
Abstract
Background:
Degenerative changes at the sesamoid-metatarsal joints (SMJs) may be a source of pain following hallux valgus surgery. The aims of this study were to describe degenerative changes at the SMJs on weightbearing computed tomography (WBCT) scans and, secondarily, investigate their association with 1-year patient-reported outcome scores following a modified Lapidus procedure for hallux valgus. We hypothesized that reduced joint space in the SMJs would correlate with worse patient-reported outcomes.
Methods:
Fifty-seven hallux valgus patients who underwent a modified Lapidus procedure had preoperative and minimum 5-month postoperative WBCT scans, and preoperative and at least 1-year postoperative PROMIS physical function (PF), pain interference, and pain intensity scores were included. Degenerative changes at the SMJs were measured using distance mapping between the sesamoids and first metatarsal head on preoperative and postoperative WBCT scans. The minimum and average distances between the first metatarsal head and tibial sesamoid (tibial-SMJ) for each patient preoperatively and postoperatively were measured. Sesamoid station was measured on WBCT scans using a 0 to 3 grading system. Linear regression was used to investigate the correlations between minimum preoperative and postoperative tibial-SMJ distances and 1-year postoperative PROMIS scores.
Results:
The median minimum and average tibial-SMJ distances increased from 0.82 mm (interquartile range [IQR] 0.40-1.03 mm) and 1.62 mm (IQR 1.37-1.75 mm) preoperative to 1.09 mm (IQR 0.96-1.23 mm) and 1.73 mm (IQR 1.60-1.91 mm) postoperative (P < .001 and P < .001), respectively. In a subset of patients with complete sesamoid reduction, we found an association between preoperative minimum tibial-SMJ distance and 1-year postoperative PROMIS PF scores (coefficient 7.2, P = .02).
Conclusion:
Following the modified Lapidus procedure, there was a statistically significant increase in the tibial-SMJ distance. Additionally, in patients with reduced sesamoids postoperatively, reduced preoperative tibial-SMJ distance correlated with worse PROMIS PF scores.
Level of Evidence:
Level IV, case series.
Introduction
Hallux valgus is a 3-dimensional deformity characterized by a valgus deformity of the hallux and varus deformity of the first metatarsal, 23 with more recent work demonstrating pronation of the first metatarsal and hallux. 4 Hallux valgus has an estimated prevalence of 23%, 1 and despite advancements in surgical interventions, up to one-third of patients continue to experience postoperative pain following hallux valgus surgery. 4 The subluxation of the first metatarsal in hallux valgus results in the change in the position of the sesamoids relative to the first metatarsal, away from their normal position in their cartilaginous grooves under the plantar surface of the distal first metatarsal.6,10 This translocation may lead to the erosion of the intersesamoid ridge and the development of arthritic changes within the sesamoid-metatarsal joints (SMJs). 15 Lateral translation of the tibial sesamoid has been associated with worsening of the hallux valgus deformity as well as with more severe degenerative changes at the SMJs, suggesting an intricate interplay between the triplanar deformity of the first metatarsal and sesamoid complex. 15 Osteoarthritis affecting the sesamoid-metatarsal joints (SMJs) occurs in a considerable number of patients with hallux valgus, with the incidence rate ranging from 32% to 81%. 23
Although osteoarthritis is known to cause severe pain and disability in other joints, 31 the role that SMJ degeneration in hallux valgus plays in preoperative symptoms and postoperative outcomes is unclear. 15 Although degenerative changes under the first metatarsal head are recognized to coincide with developing hallux valgus, 15 the direct relationship between the degree of degeneration and severity of the hallux valgus deformity remains uncertain. A previous study demonstrated that increased sesamoid subluxation was associated with decreased volume of the intersesamoidal ridge (crista), but degenerative changes between the first metatarsal head and sesamoids were not quantified. 6 Additionally, there is an intricate interplay between the triplanar deformity of the first metatarsal and the sesamoid complex. 10 Previous studies have demonstrated that appropriate reduction of the sesamoids decreases the recurrence rate of hallux valgus following surgical intervention.5,24 Moreover, there are studies that have shown improvement in patient satisfaction scores following corrective surgery. 10 However, it is yet unknown whether the degree of erosion directly impacts patient-reported outcomes following corrective surgery.
Therefore, the primary aim of this study was to quantify preoperative and postoperative degenerative changes at the SMJs in patients undergoing surgical intervention for hallux valgus. A secondary aim was to investigate if there was an association between preoperative degenerative changes at the SMJs and postoperative patient-reported outcomes. We hypothesized that postoperative reduction of the sesamoids would increase the distance between the sesamoids and the first metatarsal head as sesamoids are relocated beneath the more normal cartilage in their grooves under the first metatarsal head. We also hypothesized that worse degenerative changes at the SMJs preoperatively would be associated with worse patient-reported outcomes at 1 year postoperatively.
Methods
Inclusion and Exclusion Criteria
Data for this study were obtained from an institutional review board–approved orthopaedic foot and ankle registry, which includes office and operative notes, imaging studies, and patient-reported outcome measurements. Patients were eligible to be included in this study if they were diagnosed with hallux valgus, underwent a modified Lapidus procedure between January 2016 and April 2022 8 had preoperative Patient-Reported Outcomes Measurement Information System (PROMIS) physical function, pain interference, and pain intensity scores, and preoperative weightbearing CT (WBCT) scans. Patients were excluded if they did not have greater than or equal to 1-year PROMIS physical function, pain interference, or pain intensity scores and a minimum 5-month postoperative WBCT scan. Five months was determined to be the earliest follow-up time point for postoperative WBCT scans as patients are fully weightbearing at this time, and this follow-up period has been used as the minimum follow-up in other studies.9,10 As a result, there were 57 patients who met inclusion criteria (52 females, 5 males), and the median age of the patients at the time of surgery was 54 years (IQR 48-59 years) (Figure 1).
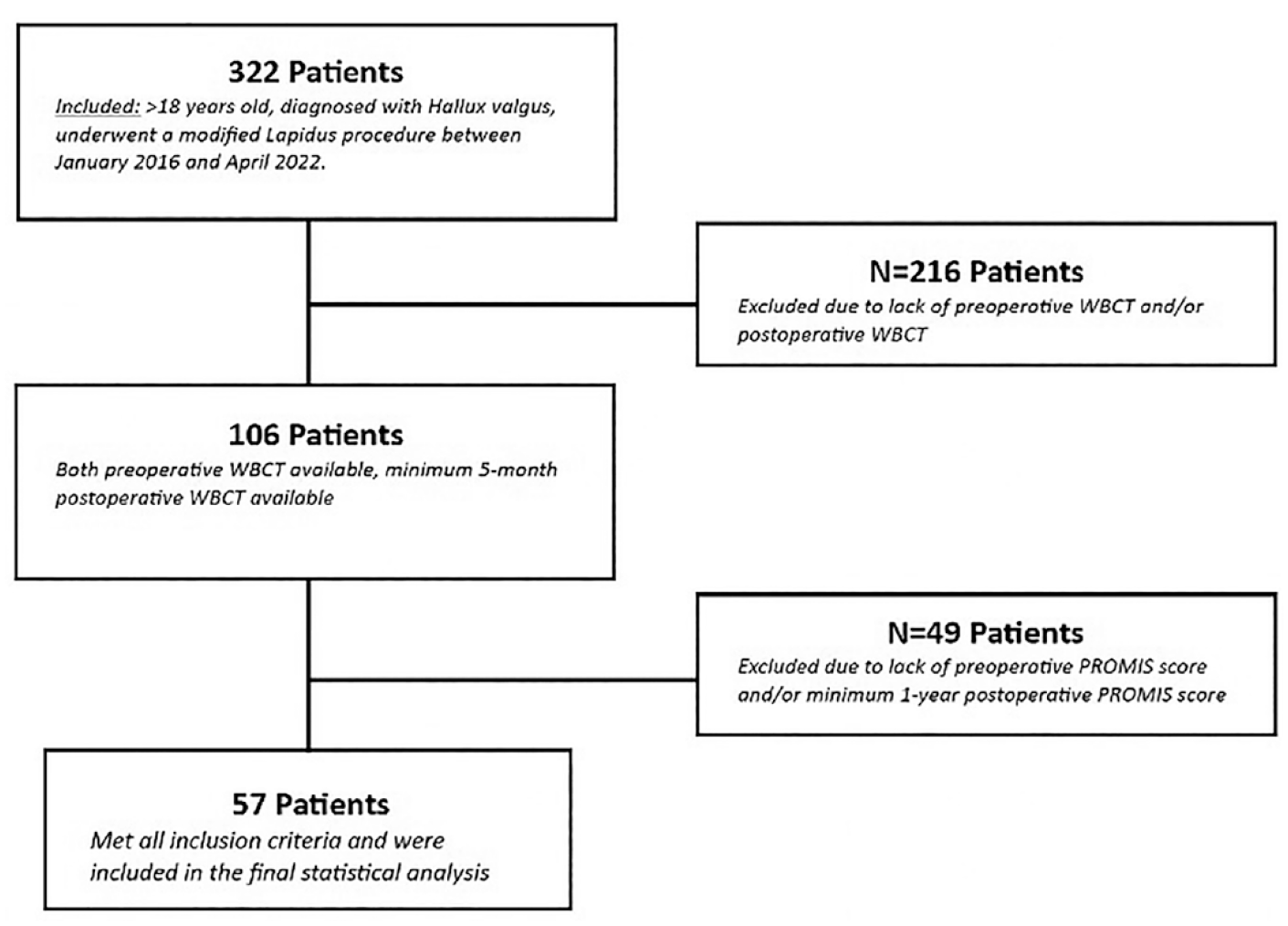
Inclusion and exclusion criteria. (PROMIS, Patient-Reported Outcomes Measurement Information System; WBCT, weightbearing computed tomography.)
Distance Mapping
Participant preoperative and postoperative WBCT scans were used to develop corresponding sesamoid distance maps. The WBCT scans were first uploaded into validated commercial software used to segment the individual bones with excellent reliability from the image files (Bonelogic; Disior Oy, Helsinki, Finland).12,18,21 The automated segmentations of individual bones were checked to ensure that the bones were accurately identified. The segmentations of the first metatarsal and sesamoids were then imported into commercial reverse engineering software to calculate the distance measurements (Geomagic Design X; 3D Systems, Rock Hill, SC). The distances were calculated along the normal surface vectors of the superior surface of the tibial and fibular sesamoids with the inferior surface of the first metatarsal head. Distance maps were then created from all individual distance measurements (Figure 2). The distance maps were colored to highlight regions with normal distances up to 2 mm because a previous study has shown that the upper limit of the combined cartilage thickness of the metatarsal head and sesamoid is approximately 2 mm.1 This was necessary as the fibular sesamoid was often subluxated preoperatively, leading to regions with large distances between the sesamoid and metatarsal head, which did not accurately represent the remaining cartilage present. The minimum and average distances were calculated between both sesamoids and the first metatarsal head. The minimum distance was used for the correlation analysis with patient-reported outcomes data as the irregular contour of the metatarsal head provided greater variability in the average distance measurement compared to the minimum distance. 30
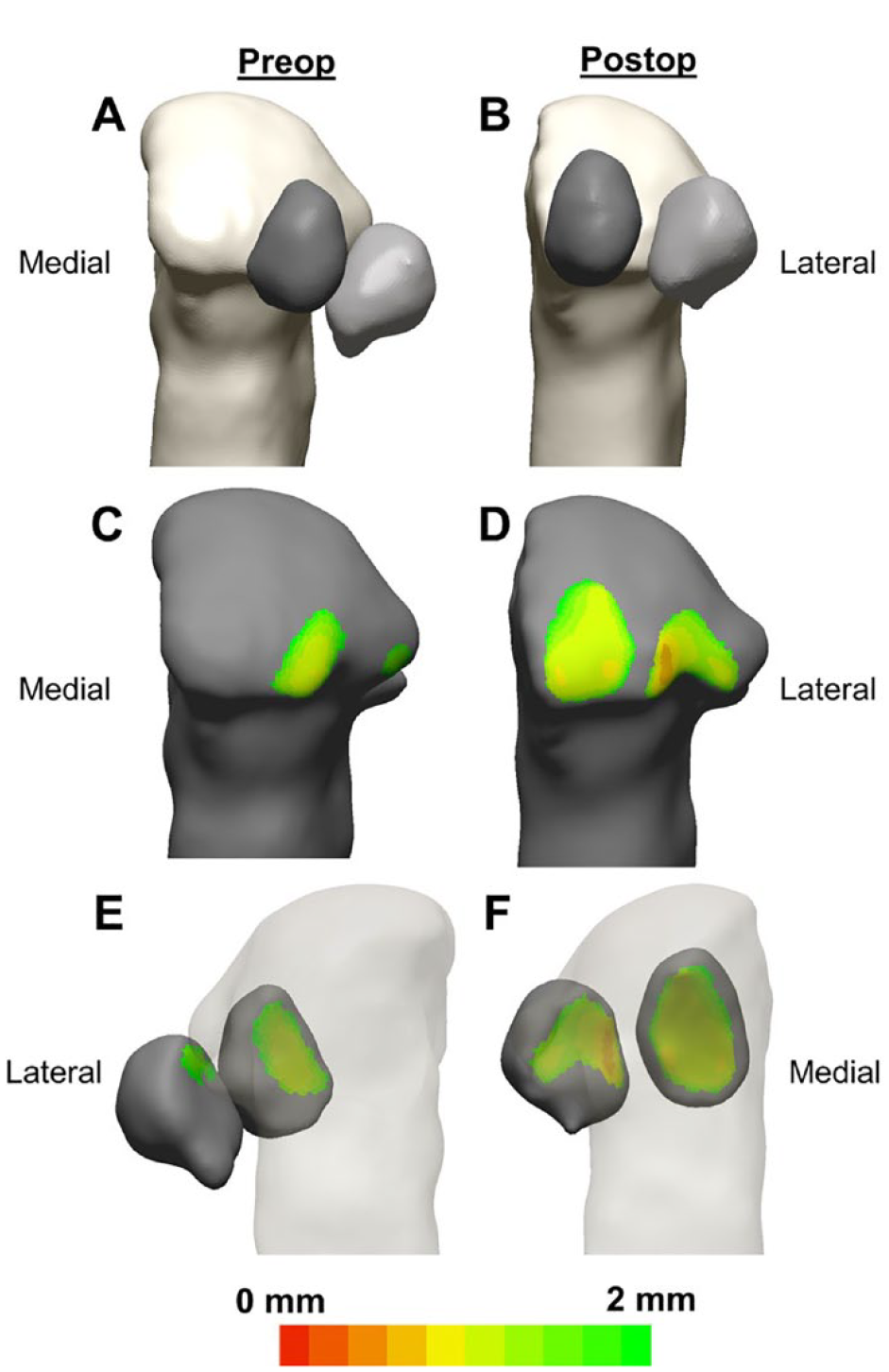
Plantar view of the 3D segmentation example of a patient’s first metatarsal and tibial and fibular sesamoids in the (A) preoperative and (B) postoperative conditions. Plantar view of the joint distance maps superimposed on the metatarsal for the (C) preoperative and (D) postoperative conditions. Dorsal view of the distance maps on the sesamoids for the (E) preoperative and (F) postoperative conditions. Distance maps are colored to highlight regions with normal distances up to 2 mm.
Following the distance mapping, the sesamoid positions were scored on a 4-stage grading system previously reported by Kim et al. 16 The 4-stage grading system was used according to the position of the tibial sesamoid relative to the intersesamoid ridge. The coronal axis of the WBCT scan, perpendicular to the third metatarsal, was then used to grade sesamoid subluxation. A grade of 0 indicated that the tibial sesamoid was entirely medial to the intersesamoid ridge, a grade of 1 indicated that less than half the width of the tibial sesamoid was subluxated laterally, a grade of 2 indicated that more than half the width of the tibial sesamoid was subluxated laterally, and a grade of 3 indicated that the tibial sesamoid was entirely lateral to the intersesamoid ridge.
Statistical Analysis
Because of the small sample size, descriptive statistics were reported as median and interquartile range for continuous variables and frequency and proportion for categorical variables. To control for potential postoperative sesamoid subluxation as a confounding factor, a subgroup of patients with a postoperative sesamoid subluxation of grade 0, which indicates reduced sesamoids, was defined and used for the patient-reported outcomes analysis. Among patients with no postoperative sesamoid subluxation, the correlation between the minimum distance of the tibial sesamoid and first metatarsal head distances at preoperative and postoperative and 1-year postoperative PROMIS domains were assessed using multivariable linear regression models after adjusting for postoperative tibial sesamoid joint distance and preoperative PROMIS scores. Additionally, because 1-year PROMIS scores were obtained after postoperative tibial SMJ was measured on 5-month postoperative WBCT scans, postoperative distances at the SMJ were also controlled. Partial plots from the models were plotted for the preoperative distance radiographic variables controlled for the median postoperative distance radiographic variable and median preoperative PROMIS score. Analyses were conducted using R (R Core Team Vienna VA 2023) with the rms package. 27
Results
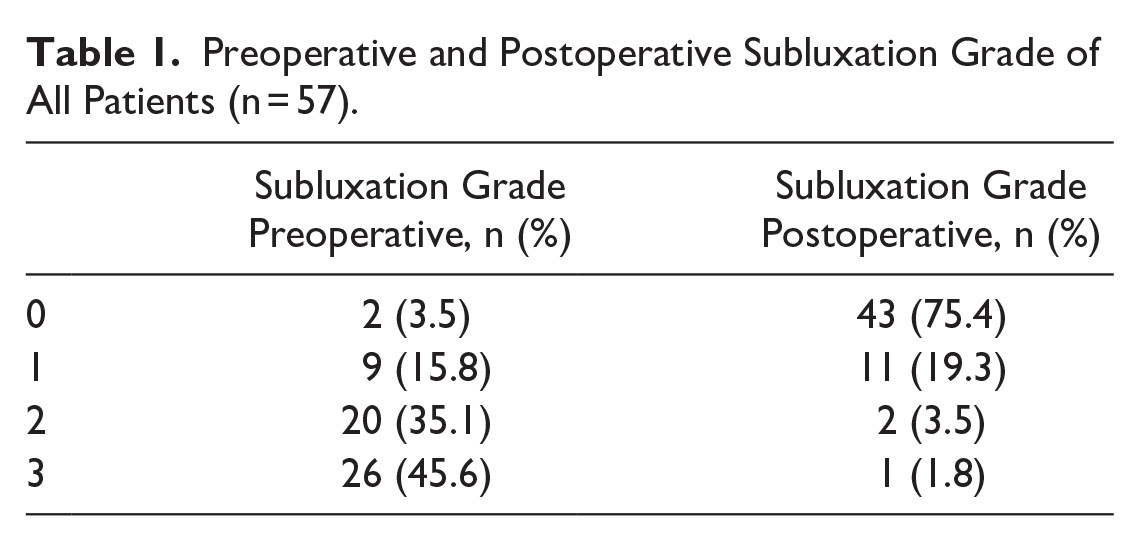
Preoperatively, 55 of 57 patients (96.5%) had a tibial sesamoid station of greater than 0, whereas, postoperatively, 43 of 57 patients (75.4%) had a reduction of the sesamoids and a sesamoid station of 0 (Table 1).
Preoperative and Postoperative Subluxation Grade of All Patients (n = 57).
Comparison of Preoperative and Postoperative Tibial and Fibular Sesamoid-Metatarsal Joint Distance
Preoperatively, the median minimum and average distances from the tibial-SMJ were 0.82 mm (IQR 0.40-1.03 mm) and 1.62 mm (IQR 1.37-1.75 mm), respectively. Postoperatively, the median minimum and average tibial-SMJ distances increased to 1.09 mm (IQR 0.96-1.23 mm) and 1.73 mm (IQR 1.60-1.91 mm), respectively, which demonstrated statistically significant increases from the preoperative measurements (P < .001, P < .001). The range of preoperative to postoperative changes for the minimum and average tibial-SMJ distances were −0.74 to 1.76 mm and −0.62 to 1.35 mm, respectively.
Additionally, the median minimum and average distances of the fibular-SMJ preoperatively were 0.99 mm (IQR 0.84-1.16 mm) and 1.61 mm (IQR 1.47-1.80 mm), respectively. Postoperatively, the median minimum and average fibular sesamoid distances did not significantly change and were 0.99 mm (IQR 0.86-1.17 mm, P = .353) and 1.56 mm (IQR 1.42-1.73 mm, P = .144), respectively. The range of preoperative to postoperative changes for the minimum and average fibular-SMJ distances measurements were −2.27 to 1.79 mm and −1.57 to 1.44 mm, respectively.
Increasing sesamoid station was not associated with lower preoperative tibial- and fibular-SMJ minimum or average distances (all P values > .40). Preoperative minimum tibial-SMJ and fibular-SMJ distances were not significantly correlated with postoperative tibial and fibular SMJ minimum distances (ρ = 0.17, P = .22, and ρ = 0.23, P = .092, respectively). However, preoperative and postoperative minimum tibial-SMJ distances were correlated with preoperative and postoperative minimum fibular-SMJ distances (ρ = 0.32, P = .017 and ρ = 0.473, P < .001, respectively), suggesting that patient degenerative changes typically occurred across both the SMJs together.
Association Between Preoperative Tibial-SMJ Distances and Patient-Reported Outcomes
Median preoperative and postoperative PROMIS scores for the cohort are shown in Table 2. At a minimum of 1-year follow-up, there was no difference in PROMIS scores between patients with postoperatively reduced sesamoids (sesamoid grade 0) and those with persistent sesamoid subluxation (sesamoid grades >0) (all P values > .25).
PROMIS Scores for the Entire Cohort and for Patients With Postoperatively Reduced Sesamoid (n = 43).

Abbreviations: IQR, interquartile range; PROMIS, Patient-Reported Outcomes Measurement Information System.
For patients with postoperatively reduced sesamoids, when controlling for preoperative PROMIS scores and postoperative minimum tibial-SMJ distances, preoperative minimum tibial-SMJ distance was significantly associated with 1-year postoperative PROMIS physical function scores (coefficient 7.2, P = .02). Although not statistically significant, there were negatively associated trends between the preoperative minimum tibial-SMJ distance and 1-year postoperative PROMIS pain interference (coefficient −3.7, P = .22) and pain intensity (coefficient −5.2, P = .08). Partial effect plots illustrating the association between preoperative minimum tibial-SMJ distances and 1-year PROMIS outcomes scores are shown in Figure 3. There was no association between postoperative minimum tibial-SMJ and postoperative PROMIS physical function, pain interference, and pain intensity scores (all P values > .20).

Partial effect plots controlling for preoperative PROMIS scores and postoperative sesamoid-metatarsal joint distance representing the correlation between tibial sesamoid preoperative minimum distance. (A) 1-year physical function scores (coefficient 7.2, P = .02). (B) 1-year pain intensity scores (coefficient −5.2, P = .08). (C) 1-year pain interference scores (coefficient −3.7, P = .22). (PROMIS, Patient-Reported Outcomes Measurement Information System.)
Discussion
In this study, we aimed to quantify the degenerative changes at the SMJ in patients and investigate the association of these changes with postoperative outcomes. The distances measured between the sesamoids and the first metatarsal head in hallux valgus were typically between 0.8 and 1.6 mm preoperatively, depending on the method used. However, preoperative tibial- and fibular-SMJ distances were not associated with postoperative tibial- and fibular-SMJ distances. In our limited sample of patients, worse preoperative degenerative changes measured by the minimum distance between the tibial sesamoid and first metatarsal head in patients who had reduced sesamoids postoperatively were associated with lower 1-year postoperative PROMIS physical function scores. This result suggests that although some patients with degenerative changes at the SMJ preoperatively may have an improvement in their sesamoid subluxation and SMJ distances postoperatively, preoperative degenerative changes may influence patient-reported outcomes even if a more normal relationship between sesamoids and the first metatarsal head is restored.
Patient discomfort from hallux valgus has been attributed to shoe fit, prominence of the medial eminence, and malalignment of the first metatarsophalangeal joint.22,25,28 These theories have guided treatment approaches, assuming that addressing factors like ill-fitting footwear would alleviate pain. There remains a limited understanding of the factors that cause pain and dysfunction in hallux valgus deformities. 15 Up to one-third of patients remain dissatisfied following surgical correction of their hallux valgus deformity, highlighting the need for a more comprehensive understanding of the condition and its treatment. 2
One potential cause for persistent dissatisfaction after surgical correction of hallux valgus is osteoarthritis at the SMJ. 23 Few studies have investigated the relationship between degenerative changes at the SMJ and outcomes. Although plain radiographs are the most common imaging modality to assess hallux valgus deformities, they may not be able to appropriately investigate the relationship between the sesamoids and the first metatarsal head.7,17,29 A recent study by Kim et al 16 raised concerns about the reliability of weightbearing anteroposterior (AP) radiographs in assessing sesamoid position in hallux valgus patients. They described a group of patients with “pseudo-sesamoid subluxation,” defined as a high-grade sesamoid position on AP radiographs but reduced sesamoid subluxation on axial WBCT views. They reported that “pseudo-subluxation” of the sesamoids occurred in 26% of patients and may be due to increased first metatarsal pronation. Consequently, weightbearing AP radiographs may not be reliable for assessing postoperative sesamoid position.17,29
Clarke et al 6 also investigated degenerative changes at the SMJ using WBCT scans. They found a significant correlation between the crista volume and sesamoid station in hallux valgus patients. The results showed that the crista volume decreased significantly as sesamoid subluxation increased. This correlation was strong (r = −0.80, P < .001), indicating that the more the sesamoids are displaced, there is a correlated loss of SMJ architecture and degenerative change. Our study did not necessarily corroborate these findings, as preoperative and postoperative tibial-SMJ and fibular-SMJ distances were not associated with the sesamoid grade. However, almost all patients in our cohort had some amount of preoperative sesamoid subluxation (96.5%), and even mild subluxation of the sesamoids may cause cartilage erosion over time. Therefore, sesamoid subluxation is likely not a good proxy for degenerative changes at the SMJs.
Few previous studies have investigated the role of degenerative changes at the SMJ with patient-reported outcomes. 19 In this setting, our study aimed to shed light on the relationship between degenerative changes at the SMJ, as assessed through WBCT scans, 24 and patient-reported outcome scores at 1-year follow-up after a modified Lapidus procedure for hallux valgus correction. The observed association between preoperatively reduced joint space at the tibial SMJ and adverse 1-year postoperative functional outcomes aligns with the biomechanical significance of joint congruity.
Other factors have also been shown to affect outcomes following corrective hallux valgus surgery and may also contribute postoperative dissatisfaction. Previous studies have demonstrated that recurrence of HV deformity,3,11 secondary metatarsalgia, 3 hallux varus deformity,3,11,20 undercorrection of the first metatarsal rotation deformity,10,13 and the need for secondary procedures,3,14,20 are all potential causes of dissatisfaction. Our study suggests that preexisting degenerative changes at the tibial-SMJ may also affect postoperative outcomes following surgery for hallux valgus.
We found a correlation between preoperative tibial sesamoid distance and 1-year postoperative PROMIS physical function scores. The SMJ plays a vital role in load distribution and joint stability during gait and weightbearing activities.25,26,33 Potentially, the reduction in joint space may alter joint mechanics, influence foot function, and cause limitations in daily activities.15,23,32 Additionally, although not statistically significant, we found that patients with decreased tibial SMJ space tended to have higher pain at 1 year postoperatively. This trend may underscore the importance that worsening preoperative degenerative changes at the tibial-SMJ may influence postoperative outcomes.
Conversely, our study did not identify a substantial correlation between postoperative degenerative changes at the SMJs and patient-reported outcomes. Potentially, preoperative distances at the SMJs more accurately represent degenerative changes at these joints as postoperative distances at the SMJs may be influenced by the preoperative cartilage wear pattern of the joints. For example, a patient with a subluxated tibial sesamoid with cartilage completely worn away preoperatively but not worn away under the metatarsal head may have a greater postoperative distance at the tibial SMJ than the average patient. In contrast, a patient with a tibial sesamoid that was partially subluxated preoperatively but has partially worn away the cartilage of both the tibial and metatarsal sides of the SMJ would have a lesser postoperative distance. The patient with the tibial sesamoid that was completely subluxated preoperatively may have a worse postoperative outcome because of eburnation of the tibial sesamoid despite a greater postoperative distance at the SMJ. Therefore, reduction of the sesamoids may mitigate or alter the relationship between distances at the SMJ and postoperative outcomes, and there was some individual variability in the change in SMJ distances between patients, with some patients having an increased SMJ distances postoperatively and others decreased SMJ distances postoperatively. Ultimately, the amount of cartilage wear at the SMJs before surgical intervention may not be reversible postoperatively despite adequate correction of the sesamoids.
This study has some important limitations to consider. The study population was a sample of convenience and included consecutive patients who met all inclusion criteria. Therefore, no a priori power analysis was performed. The study was limited by the number of patients who had preoperative and postoperative WBCT scans as well as those who completed 2-year postoperative PROMIS scores. At our institution, postoperative WBCT scans are typically obtained to evaluate fusion of the first tarsometatarsal arthrodesis site, even in the absence of symptoms, but are not routinely obtained by all providers. This process limited our cohort, and we may have been underpowered to find a correlation between tibial SMJ distance and postoperative PROMIS pain intensity and pain interference scores. Additionally, distance mapping was used as a proxy for cartilage wear in the SMJs, which may not directly correlate with osteoarthritis. Other factors that we were unable to control for such as rotational changes of the metatarsal and variability in the plantar surface of the first metatarsal head between individuals may contribute to differences in decreased preoperative SMJ distances. Degenerative changes at the SMJs were not directly visualized at the time of surgery.
Conclusion
This study suggests that correction of the hallux valgus deformity using a modified Lapidus procedure results in a statistically significant increase in the distance between the tibial sesamoid and first metatarsal head. However, no change was found in the preoperative to postoperative distance between the fibular sesamoid and first metatarsal head. Additionally, in a subset of patients with reduced sesamoids postoperatively, a lower preoperative tibial sesamoid distance at the SMJ joint was associated with lower PROMIS physical function outcomes at 1 year following corrective surgery for hallux valgus. Our results suggest that preexisting SMJ arthritic changes are associated with lower postoperative outcomes despite complete reduction of the sesamoids. Although many factors may contribute to decreased patient-reported outcomes following correction of the hallux valgus deformity, degenerative changes at the SMJ may be a source of dissatisfaction.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241256370 – Supplemental material for Preoperative Degenerative Changes at the Tibial Sesamoid-Metatarsal Joint in Hallux Valgus: Association With Postoperative Patient-Reported Outcomes After Modified Lapidus Procedure
Supplemental material, sj-pdf-1-fao-10.1177_24730114241256370 for Preoperative Degenerative Changes at the Tibial Sesamoid-Metatarsal Joint in Hallux Valgus: Association With Postoperative Patient-Reported Outcomes After Modified Lapidus Procedure by Sophie Kush, Stone R. Streeter, Agnes D. Cororaton Jones, Brett Steineman, Scott J. Ellis and Matthew S. Conti in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the Hospital for Special Surgery Institutional Review Board (IRB# 2013-038-CR10) with approval from the registry steering committee (2022-24).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.