mm) and stiffness (N/mm) were displayed and recorded. Force and displacement graphics were derived. The stiffness ratio values were calculated from the graphics according to the linear curve from prelude to end of the curve. The slope of the linear curve was taken as the stiffness. The evaluation criteria included maximum load to failure, displacement amount at failure and stiffness parameters. The electromechanical test machine and experimental setup for testing.
Statistical analysis
The IBM® SPSS (Statistical Package for the Social Sciences) V22.0 software was used for the statistical analysis. While evaluating the study data, the conformity of the parameters to the normal distribution was assessed with the Shapiro–Wilk test. The Student’s t-test was used to compare the parameters with normal distribution between the two groups. The Mann–Whitney U test was used to compare the parameters that did not show normal distribution between the two groups. Significance was evaluated at the p < 0.05 level.
Results
Maximum force, maximum displacement and stiffness values of the biomechanical test results of the samples.
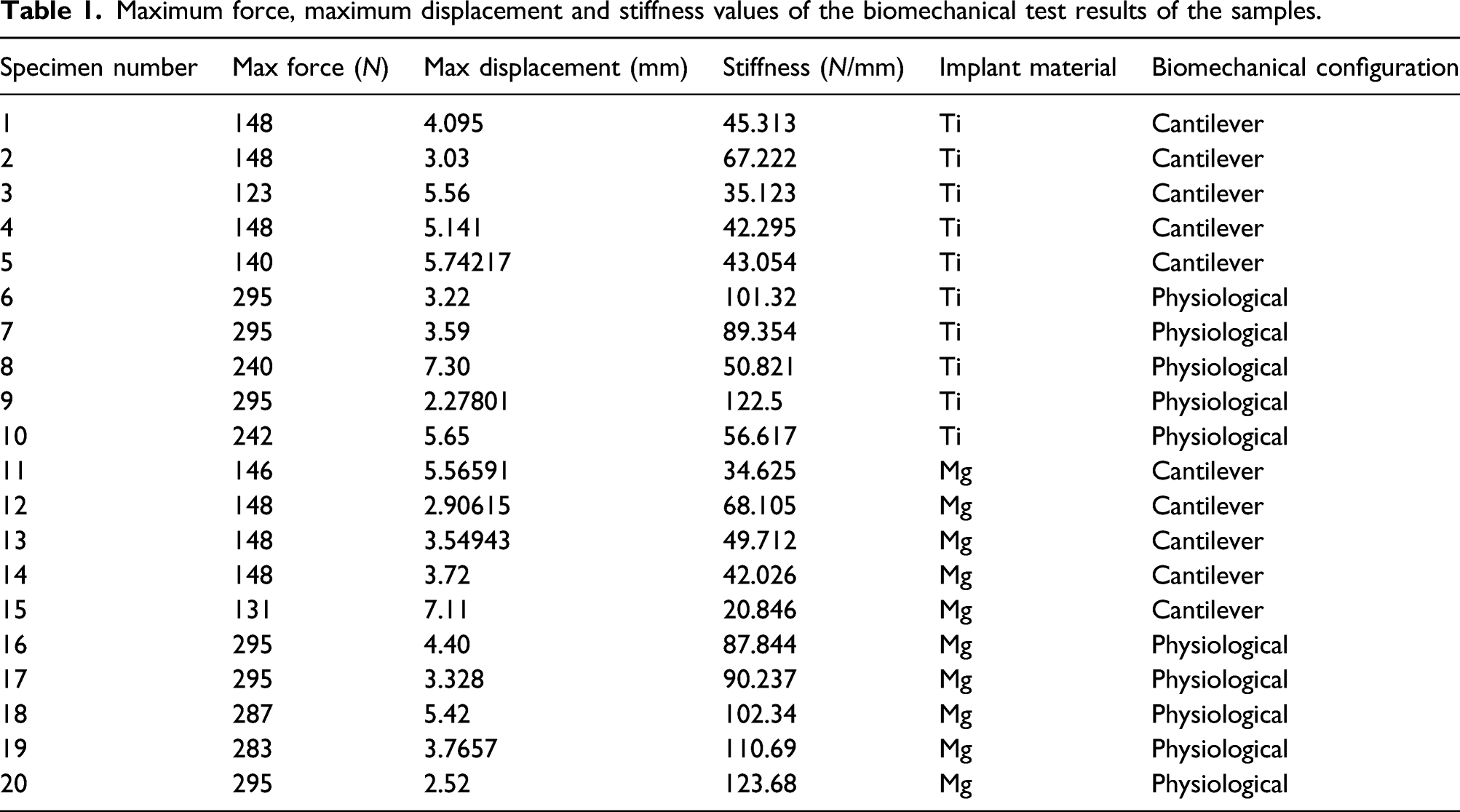
In the physiological configuration, the mean maximum load to failure was 273.4 ± 29.59 N in group-1 (titanium screw) and 291 ± 5.66 N in group-2 (magnesium screw) (p = 0.638); the mean displacement at maximum loading was 4.41 ± 2.03 mm in group-1 and 3.89 ± 1.1 mm in group-2 (p = 0.628); the mean stiffness ratio was 84.12 ± 30.26 N/mm in group-1 and 102.96 ± 14.83 N/mm in group-2 (p = 0.247).
When the mechanical testing performed in the cantilever configuration, the mean maximum load to failure was 141.4 ± 10.85 N in group-1 (titanium screw) and 144.2 ± 7.43 N in group-2 (magnesium screw) (p = 0.814); the mean displacement at maximum loading was 4.71 ± 1.14 mm in group-1 and 4.57 ± 1.73 mm in group-2 (p = 0.881); the mean stiffness ratio was 46.6 ± 12.14 N/mm in group-1 and 43.06 ± 17.59 N/mm in group-2 (p = 0.721).
Statistical evaluation of maximum force, maximum displacement and stiffness measurement values among the materials used separately in biomechanical tests.
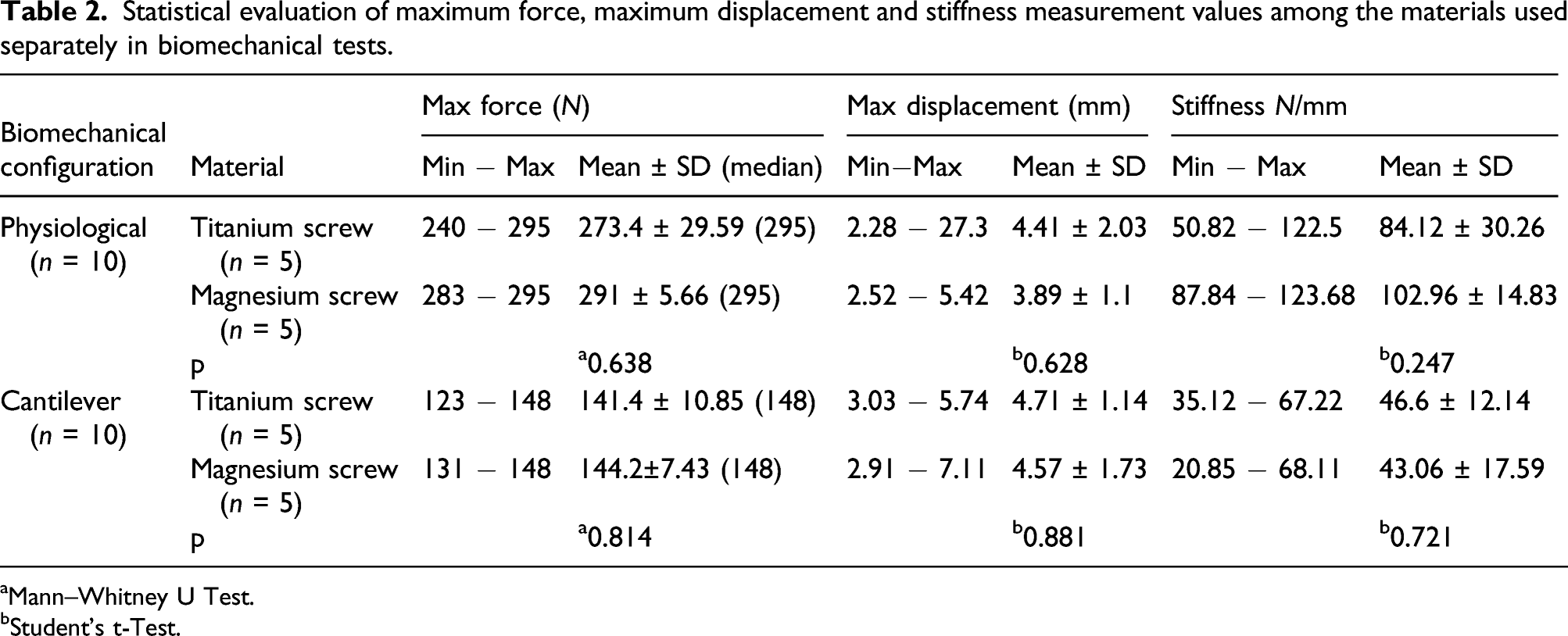
aMann–Whitney U Test.
bStudent’s t-Test.
Discussion
Biomechanical studies have been performed on the shaft and proximal osteotomies in hallux valgus surgery. Studies on distal osteotomies are fewer. There are clinical studies in which osteotomy fixation is performed with magnesium screw in hallux valgus surgery. Windhagen et al 12 used biodegradable magnesium screws for internal fixation on 12 patients who underwent first metatarsal osteotomy; the first clinical results were published in 2013. In contrast, no biomechanical studies have been found in the literature for the fixation of the first metatarsal DCO with magnesium screws. When studies were reviewed for the biomechanical comparison of magnesium and titanium screws, only the study by Ferdinand et al 22 on cadaver capitellum fractures was found. The study found that the headless titanium screw and the magnesium screw provided equal stabilisation. Although the anatomical region and surgical technique are different, our study found no significant stability difference between the magnesium and titanium screws for DCO fixation.
Non-degradable implants, such as titanium or steel, have quite different mechanical properties than cortical bone. As a result, stress transfer is not homogeneous when these implants are used, and bone healing could be adversely affected. This condition is known as “stress shielding.”23,24 Therefore, it may be beneficial to use implants that have similar Young’s modulus to the cortical bone, such as polymer-based or magnesium.
Today, the most widely used degradable implants are polymer-based. Disadvantages are that they are not as mechanically strong as metallic implants and can cause osteolysis and foreign body reactions. 25 Although metallic implants such as titanium are stronger than degradable implants, failure and fractures occur in titanium implants under various conditions.26,27 Degradable magnesium alloys show more promising results in terms of biomechanical strength than polymer-based implants in vivo 28 and in vitro. 29 In a large study comparing magnesium and titanium screws, the failure rate of the magnesium screw was 1%. 30 In comparison, the failure rates of polymer-based implants used in orthopaedic and traumatological indications were as high as 4%. 31
Especially during gait, one of the most important forces acting on the first metatarsal is muscle contractions. Unfortunately, this condition is not considered in most biomechanical studies. The physiological loading configuration introduced by Favre et al 18 was included in our study as a model that simulates the muscle forces acting on the first metatarsal. In this study, the stiffness ratios in the physiological and cantilever configurations were compared between the groups in which fixation with the headless titanium and magnesium screw after DCOs were performed. The ratios were similar in both groups. Similar to Favre et al 18 study, stiffness values in the physiological configuration were higher than cantilever in both groups. Trost et al 19 found similar stiffness rates in the DCOs fixed with a single cortical screw or two K-wire. In contrast, the stiffness ratios were lower in the physiologic configuration than the cantilever in both groups. The discongruity between the findings of Trost et al. and our study might be due to different materials, techniques or cadaveric bones used.
An optimal metatarsal osteotomy should allow performing deformity correction, internal fixation and stabilisation in a reproducible manner without any significant complications. The patient should be able to bear weight immediately after the operation. Some biomechanical studies have investigated the metatarsal osteotomies’ initial stability, in which the possibility of early MTP joint motions and weight-bearing at post-operative has been considered a criterion. 32 During normal gait, the subhallucal load is 25% of body weight at toe-off. Estimation of the minimum hallux load for the 784 N, the average weight of male patients, results in 196 N under the first MTP joint. 33 However, a higher upper limit on the allowable load could assure higher confidence in the outcome. In our study, the maximal force values in the cantilever configuration were lower than 196 N in both groups (Group-1 mean: 141.4 N; Group-2 mean: 144.2 N). The cantilever loading configuration is a well-established test to evaluate the biomechanics of the first metatarsal osteotomies. The fact that the cantilever test results in our study did not achieve the load values affecting the first MTP joint during normal gait shows that osteotomy fixation cannot safely allow early post-operative full weight-bearing. However, based on these values, MTP joint motions and partial weight-bearing may be allowed.
It is essential to consider the failure mode in biomechanical studies in evaluating the stability of surgical techniques. The failure mode of all specimens in this study resulted in distal lateral segment rotation. This failure mode is most common for DCO, as confirmed by the other studies.18,19 Trost et al. compared the fixation of DCO in cadaveric metatarsals with a single 3.5 x 26 mm titanium screw or 1.6 mm two K-wire. The average failure strength was 187.2 N for the single screw group and 258.8 N for the two K-wire group. However, the differences between the groups were not statistically significant. 19 In our study, 2.7 x 26 mm screws were used on the sawbones models, and the failure strength was 141.4 ± 10.85 N for the titanium screws and 144.2 ± 7.43 N for the magnesium screws. The results showed that the failure strength of Trost et al. was higher than our study. The possible reasons for this difference are fixing the osteotomy with larger diameter screws and the difference in strength between the cadaver bone and the sawbones.
Sawbones materials provide many advantages such as size, density and consistency of shape. They are modelable in almost any shape. Additionally, their costs are low, and ethics committee approval or special storage conditions are not required. 34 Heiner 35 found a structural consistency between the stiffness of the synthetic bone models and real bones. Conversely, Quenneville et al 36 found no consistencies in impact testing results between the synthetic and natural bones. Several authors have studied the correlation between bone mineral density (BMD) and biomechanical stability of reconstructive hallux valgus procedures’ fixation techniques. 32 In studies of cadaver bones, standard deviations were high because the BMDs of the specimens were different. However, this situation is more appropriate with clinical reality. Therefore, more relevant data with actual clinics could be achieved by using conserved or fresh cadaver bone material.
A limitation of our study is that although sawbones materials appear to be a better option for performing a standard biomechanical comparison, studies with actual patients or cadaver bones are preferred because they reflect clinical data more accurately.
In conclusion, this study demonstrates no significant differences in maximal load to failure, maximal displacement and stiffness in sawbones that underwent DCO and were fixed with magnesium or titanium screws. Further studies with larger numbers of cadaver bones are needed. The published results of this study may serve as the basis for future biomechanical gait and segmental foot kinematic studies.
Footnotes
Author contributions
AS: Main author of manuscript, Study design.DG: Study design, Data collection and analysis.HB: Data collection and analysis. AA: Data collection and analysis.BK: Study design.IM: Study design, Data collection and analysis.CE: Interpretation of study material, Senior author.All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.