
Abstract
Background:
Orthopaedic surgical interventions are often costly, not only due to the procedures themselves, but also due to the need for frequent follow-up and imaging tests. Recent orthopaedic literature across several subspecialties has produced evidence suggesting that routine immediate postoperative radiographs do not provide any clinical advantage to justify their costs. This study aims to evaluate the economic feasibility of first postoperative radiographs after minimally invasive (MIS), fourth-generation MIS transverse double osteotomy for treatment of hallux valgus.
Methods:
We retrospectively evaluated patients with hallux valgus treated with fourth-generation MIS transverse double osteotomy between January 2019 and December 2021. Medical records were reviewed to assess changes in management following initial radiographs taken on average 1.38 ± 0.83 weeks after surgery. Direct costs of radiographs at the first postoperative visit (FPOV) were estimated using 2025 Medicare Fee Schedule data (HCPCS Code 73630), United Healthcare cost estimator website (zip code 33146), and multiple locally available public self-pay resources. National costs were estimated using Medicare data for the estimated 110,000 to 220,000 annual bunion procedures performed in the United States.
Results:
A total of 245 patients were included in our analysis. Four patients (1.6%, 95% CI 0.64%-4.12%) had an FPOV radiographic finding that warranted a change in management. Reasons included 1 (0.4%) loss of reduction of the first metatarsal osteotomy, 1 (0.4%) fracture through the Akin proximal phalanx osteotomy, and 2 (0.8%) subluxations of lesser toes fixated via K-wire. The cost per 3-view radiograph of the foot ranged from $31.68 to $106, depending on provider and payment type. National costs of routine radiographs for MIS bunion were estimated to be between $3.5 million to $23.3 million annually.
Conclusion:
Routine radiographs after fourth-generation MIS transverse double osteotomy surgery at FPOV rarely result in a change of management. In patients without clinically visible signs or symptoms warranting intervention, radiographs in the FPOV are rarely justified for MIS bunionectomy patients. We recommend physical evaluation at FPOV but suggest that substantial health care expenses could be saved by removing unnecessary FPOV radiographic analysis.
Level of Evidence:
Level IV, therapeutic/economic case series.

Keywords
Introduction
Routine immediate postoperative radiographs have become standard practice across various orthopaedic subspecialties, serving as a cornerstone in early postoperative clinical decision making and patient management. Early postoperative imaging (EPI) is typically performed to verify appropriate implant positioning, assess the adequacy of fracture reduction, and ensure accurate documentation of imaging studies within the electronic medical record. 5 However, emerging literature across multiple orthopaedic procedures suggests that in the absence of complications or clinical concerns, immediate postoperative imaging may provide limited clinical benefit while contributing significantly to healthcare costs.2,3,9,13 Although these studies highlight a trend observed across various orthopaedic subspecialties, specific research focusing on foot and ankle procedures such as minimally invasive bunion surgery is limited.
Hallux valgus (HV), a prevalent forefoot deformity affecting up to 23% of adults aged 18-65 years and 35.7% of those aged ≥65 years, has historically been treated with open osteotomies and soft tissue procedures, with minimally invasive surgery (MIS) gaining popularity recently because of its potential benefits including smaller incisions, faster recovery, and improved postoperative range of motion. 6 Despite these advantages, postoperative protocols often mirror those of traditional open procedures, including routine early radiographic evaluation. In some cases of open HV procedures, the use of postoperative radiographs was proposed to be unnecessary; whether this practice is necessary or cost-effective in the setting of MIS bunion surgery remains unclear. A recent study revealed similar findings where patients who received open scarf osteotomies also did not have early postoperative radiographic studies and found that it made no difference in the postoperative management. 10
In this study, we examined 245 patients who underwent the fourth-generation MIS transverse double osteotomy technique to evaluate the clinical utility and economic implications of early postoperative radiographs following minimally invasive hallux valgus correction.
Materials and Methods
Study Design
We retrospectively analyzed patients who underwent fourth-generation MIS transverse double osteotomy surgery for treatment of hallux valgus at a single outpatient center between January 2019 and December 2021, with all operations in this study carried out by 3 board-certified foot and ankle surgeons (N = 245; 109:84:52) having specialized training in MIS techniques. Our study was approved by our institution's Institutional Review Board (IRB 1952671-6). Patient demographic information was obtained from electronic medical record review. Patients included in our study (1) had symptomatic hallux valgus, (2) elected to do MIS bunion surgery for treatment, and (3) had consistent postoperative follow-up, including a first postoperative visit within 2 months. We excluded patients (1) under the age of 18 years, (2) those with symptomatic osteoarthritis, (3) an open procedure, or (4) patients with inconsistent follow-up.
Electronic medical records for each patient included in the study were reviewed to assess radiograph findings at the first postoperative visit (FPOV) and if subsequent modifications to the patients’ postsurgical care were documented. Review of radiographic data focused on markers for goals of treatment and possible complications including the maintenance of correction (hallux valgus angle [HVA], intermetatarsal angle [IMA], proper fixation or reduction, subluxations, and osteotomy site malalignment). We used these markers to reveal if such findings resulted in changes in care such as in weight-bearing status, precautions, scheduling of additional follow-up visits, a return to the operating room, or any other divergence from the standard postoperative protocols, which include full weightbearing as tolerated in a postoperative sandal up to 2 weeks followed by progression of activities as tolerated.
Cost Analysis
Direct costs of radiographs at the FPOV were estimated using the 2025 Medicare Fee Schedule data (HCPCS Code 73630), United Healthcare cost estimator website (zip code 33146), and multiple locally available public self-pay resources.14,15 In gathering the self-pay cost estimate for the Current Procedural Terminology code 73630 in the zip code 33146, an extraction of multiple publicly available prices were sourced for imaging centers, surgical centers, and outpatient hospitals. These prices came from pricing tools, health transparency websites, and institutional fee websites to give us an estimated self-pay cost for multiple locations.16 -18 However, heterogeneity in pricing and limited transparency make it difficult to determine an exact self-pay cost. National costs were estimated using Medicare data applied to the estimated 110,000 to 220,000 annual bunion procedures performed in the United States. 4 A percentage of how many patients would represent each payment category—private insurance (66.1%), public insurance (25.9%), and self-pay (8.0%)—was obtained using 2024 census data. An exact percentage of fourth-generation bunion patients was not obtained because there is a lack of information giving specific distribution of insurance types for patients who have undergone fourth-generation MIS transverse double osteotomy. Table 1 illustrates the cost ranges across payment and location categories.
Insurance Radiographic Costs per Different Healthcare Providers. a

Cost analysis of 3-view foot radiograph for procedure volume based on practice setting and payer type. Procedure volume is separated into Low, Median, and High estimates for the United States, with costs represented in US dollars (USD) depending on the practice and payer type.
Results
A total of 245 patients were included in our analysis. Table 2 summarizes patient demographics. All patients received fourth-generation MIS transverse double osteotomy, and 63 (25.7%) of patients had an additional lesser toe(s) osteotomy to assist in correction of hallux valgus.
Patient Demographics. a

Continuous data are represented as mean ± SD. Categorical data are expressed as a count (percentage of total).
Our patients received their first radiographs at a mean time of 16.03 days postoperatively (SD = 7.73). Four patients (1.6%) had an FPOV radiographic finding that warranted a change in management. One patient (0.4%) with loss of reduction of the first metatarsal osteotomy because of walking barefoot and pivoting on the foot without supportive equipment 2 days after surgery, resulting in a return to the operating room. One patient (0.4%) had a shift of the Akin proximal phalanx osteotomy screw as they fell and hit their toes. The patient was advised that no immediate change in postoperative protocol was needed but that the screw would need to be removed once the bone had healed. Two patients (0.8%) had subluxation of lesser toe fixated via K-wire as a result of both patients hitting their foot against a hard surface; 1 patient returned to the operating room for revision, whereas the other was able to have the K-wire adjusted in the clinic (Table 3). It is important to note that all 4 of these patients had a deviation from the traditional postoperative protocol, and all 4 patients had a lesser toe operation alongside the fourth-generation MIS. There were 2 cases of patients who had a deviation from postoperative protocol that did not warrant a change in management. One patient presented to the emergency room and clinic 6 days after surgery as they had concerns of deep vein thrombosis as their operative foot was red and swollen. A bilateral venous ultrasonography was performed and found to be negative. The patient was discharged with no change in management and told to return in case of worsening symptoms. The second patient returned to the clinic reporting sharp pain from the operative foot. This was due to positioning the contralateral foot on top of their operative foot and having excessive movement in bed. There was no change in management needed. Unfortunately, we are unable to determine how many patients deviated from the postoperative protocol without making the clinic aware, it was assumed that if this was the case, then no complication occurred that could be noticed in the postoperative radiographs would. That the other 59 patients also had lesser toe operations without deviation from the postoperative protocol suggests that the additional operation played little to no role in the incidence of their change in management, and is mainly attributed to deviations or external trauma.
Protocol Management Changes at First Postoperative Visit.
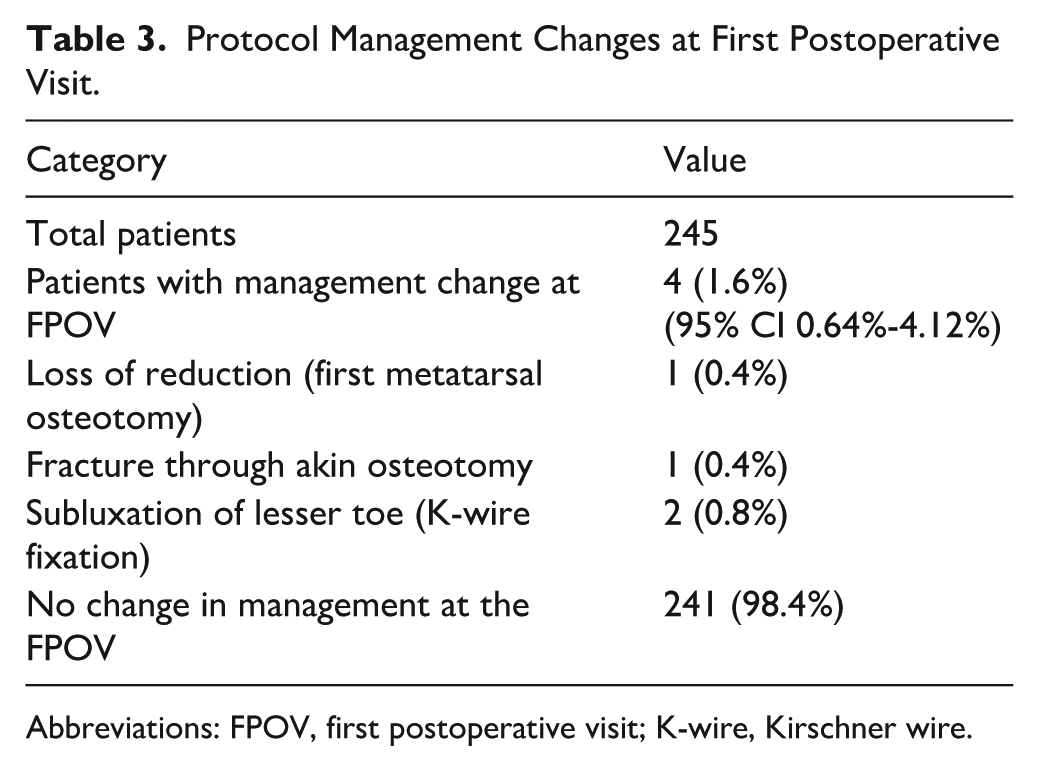
Abbreviations: FPOV, first postoperative visit; K-wire, Kirschner wire.
Cost Analysis
The cost per 3-view foot radiograph ranges from $31.68 to $106, depending on the payment type and provider. Within the Medicare National Fee Schedule, this includes a professional component (Modifier 26) of $7.76 with a technical component (TC) of $25.23. Using the Medicare National Fee Schedule, United Healthcare cost estimator website (zip code 33146), and multiple locally available public self-pay resources against the annual incidence of bunion surgery, the national estimated cost of routine radiographs for MIS bunion was found to be between $3.5 million to $23.3 million annually. Of the 245 patients in this study, when placed into their respective payment category for hospital radiographs, it was found that 54 had public insurance (22.0%), 184 private insurance (75.1%), and 7 self-paid (2.9%).The total amount was spent to obtain radiographs for each patient at their respective price was $21696.69 (Table 2).
Discussion
Only 1.6% of our patients had a change in management based on radiographic findings, with these patients having an earlier first follow-up appointment, on average being 1.38 ± 0.83 weeks, because of their individual circumstances. Because the only changes in postoperative management were due to nonadherence or external trauma, we recommend that patients who fall into these categories have a first follow-up radiographic study performed. We believe that immediate postoperative radiographs can be delayed unless a clinical picture indicates a necessity for investigation. Standard patients who follow postoperative protocol may obtain their first radiograph at 6 weeks, with follow-up studies at the 12-, 26-, and 52-week marks to track cortical formation and primary ossification.
There has been growing controversy whether early radiographic imaging is necessary among many orthopaedic surgery patients. Recent studies have raised the question whether radiographic analysis in the early postoperative period influences postsurgical decisions and whether the associated costs can be justified in a value-based health care environment. Numerous subspecialties in orthopaedics including shoulder arthroplasty, hip, and pediatric implant removal have all similarly reported that early postoperative radiographs may not provide meaningful insights into the future plan of postoperative care.1,3,10 On the contrary, Pansek et al 13 found that in spinal fusion for scoliosis, these early radiographic studies are quite versatile and are imperative to determine clinical management of patients. Literature analyzing the utility and cost of routine first postoperative radiographs following geriatric hip fracture fixation indicated that these imaging modalities led to minimal change in physician-guided management.7 -9 However, only 1 of the 241 patients seen in Monir et al 10 had their future plan of treatment altered because of irregularities in their radiograph. Despite an emerging consensus regarding the use of early postoperative radiographs, incongruity of best postoperative management practices exists in the field.
Patient management in the early postoperative period typically includes a patient interview, physical examination, and radiographs to evaluate for prosthetic and reduction patency, postoperative complications, and overall clinical status of the patient. Among all possible orthopaedic postoperative complications, efforts are most prioritized to address infection, malunion, loss of reduction, and additional fracture. If the aforementioned complications are not quickly identified and addressed, the prognosis for the patient becomes exponentially worse.
Our study indicates that first follow-up visit radiographs in patients undergoing MIS bunion surgery rarely reveal findings that would necessitate a change in patient management. This affirms several other studies addressing the same question amongst other orthopaedic subspecialties. Birir et al 2 demonstrated in total knee arthroplasty that early postoperative radiographs have utility in a clinical setting but significantly increase the cost of health care and expose the patients to unnecessary radiation. Although a single radiograph delivers negligible radiation, it serves as an example of the many postoperative radiographic studies that tend to be overordered. Additionally, Murphy and Blundell 12 also found that routine postoperative radiographs demonstrated low clinically usefulness in total hip arthroplasty and scarf osteotomy, respectively. These findings are evident in almost every subspecialty of orthopaedics except spine. Routine postoperative radiographs obtained following primary total knee arthroplasty, total hip arthroplasty, shoulder arthroplasty, and scarf osteotomy provide low clinical utility, although contributing to substantial health care costs.2,3,10,11,12
Although opting out of the first postoperative visit entirely would lower total costs via removal of transportation expenses for patients, we are recommending that patients still come in for a physical assessment but forgo a first follow-up radiographic image series. This way, providers can still assess for infection, range of motion, pain, take out sutures or staples, and rule out other complications while simultaneously lowering the overall costs for the patient and the health care system. If the physical assessment is concerning, imaging should be obtained for a definitive diagnosis. In addition, a diagnosis should never be made without a full radiographic study. Regardless, other complications can still occur, and 6-week radiographs will allow physicians to see the rate of healing for the osteotomy and comparison studies. This is also important to avoid legal cases. However, it is strongly recommended that intraoperative fluoroscopy be taken and saved to obtain a baseline study. In addition, an initial follow-up x-ray can still be performed, if clinically warranted, based on findings at the first follow-up examination.
This retrospective, single-center study cannot establish causality and may be subject to selection and documentation bias. Examination-radiograph correlations at FPOV were not prospectively standardized, and adherence deviations may be underreported. Cost estimates combine Medicare rates, insurer tools, and self-pay “list” prices; national savings are scenario-based and sensitive to payer mix and site-of-service. Findings pertain to fourth-generation MIS bunionectomy and should not be extrapolated to other procedures without comparative data. However, the patient population included is representative of the broader demographic affected by hallux valgus—primarily women over the age of 60 years. External orthopaedic literature published by Cai et al 5 supports these data, showing that the condition is more common in females compared with males, with prevalence increasing with age: from 11% in those <20 years old, to 12.22% in adults aged 20-60 years, to 22.7% in those aged >60 years. Additionally, data was obtained from procedures performed at a single outpatient center, which may not reflect the variability in outcomes seen across different practice environments. Although all operations in this study were carried out by 3 board-certified foot and ankle surgeons (N = 245; 109:84:52) with specialized training in MIS techniques, this may not reflect outcomes in the broader community, particularly among surgeons with varying levels of experience or different training backgrounds. We also recognize sociodemographic factors such as insurance status, geography, and access to follow-up care in this analysis may also influence outcomes. Finally, although our findings provide meaningful insights into the use of immediate radiographic imaging following MIS techniques in the foot and ankle domain, these findings should not be extrapolated to other orthopaedic subspecialties without appropriate comparative data. Our results are consistent with emerging literature in other orthopaedic fields, such as sports medicine and trauma, which suggests that immediate postoperative radiographs are an addressable cost burden unless indicated as a clinical necessity for investigation.
Conclusion
Immediate postoperative radiographs are a valuable resource that allows surgeons to address important postoperative complications and provide the clinician with assurances in patient care. However, their utility in foot and ankle patients without clinical signs and symptoms of pathology are a burden to medical resource best practices. We estimate that judicious use of radiographs could save our health care system up to $23.3 million annually for this specific subset of foot and ankle patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251388084 – Supplemental material for Economic Feasibility of Routine First Postoperative Radiographs in Minimally Invasive Bunion Surgery
Supplemental material, sj-pdf-1-fao-10.1177_24730114251388084 for Economic Feasibility of Routine First Postoperative Radiographs in Minimally Invasive Bunion Surgery by Taylor Schnepp, Chase Burzynski, Kyle A. Lorenzo, Teana Tee, David Vasserman, Jonathan Gibbs, Jorge N. Gil, Thomas P. San Giovanni and Cary B. Chapman in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
This study has been approved under Baptist Health Institutional Review Board (IRB approval no. 1952671-5).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cary Chapman, MD, reports general disclosures of Enovis, consultant; Conventus, consultant. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.