
Abstract
Background:
The Lapidus procedure evolved into the first tarsometatarsal (TMT) arthrodesis, primarily used for treating severe hallux valgus, particularly in TMT arthritis or instability. Although effective, early techniques have high nonunion rates. Recent developments, including locking plate (LP) and intramedullary nail (IN) use, are aimed at enhancing fixation. LPs enable early weightbearing but may cause symptomatic hardware irritation. We hypothesized that IN fixation would yield better clinical and radiologic outcomes and fewer complications than LP fixation. In this retrospective study, we aimed to compare the radiographic and clinical outcomes of IN and LP fixation.
Methods:
Eighty-five patients (120 feet) underwent the modified Lapidus procedure between 2020 and 2023 and were retrospectively grouped according to the fixation type: IN and LP with a crossing screw. Three foot and ankle attending surgeons performed the procedures. Radiographic parameters (hallux valgus angle [HVA], intermetatarsal angle [IMA], and metatarsocuneiform angle [MCA]) were evaluated preoperatively, 2 months after initial weightbearing, and 1 year postoperatively. Clinical outcomes were measured using the Self-Administered Foot Evaluation Questionnaire (SAFE-Q), comprising 5 subscales scored out of 100.
Results:
Among the 64 patients (94 feet) analyzed, 57 and 37 underwent IN and LP fixation, respectively. At 1 year postoperatively, the amount of IMA correction from preoperative to 1 year was similar in both groups, but the IN group showed slightly lower IMA (95% CI: −3.57 to −0.22, P = .0265). HVA correction was similar between the groups; however, there was greater variability in the IN group. MCA changes indicated a comparable degree of correction loss between groups. SAFE-Q scores were statistically similar. The IN group experienced fewer complications (8.8%) compared with the LP group (22%). The LP group revisions mostly involved hardware removal.
Conclusion:
In the modified Lapidus procedure, IN fixation demonstrated a slightly lower IMA at final follow-up and less hardware irritation compared with LP fixation. IN fixation should be considered an alternative to LP fixation.
Level of Evidence:
Level III, retrospective case control study.

Introduction
The Lapidus procedure entails fusion of the first tarsometatarsal (TMT) joint for hallux valgus correction, as initially described by Paul Lapidus in 1934. 1 Originally, the fusion involved the second metatarsal and/or second cuneiform bone. Thereafter, numerous modifications were reported. Consequently, the procedure is now most commonly performed first as an isolated TMT arthrodesis. 2 Despite some controversy regarding the surgical indications, most authors agree that the Lapidus procedure is highly effective for correcting severe hallux valgus deformity associated with an increased intermetatarsal angle (IMA; >14 degrees) and hallux valgus angle (HVA; >30 degrees), especially in cases with concomitant first TMT arthritis or instability.3,4 However, in early reports, the nonunion rate reached 20%, reflecting the limitations of internal fixation devices and surgical techniques at the time. 5 Recently, owing to device advancement, 2 crossed screws or locking plates (LPs) with 1 crossing screw are commonly used. Although LP fixation has demonstrated a trend toward early weightbearing and reduced nonunion rates, complications continue to arise. Symptomatic hardware pain is one such issue that can be both debilitating and costly. These plates are designed to be low-profile and anatomically contoured; however, the thin dorsal soft tissue of the foot and pressure from footwear can easily lead to irritation and prominent hardware pain, often necessitating removal. Therefore, the use of an intramedullary nail (IN) as an alternative implant for fixation has been increasingly recognized in recent reports.6,7 We aimed to compare the radiographic and clinical outcomes of LP vs IN for the modified Lapidus procedure. In addition, we hypothesized that an IN fixation device would demonstrate similar radiographic correction as an LP; however, it would lead to fewer complications, specifically related to reoperation for hardware-related pain.
Methods
Study Population
Between 2020 and 2023, a modified Lapidus procedure for hallux valgus was performed on 85 consecutive patients (120 feet) at our institution. Patients were diagnosed with hallux valgus if the HVA, which is the angle between the proximal phalanx of the hallux and the first metatarsal on weightbearing anteroposterior radiographs of the foot, was ≥20 degrees. The modified Lapidus procedure was indicated in patients with HVA ≥20 degrees and instability of the first TMT joint. The exclusion criteria included cases involving combined surgical procedures beyond the forefoot, such as ankle arthrodesis and correction of progressive collapsing foot deformity (14 feet). In addition, cases in which postoperative foot evaluation was compromised because of spinal surgery for severe spinal disease during the follow-up period were excluded (4 feet). The patients were categorized into 2 groups based on the fixation method used in stabilizing the first TMT fusion site: the IN or dorsomedial LP with 1 crossing screw group.
The surgeries were performed by 3 experienced foot and ankle surgeons, each with >10 years of surgical experience. One surgeon used LP for fixation until March 2021, after which IN was used. The other 2 surgeons performed all procedures using LP.
Adjunctive surgical procedures, including metatarsal shortening osteotomy or TMT joint arthrodesis, were performed for lateral toe lesions in 45 and 30 cases in the IN and LP group, respectively.
The Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was used as the clinical evaluation tool preoperatively and at 1 year postoperatively.8,9 SAFE-Q comprises 5 subscales: “pain and pain-related,” “physical functioning and daily living,” “social functioning,” “shoe-related,” and “general health and well-being.” Each subscale is graded on a 100-point scale, where higher scores indicate better function or less impairment. This tool was specifically developed to assess patient-reported outcomes related to foot and ankle conditions, capturing both the physical and psychosocial aspects of daily life.
The radiographic outcomes included the HVA, IMA (the angles between the first and second metatarsal bone shaft; mean normal value of IMA, 9.93 ± 2.97 degrees 10 ), and MCA (the angles between the first metatarsal bone shaft and the medial cuneiform bone 11 ) measured on anteroposterior views using weightbearing feet radiographs (Figure 1). Radiographic measurements were performed at 3 time points: preoperatively, at 2 months postoperatively (initial weightbearing), and at 1 year postoperatively.
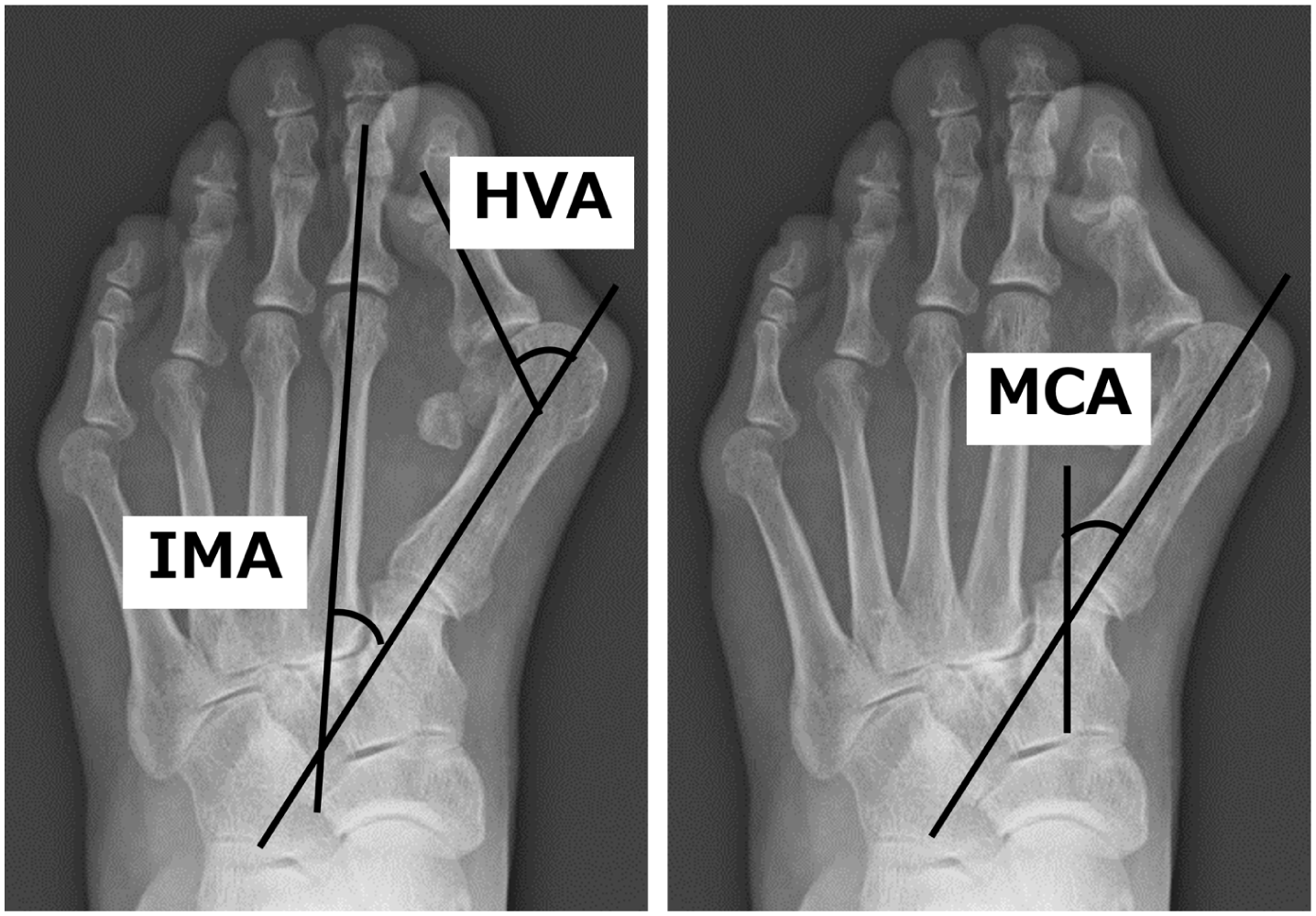
Radiographic values. Each value was evaluated at 3 time points: preoperatively, at 2 months postoperatively (initial weightbearing), and at 1 year postoperatively. HVA, hallux valgus angle; IMA, intermetatarsal angle; MCA, metatarsocuneiform angle.
Surgical Technique
All patients underwent a modified Lapidus procedure involving the use of IN (InCore Lapidus System, Zimmer Biomet, Warsaw, IN) or dorsomedial LP with 1 crossing screw (APTUS Hallux Foot System, Medartis, Basel, Switzerland) (Figure 2).

Postoperative radiographs: (A) intramedullary nail, (B) dorsomedial locking plate with 1 crossing screw.
A medial incision (first skin incision) was made over the first metatarsophalangeal joint to expose the capsule. Subsequently, the medial eminence was removed in line with the metatarsal shaft, starting 1 to 2 mm medial to the sagittal groove.
A second skin incision was made in the first web space. The subcutaneous tissue was dissected until the adductor hallucis tendon, deep transverse metatarsal ligament, and the lateral capsule around the fibular sesamoid were clearly identified. They were cut sharply enough to allow the hallux to be corrected to approximately 10 degrees varus and the sesamoid to be repositioned beneath the first metatarsal head.
A third skin incision was made dorsal to the first TMT joint, which was corrected by performing a closed wedge osteotomy. Exposure was limited to the insertion site for the nail on the medial cuneiform and the 2 lag screws on the first metatarsal bone in the IN group. In the LP group, careful additional soft tissue dissection was performed to minimize invasion, particularly to the tibialis anterior tendon and surrounding structures, for placement of the dorsomedial plate. The first TMT joint was fixed with the IN or dorsomedial LP with 1 crossing screw (Figure 3). Lag screws were placed via the first or second skin incision, and an intramedullary nail was inserted through the third skin incision. LP and crossing screw were inserted through the third skin incision.

Intraoperative photographs by type of internal fixation (a) medial skin incision (A); (b) skin incision for lateral soft tissue release (B) and arthrodesis (C); (c) Intramedullary nail; and (d) dorsomedial locking plate with 1 crossing screw.
Postoperative management involved applying a bulky dressing using bandages for 6 weeks to primarily protect the surgical site and facilitate soft tissue correction. Patients were instructed to walk with a heel gait during this period. Full weightbearing on the forefoot was permitted after removal of the bulky dressing, approximately 2 months postsurgery.
Statistical Analysis
The sample size used in this study was smaller than that required to compare means between the 2 groups, with a power of 0.80 and an alpha error of 0.05. Homogeneity of variances was assessed using F test following confirmation of normality of the continuous variables (eg, HVA, IMA, age, SAFE-Q score) using the Shapiro-Wilk test. Student t test was applied when variances were equal; otherwise, Welch t test (preoperative IMA, follow-up period, preoperative physical functioning and social functioning, postoperative physical functioning, social functioning, and general health) was used.
Regarding the presence or absence of hardware removal, Fisher exact test was applied because of the presence of cells with expected frequencies ≤5.
Receiver operating characteristic curve analysis was performed to evaluate the predictive value of IMA for hallux valgus recurrence and hallux varus onset. The sensitivity and specificity were calculated using the receiver operating characteristic curve, and the optimal cut-off value was determined using the Youden index. All analyses were performed using IBM SPSS (version 26.0; IBM Corp, Armonk, NY), and statistical significance was set at P <.05.
Results
Overall, 64 patients (94 feet) were included in the study: 40 (57 feet) in the IN group and 24 (37 feet) in the LP group (Figure 4). The patient demographics are presented in Table 1. The average age at the time of surgery was significantly higher in the IN group (73.0 years) than in the LP group (69.9 years) (P = .0495).

Flow diagram of participant selection.
Patient Demographics.

Abbreviations: IN, intramedullary; LP, locking plate.
The radiographic evaluations before and after surgery are presented in Table 2. No significant preoperative difference in deformity severity was observed between groups. Compared with the LP group, the IMA at 1 year postoperatively was significantly lower in the IN group. No significant difference was observed in the average HVA at 1 year postoperatively between the 2 groups (P = .0422). The mean HVA was 9.85 ± 11.5 degrees (range: −25 to 38) in the IN group and 14.1 ± 8.30 degrees (range: −3 to 44) in the LP group. Hallux varus, defined as an HVA <0 degrees at 1 year postoperatively, was observed in 6 feet (11%) in the IN group and 1 foot (2.7%) in the LP group. The cut-off value of the IMA for the hallux varus was 2 degrees in the IN group (Figure 5). Recurrence was defined as an HVA >20 degrees at 1 year postoperatively and was observed in 11 and 7 cases (19 and 19%) in the IN and LP groups, respectively. The IMA was analyzed in the IN and LP groups, and the recurrence cutoff values were 10 degrees and 11 degrees for the IN and LP groups, respectively (Figure 6).
Radiographic Evaluations Before and After Surgery.
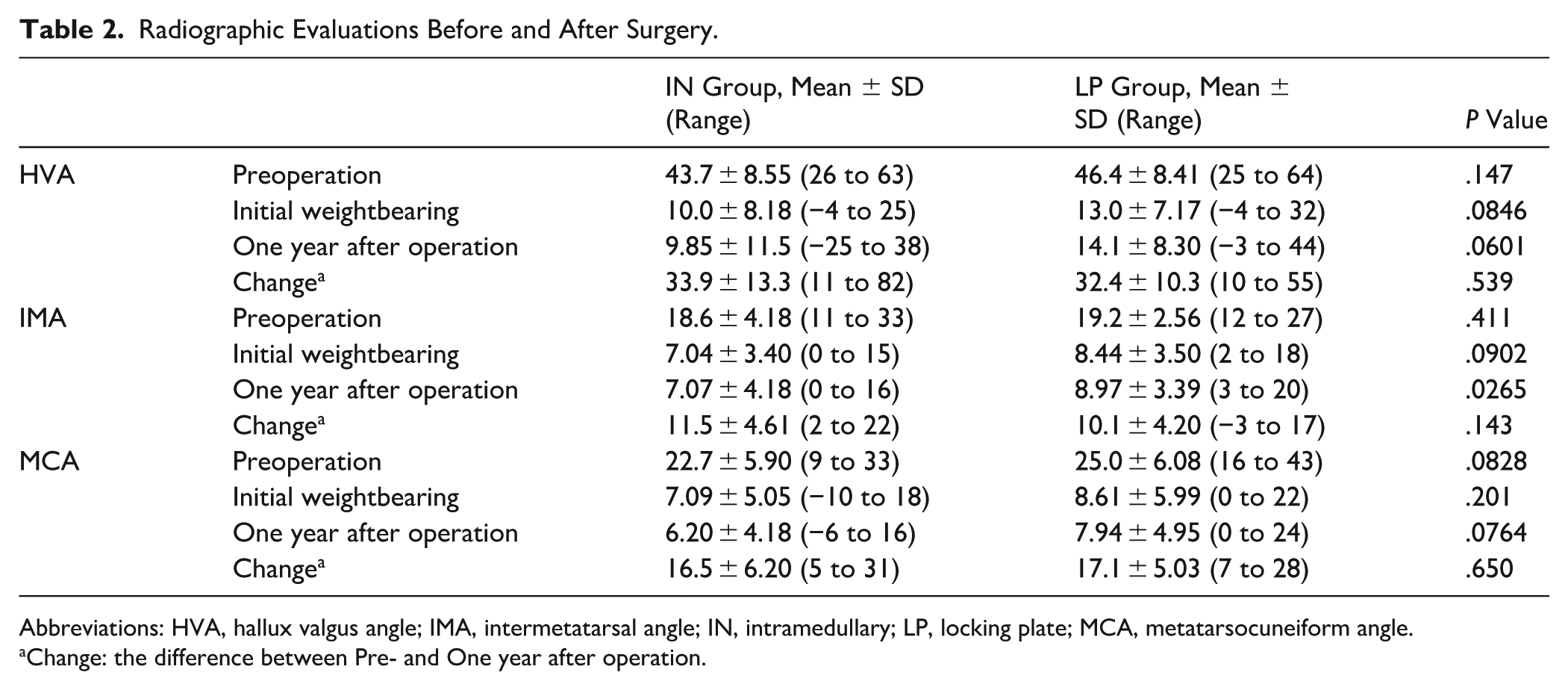
Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; IN, intramedullary; LP, locking plate; MCA, metatarsocuneiform angle.
Change: the difference between Pre- and One year after operation.

Receiver operating characteristic curve analysis of the intermetatarsal angle (IMA) in the IN group for predicting postoperative hallux varus. The optimal cutoff value of IMA was 2 degrees, with corresponding sensitivity and specificity shown in the figure. IN, intramedullary.
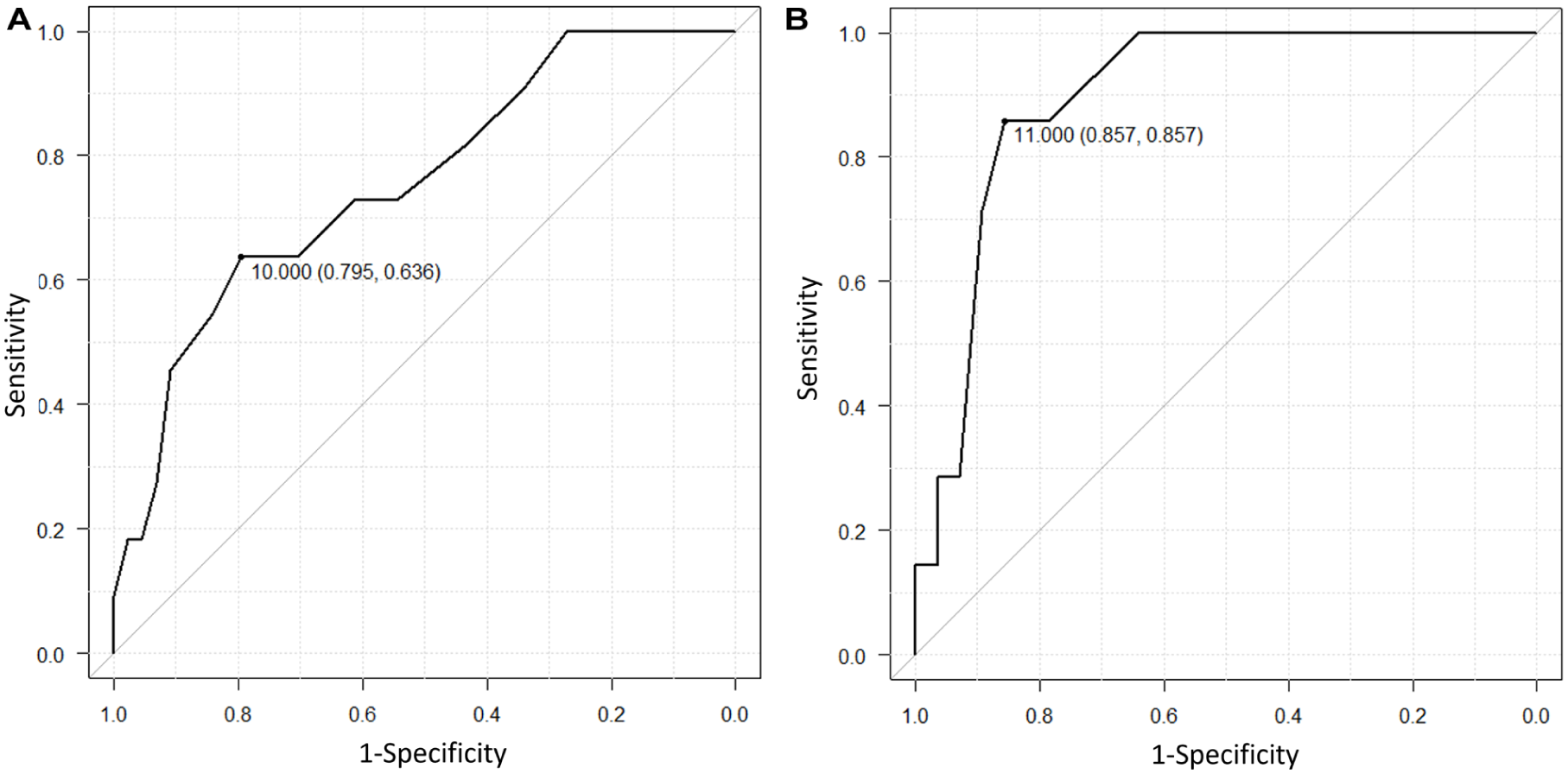
Receiver operating characteristic curve analysis of the intermetatarsal angle (IMA) for predicting recurrence of hallux valgus after Lapidus procedure. (A) IN group, (B) LP group. IN, intramedullary; LP, locking plate.
The difference in the MCA between the initial weightbearing phase and at 1 year postoperatively, measured in each case, was 2.87 ± 2.50 degrees (range: 0-9) in the IN group and 3.09 ± 2.58 degrees (range: 0-10) in the LP group, indicating a correction loss. The F test showed no significant difference in variance between the groups (P = .812); therefore, Student t test was applied for comparison. The difference in MCA between the groups was statistically insignificant (P = .694).
The clinical outcomes based on SAFE-Q are presented in Table 3. At 1 year postoperatively in the IN group, all subscales showed significant improvement. In contrast, the LP group demonstrated significant improvement in the “pain and pain-related,” “shoe-related,” and “general health and well-being” subscales. The mean preoperative social functioning score was significantly lower in the IN group than in the LP group. No significant differences were observed in the IN and LP groups in any of the 1-year postoperative subscales.
Clinical Outcomes Based on SAFE-Q.

Abbreviations: IN, intramedullary; LP, locking plate; SAFE-Q, Self-Administered Foot Evaluation Questionnaire.
Complications
In the IN group, complications were observed in 5 cases (8.8%), and revision surgery was performed in 2 cases (3.5%). In 1 case, an intraoperative metatarsal fracture occurred at the insertion site of the lag screw, necessitating a change in the fixation method to LP. In another case, nerve injury at the lag screw insertion site resulted in postoperative sensory impairment. One patient inadvertently applied full weightbearing to the forefoot immediately after surgery, resulting in a cuneiform fracture at the nail insertion site. Although loss of correction was observed, bone union was achieved with conservative management, and reoperation was not required.
Revision surgery was performed in 1 case of nonunion and 1 case of recurrent deformity.
In the LP group, complications were observed in 8 cases (22%), and revision surgery was performed in all the cases. The reasons for the revision surgery included hardware removal due to irritation from the locking plate in 7 cases and nonunion in 1 case. Fisher exact test revealed a significantly lower incidence in the IN group despite hardware removal (P < .01).
Discussion
In this study, we evaluated the clinical and radiographic outcomes of IN fixation in comparison with LP fixation for the modified Lapidus procedure. At 1 year postoperatively, the IMA was slightly lower in the IN group, whereas SAFE-Q did not differ significantly between both groups. Notably, no cases of hardware removal were observed in the IN group, indicating that IN fixation may be associated with reduced soft tissue irritation relative to LP fixation. IN has been increasingly employed with the expectation of reduced surgical invasiveness in the soft tissue. Recent reports have suggested improved clinical outcomes with IN fixation; however, the available evidence remains limited. To our knowledge, this is the first study to directly compare the clinical and radiographic outcomes of IN vs LP fixation with regard to the modified Lapidus procedure.
In this study, we compared the 1-year postoperative outcomes of the modified Lapidus procedure using different fixation constructs (IN and LP). Radiographic assessment revealed a significantly lower IMA in the IN group. There was no significant difference in the amount of IMA correction—defined as the change between preoperative and 1-year postoperative values—between the 2 groups. Although no significant difference was found in the HVA between the 2 groups, the F test analysis revealed a significant difference in variance, with the LP group showing a smaller standard deviation. This suggests that the outcomes were more consistent with those of LP. Regarding the MCA, no significant differences were observed between the groups at any time point: preoperatively, at initial weightbearing, or 1 year postoperatively. Furthermore, both groups demonstrated no significant changes in the MCA postoperatively, indicating the absence of substantial correction loss over time. The postoperative clinical outcomes, assessed using SAFE-Q, showed no statistically significant differences between the 2 groups. Regarding the observed variance in HVA between the 2 groups, the learning curve for the Lapidus procedure reportedly involves approximately 23 cases. 12 In our study, all 3 surgeons had experience exceeding this threshold, indicating that the increased variance in the IN group may be attributable to limited familiarity with the IN device rather than surgical proficiency. Nonetheless, this variance did not result in a statistically significant difference in the HVA between the groups.
Regarding complications, the nonunion rate in previous studies was 6% to 12%.13 -15 Coetzee reported that all the cases occurred in smokers. In that study, fixation was performed using a single screw across the first TMT joint and an additional intermetatarsal screw between the first and second metatarsals. 16
A cadaveric study comparing the fixation strength of various internal fixation constructs (the 4-hole IN, 3-hole IN, medial LP with crossing screw, and crossing screws) demonstrated that locked IN and medial LP with crossing screws resisted plantar gapping more effectively than 2 crossing screws. 6 These findings suggest that locked IN and medial LP with crossing screws may promote superior bone healing and better tolerate early weightbearing when compared with 2 crossing screws. In our study, nonunion occurred in only 1 patient in the IN group (1.8%) and 1 patient in the LP group (2.7%), indicating favorable outcomes when compared with previously reported rates.
Regarding complications, hallux varus was defined as a postoperative HVA <0 degrees, which was observed in 6 feet (11%) in the IN group and 1 foot (2.7%) in the LP group. However, none of these patients required revision surgery. Previous reports have indicated a hallux varus incidence of approximately 16%, 17 with postoperative IMA <5 degrees identified as a risk factor. 18 In our study, a postoperative IMA <2 degrees appeared to be a risk factor in the IN group.
Postoperative recurrence rates of hallux valgus were reportedly from 3% to 73%, with few studies distinguishing between symptomatic and asymptomatic cases. Failure to reduce the IMA to <10 degrees has been identified as a risk factor for the recurrence of hallux valgus deformity. 19
In our study, radiographic recurrence was defined as HVA ≥20 degrees and was observed in 11 and 7 cases (19% and 19%) in the IN and LP group, respectively. One patient in the IN group required revision surgery. This suggested that most patients maintained satisfactory clinical outcomes despite radiographic recurrence. These findings align with the perception that radiographic changes do not necessarily correlate with poor clinical outcomes following scarf osteotomy. 20 Postoperative IMA of 10 degrees or greater in the IN group and 11 degrees or greater in the LP group were identified as risk factors for recurrence.
Although LP with crossing screws provides robust fixation, their placement requires extensive soft tissue dissection. Hardware prominence, despite its association with dorsal plating or screw fixation, can cause patient discomfort, particularly under the thinner and more vulnerable dorsal skin. 21 A previous study documented a hardware removal rate of 17% (15 plates), occurring at an average of 22.5 months postoperatively, because of symptomatic plate prominence. 22
In our study, hardware removal was required in 7 cases (19%) in the LP group following bone union. In contrast, IN is a low-prominence implant, which may mitigate the pain related to hardware protrusion in conventional plating systems. 23 In our study, no cases in the IN group required hardware removal because of soft tissue irritation.
This study had some limitations. First, the relatively short follow-up period should be acknowledged, and continued long-term monitoring is necessary. However, appropriate correction of the IMA is essential to prevent complications such as hallux valgus recurrence and hallux varus development. In our study, bone fusion was observed in most patients during the follow-up period, suggesting that the risk of correction loss was minimal. Nevertheless, this interpretation should be made with caution and validated by future studies with a long-term follow-up period.
Second, among the 3 participating surgeons, only 1 used IN fixation. Consequently, possible surgeon-related bias cannot be entirely excluded. Nonetheless, all surgeons were foot and ankle surgeons with more than a decade of surgical experience, and the influence of individual surgeon variability on clinical outcomes was minimal.
Third, this study was underpowered to detect statistically significant differences between the 2 groups, as the sample size was smaller than that required for a power of 0.80 and an alpha error of 0.05.
Fourth and notably, the patient backgrounds were not completely matched between the groups. As described in the methods section, there was no selection bias; however, the mean preoperative age in the IN group was significantly older (P = .0495). This may have contributed to the significantly lower mean preoperative social functioning score observed in the IN group compared with the LP group. The details of comorbidities, such as diabetes mellitus, were not evaluated. These factors may have influenced the baseline functional status and should be considered when interpreting the results. Nevertheless, we believe that our findings are clinically relevant because, to our knowledge, no previous studies have directly compared the clinical outcomes of IN and LP fixation in this context.
Conclusion
In this study, we compared a novel fixation method, IN, with LP in the modified Lapidus procedure for hallux valgus correction. One year postoperatively, IMA was slightly lower in the IN group, although the preoperative to 1-year IMA change was similar between groups. The postoperative outcomes assessed using the SAFE-Q showed no significant differences between the 2 groups. Hardware removal was not required in the IN group, suggesting that IN fixation may cause less soft tissue irritation than LP fixation. These results must be cautiously interpreted because of the small sample size and limited follow-up.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251393647 – Supplemental material for Radiographic and Clinical Outcomes of Intramedullary Nails in the Modified Lapidus Procedure: A Retrospective Comparison with Dorsomedial Locking Plates
Supplemental material, sj-pdf-1-fao-10.1177_24730114251393647 for Radiographic and Clinical Outcomes of Intramedullary Nails in the Modified Lapidus Procedure: A Retrospective Comparison with Dorsomedial Locking Plates by Hiroaki Kurokawa, Akira Taniguchi, Toru Ota, Norihiro Tsujimoto, China Teraoka, Yoshiyuki Kamatani, Yinghao Li, Nan Mei, Yuki Ueno, Shuichiro Ueda, Takuma Miyamoto, Katsuya Nishikawa, Mayumi Yasuda and Yasuhito Tanaka in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
This study was approved by the local institutional review board (research number: 4036).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.