
Abstract
Background:
Hallux valgus deformity affects more than 35% of people aged ≥65 years. Surgical correction in this population can be more complicated because of poor bone quality, worse deformity, and postoperative recovery challenges. The purpose of this study was to compare the radiographic and clinical outcomes of patients aged ≥65 years who underwent either open Lapidus or minimally invasive chevron Akin osteotomy for bunion correction.
Methods:
A retrospective review identified 62 patients aged ≥65 years who were treated surgically for hallux valgus with at least 1-year postoperative Patient-Reported Outcomes Measurement Information System (PROMIS) scores (physical function and pain interference). Preoperative and at least 6-month postoperative radiographs were measured for the hallux valgus angle and intermetatarsal angle. PROMIS scores were obtained preoperatively and at 1 and/or 2 years postoperatively. Differences in demographic, clinical, and radiographic outcomes were assessed using the Mann Whitney U test and P values were adjusted for a false discovery rate of 5%.
Results:
There was no difference between the MIS and open cohorts in pre- or postoperative radiographic measurements or clinical outcomes at any time point. At 1 year postoperatively, both groups had statistically significant improvements in the PROMIS pain interference domain but only the MIS group had a statistically significant improvement in the PROMIS physical function domain. Clinical significance was equivocal. At 2 years postoperatively, there were clinically and statistically significant improvements in the PROMIS pain interference and physical function domains for the open and MIS groups.
Conclusion:
Patients in both surgical groups had improvement in radiographic measurements and 2-year PROMIS scores, although there was no clinical or statistical difference found between groups. MIS and open surgical techniques appear to be safe and effective in correcting hallux valgus in older patients; however, patients may need to be counseled that maximum improvement after surgery may take more than 1 year.
Level of Evidence:
Level III, retrospective cohort study.
Keywords
Introduction
Hallux valgus deformity, also known as a “bunion,” is a complex forefoot deformity characterized by progressive abduction and pronation of the first phalanx along with adduction, pronation, and elevation of the first metatarsal. The incidence of this deformity increases with age and affects more than 35% of individuals aged ≥65 years.19,20,23,26 Surgical correction in this population can be more complicated because of the higher likelihood of poor bone quality, worse deformity, increased risk of recurrence, and postoperative recovery challenges associated with weightbearing restrictions.9,21 There is no consensus on which surgical option is the best in this age group. Minimally invasive bunionectomy (MIS) has gained popularity, namely, because of evidence showing reduced recovery time, earlier weightbearing, and less postoperative pain, which can eliminate the need for opioids,13,17 all of which are beneficial to older surgical patients.8,14
Throughout the orthopaedic literature, there are very few studies directly comparing outcomes following open and minimally invasive bunionectomy. A previous study comparing outcomes of MIS chevron bunionectomies to the modified Lapidus procedure found similar correction and Patient-Reported Outcomes Measurement Information System (PROMIS) scores between the 2 groups. 7 However, the average age in this study was approximately 50 years. 7 Multiple studies have shown surgical correction of hallux valgus to be advantageous even within an older population.18,22
Given the challenges associated with surgical correction and postoperative care in an older patient, it is imperative to determine if there is a particular surgical option that is best for this population. The purpose of this study was to compare the radiographic and clinical outcomes of patients aged ≥65 years who underwent either open Lapidus or minimally invasive chevron osteotomy for bunion correction.
Methods
Participants
Following institutional review board approval, a retrospective review of prospectively collected data within an institutional outcome registry was performed. Information obtained from the registry included demographic information, surgical information, and preoperative and postoperative PROMIS scores (1- and/or 2-year scores). Chart review was performed to obtain patient height and weight in order to calculate body mass index, confirm the registry-obtained surgical procedures, and determine if there were any postoperative complications or additional surgeries required (removal of hardware, recurrence of hallux valgus deformity, development of hallux varus deformity, nonunion, metatarsalgia, and nonremoval of hardware procedures required postoperatively). Inclusion criteria included (1) patients with a diagnosis of hallux valgus, (2) patients who were at least 65 years of age who underwent primary surgery to treat hallux valgus via open Lapidus or minimally invasive chevron osteotomy between January 2017 and August 2022 at a single institution, (3) minimum 1-year postoperative PROMIS scores, and (4) minimum 6-month postoperative radiographs. Exclusion criteria included (1) patients who were <65 years of age at the time of surgery, (2) patients undergoing revision surgery, (3) patients who lacked at least 1-year postoperative PROMIS scores, and (4) patients who lacked at least 6-month postoperative radiographs. Surgery was performed by 9 different surgeons throughout the inclusion period, 2 surgeons within the MIS group, and 9 surgeons within the open group.
Outcome Measures
PROMIS scores, including the physical function (PF) and pain interference (PI) T scores, preoperatively and 1 or 2 years postoperatively were used to assess patient outcomes. PROMIS scores are reported using a T score between 0 and 100—the national average within the Unites States is a T score of 50 and an SD of 10 points. For PROMIS functional scores (physical function), higher scores indicate greater physical function (better outcomes). For PROMIS symptom scores (pain interference), higher scores indicate greater pain interference (worse outcomes). The MCID for the PROMIS PF domain has been reported as 4.5 to 4.7 and for the PROMIS PI domain, the MCID has been reported as 4.1 to 4.3. 11
Radiographic Analysis
All radiographic measurements were done in PACS (picture archiving and communication system) software with digital radiographs. Preoperative and at least 6-month postoperative radiographs were identified for each patient. A foot and ankle fellowship-trained surgeon measured the hallux valgus angle (HVA) and intermetatarsal angle (IMA) on radiographs. The HVA is defined by the angle between the longitudinal axis of the first metatarsal and the longitudinal axis of the proximal phalanx. 12 The IMA is defined by the angle between the longitudinal axes of the first and second metatarsals. 12 Bunion severity was determined based on radiographic measurements: (1) mild, HVA < 20 degrees, IMA < 13 degrees; (2) moderate, HVA 20-40 degrees, IMA 13-16 degrees; or (3) severe, HVA > 40 degrees, IMA > 16 degrees. Radiographic recurrence was defined as HVA >20 degrees. 2 Hallux varus was defined as HVA <0 degrees.
Surgical Technique
All MIS bunion procedures included in this study were performed by one of 2 surgeons at a single institution. The MIS procedures were performed using standard MIS technique, as described by Vernois and Redfern. 24 The chevron osteotomy was fixed using either two 4.0-mm fully threaded headless screws or one 4.0-mm and one 3.0-mm fully threaded headless screw. The Akin was fixed with a fully threaded headless screw. Postoperatively, the patients were placed into a supportive dressing and allowed to begin weightbearing on postoperative day 1. Representative radiographs are presented in Figure 1.

Preoperative (left) and postoperative (right) weightbearing anteroposterior radiographs demonstrating the minimally invasive operative technique for bunion correction.
Nine surgeons performed open Lapidus bunionectomies within this study. Per standard procedure, 8 of the 9 surgeons indicate patients for the Lapidus procedure to treat hallux valgus regardless of bunion severity or first tarsal-metatarsal (TMT) hypermobility. The open Lapidus was performed via a dorsal incision over the first TMT joint and medial incision at the first metatarsophalangeal (MTP) joint as described by Mani et al. 16 A lateral release was performed through an incision in the first webspace. Akin osteotomies were performed at the surgeon’s discretion. The first TMT joint was fixed with either two 3.5-mm or 4.0-mm screws or a plate and crossing compression screw construct. Postoperatively, patients were placed into a well-padded splint and remained nonweightbearing for at least 6 weeks, after which they began a progressive weightbearing protocol. Representative radiographs are presented for each technique in Figure 2.

Preoperative (left) and postoperative (right) weightbearing anteroposterior radiographs demonstrating the open Lapidus technique for bunion correction via a plate-screw construct (top) or 2 crossing compression screws (bottom).
Statistical Analysis
A department-designated statistician performed the analysis of the collected data. Because of small sample sizes, differences in continuous variable outcomes between cohorts were assessed using the Mann Whitney U test, while paired differences in outcomes with continuous variables between cohorts were tested using the paired Wilcoxon signed-rank test with continuity correction. Differences in binary outcomes were assessed using Fisher exact test. For hypothesis testing, both unadjusted and adjusted P values at a false discovery rate of 5% were reported.5,6 Statistical significance was established at an alpha level of 0.05 for hypothesis testing. Analysis was conducted on R: A Language and Environment for Statistical Computing (R Core Team, Vienna, Austria) with the confintr package.
Results
There were 214 patients aged ≥65 years who underwent hallux valgus surgery within the study period. Eighty-four patients (39%) had less than 3-month follow-up imaging and 20 patients (9%) had less than 6-month follow-up imaging, 40 patients (19%) underwent an operative procedure that did not include open Lapidus or minimally invasive chevron osteotomy (26 first metatarsal-phalangeal joint fusions, 10 open scarf osteotomies, 4 MIS Lapidus), and 8 patients (4%) underwent revision surgeries and were therefore excluded. Overall, there were 62 patients who met inclusion criteria, of which 31 were in the open Lapidus (open) cohort and 31 were in the minimally invasive chevron osteotomy (MIS) cohort. In the open cohort, the average age of the patients was 68 ± 2.7 years, the average body mass index was 24 ± 3.1, and 100% of patients were female. In the MIS cohort, the average age of the patients was 70 ± 4.6 years, the average body mass index was 24 ± 2.9, and 93% (29/31) were female (Table 1).
Demographic Information and Bunion Severity.

Abbreviation: MIS, minimally invasive surgery.
There was a statistically significant improvement within the PROMIS domain of pain interference for the open and MIS groups and physical function for the MIS group between preoperative and 1 and 2 years postoperative; however, there was only a significant difference at 2 years for the PROMIS physical function domain in the open group. No difference was noted in physical function at 1 year postoperation for the open group or between groups (Table 2). Clinical significance was achieved for both the open and MIS groups at 2 years postoperatively; however, clinical significance at 1 year postoperatively was equivocal.
Radiographic and PROMIS Outcomes for the Open and MIS Groups.

Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle; MIS, minimally invasive surgery; PF, physical function; PI, pain interference; PROMIS, Patient-Reported Outcomes Measurement Information System.
In the open group between preoperative and 1 year postoperative, there was an average improvement of 2.2 points in PF and 4.6 points in PI and a median improvement of 3.3 points in PF and 2.5 points in PI. Between preoperative and 2 years postoperative, there was an average improvement of 8.7 points in PF and 6.3 points in PI and a median improvement of 5.4 points in PF and 4.2 points in PI, which were both clinically and statistically significant improvements. In the MIS group at the 1-year postoperative time point, there was an average improvement in PF and PI of 4.4 and 4.3 points (median improvement in PF and PI of 4.9 and 2.4), respectively, and at the 2-year postoperative time point, there was a 9.3-point and 8.6-point improvement in PF and PI (median improvement in PF and PI of 8.9 and 6.1), respectively. For the open group between the 1- and 2-year time points, patients trended toward a statistically significant improvement in PF (P = .056) and had a clinically significant improvement in PF (6.5 points). For the MIS group between the 1- and 2-year postoperative time points, patients trended toward statistically significant improvement in in PF (P = .079) and PI (P = .13) and had a clinically significant improvement in PF (4.9 points) and PI (4.3 points).
Both the MIS and open cohorts showed clinically and statistically significant improvement in radiographic measurements between preoperative and postoperative radiographs. Of the 31 patients in the open group, 2 patients (6%) had mild, 13 patients (42%) had moderate, and 16 patients (52%) had severe bunion deformities. The HVA improved from 34 ± 10.0 degrees to 8 ± 11.4 degrees (adjusted P < .001), and the IMA improved from 15 ± 3.4 degrees to 5 ± 2.8 degrees (adjusted P < .001). In the MIS group, 1 patient (3%) had mild, 22 patients (71%) had moderate, and 8 patients (26%) had severe bunion deformities (Table 1). The HVA improved from 31 ± 7.4 degrees to 11 ± 8.7 degrees (adjusted P < .001), and the IMA improved from 14 ± 3.8 degrees to 3.8 ± 2.5 degrees (adjusted P < .001). There was no difference in HVA or IMA pre or postoperatively between groups (adjusted P > .05) (Table 2).
In regard to complications, the overall complication rate in the open cohort was 26% and the overall complication rate in the MIS cohort was 42% (adjusted P value > .05). See Table 3 for complications. There was no statistically significant difference found in complication rate between cohorts (adjusted P = .578).
Complications With the Open and MIS Groups.
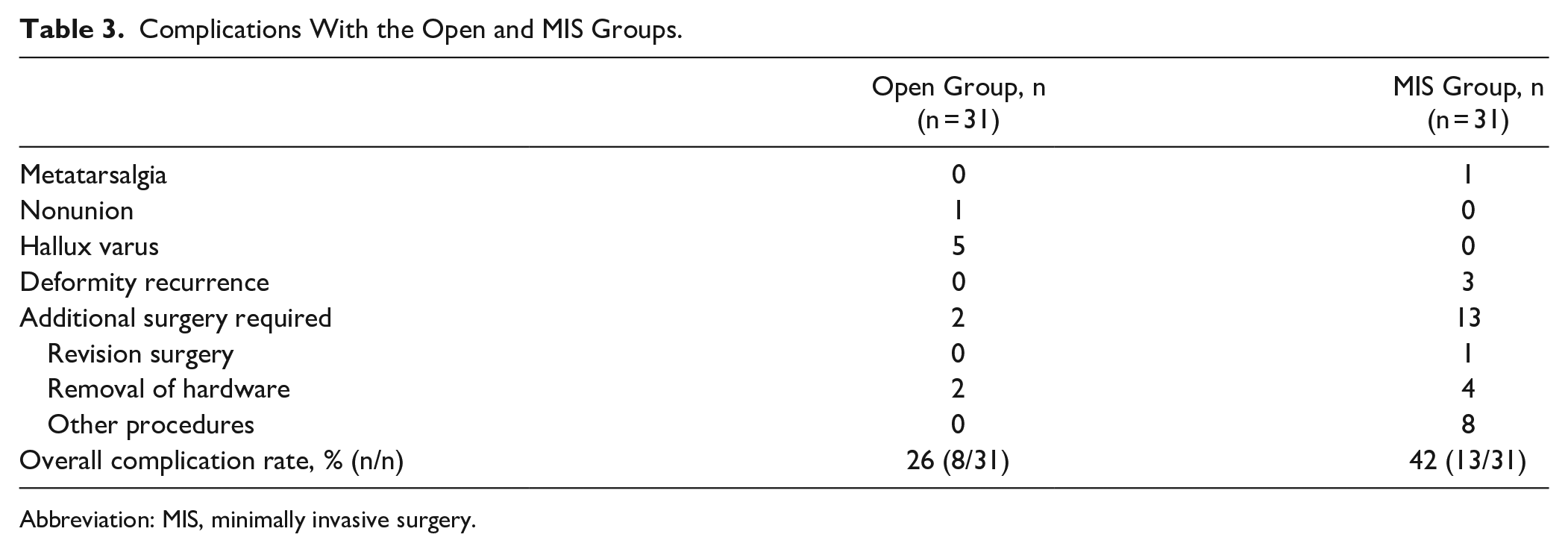
Abbreviation: MIS, minimally invasive surgery.
Discussion
To our knowledge, this is the first study to compare the radiographic and clinical outcomes of patients aged ≥65 years who underwent either open Lapidus or MIS chevron akin osteotomy for bunion correction. This study showed that despite significant improvement in both groups, there was no statistically significant difference in radiographic outcomes or PROMIS scores between the open or MIS groups at 1 or 2 years postoperatively, consistent with previously published literature.3,7
Surprisingly, patients in both the MIS and open groups made clinically significant gains in PROMIS PF scores between 1 and 2 years postoperatively. This was most pronounced in the open Lapidus group. The improvement in PF score within the open group was only statistically significant 2 years postoperation and not 1 year postoperation, which may suggest that it takes longer for patients to improve their physical function following open Lapidus to correct their bunion as compared to MIS bunion correction. One explanation for this may be differences in the postoperative protocol, as the MIS group was able to begin weightbearing after 24 hours postoperation, whereas the open group was nonweightbearing for 6 weeks. Early weightbearing in elderly patients has been shown to impact a patient’s independence and ability to return to their own home. 4 However, it was unexpected that both groups would have clinical improvements in PROMIS scores after 1 year postoperatively. The lack of statistically significant improvement was likely due to some patients being lost to follow-up at 2 years postoperatively. The primary outcome in this study was 1-year postoperative clinical outcomes as we anticipated differences between the MIS and open groups to be more pronounced with earlier follow-up. Additionally, a previous study demonstrated that subjective maximal improvement following a total ankle arthroplasty was 1 year postoperatively. 1 Despite bunion surgery being considered a less aggressive surgery, our study suggests that maximum improvement may be between 12 and 24 months after surgery for patients aged ≥65 years. This may help surgeons counsel patients about the expected improvement following both open and MIS bunion correction.
Following both open Lapidus and MIS correction, the average postoperative HVA and IMA was within normal parameters, and there was excellent overall correction. The results of this study in regard to the radiographic improvement in HVA and IMA are similar to results previously reported in the literature.15,20,25 Although prior studies have shown greater correction achieved with open bunion correction and improved IMA with MIS correction, there were no differences in radiographic parameters found within this study.20,25
The overall complication rate of 34% found within this study is higher than previously reported in the literature for hallux valgus correction surgery. The authors believe this increased complication rate is likely due to the variety of complications reported and the average age within the cohorts. A systematic review published in Foot & Ankle Orthopedics 10 in 2023 evaluated 17 studies that reported on MIS hallux valgus correction between 2008 and 2022. There were a total of 911 patients who underwent 1088 MIS procedures with an average follow-up time of 23.8 months. Overall complication rate was 16.6%, which included need for hardware removal (6.2%), recurrence (2.2%), nerve injury (2.2%), infection (1.1%), nonunion (0.4%), and hallux varus (0.09%). The average age of the patients in the systematic review was 54.4 years, as compared to the average age in this study of 70 years in the MIS cohort. Goh et al 9 reported a 5 times higher risk of recurrence in patients ≥60 years of age compared to those <50, so the recurrence rate of 10% in our MIS group is not surprising.
Strengths of the study include the use of a validated patient-reported outcomes metric, the length of clinical follow-up, and the inclusion of multiple surgeons, which may make the findings more applicable to a wider group of patients and surgeons. This study does, however, have several limitations. Inclusion criteria required the completion of 1-year postoperative PROMIS scores and at least 6-month postoperative radiographs, which may have introduced selection bias. Unfortunately, the single institution at which this study was conducted does not collect PROMIS scores at 3 or 6 months postoperatively, so these postoperative time points were not able to be included in analysis. Because of this, further studies need to be conducted in order to determine if there is a linear difference in physical function at any time points earlier than 1 year postoperation, as one might expect given the vastly different postoperative weightbearing protocols. Additionally, this study was performed at a single institution, which may limit its generalizability, although there were 10 operating surgeons whose patients were included in analysis.
Conclusion
Patients in both the MIS and open surgical groups had improvement in radiographic measurements and 2-year PROMIS scores, although there was no clinical or statistical difference found between groups. However, patients continued to make clinically meaningful improvements in PROMIS physical function and pain interference domains after 1 year postoperatively. Given the results, both MIS and open surgical techniques appear to be safe and effective in correcting hallux valgus in older patients, but in this age cohort, patients may need to be counseled that improvement after surgery may take more than 1 year. Future research is needed to evaluate whether there may be clinically relevant differences in shorter-term follow-up, as patients may have a faster early recovery in the MIS group.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241266843 – Supplemental material for Comparison of Minimally Invasive Chevron Akin and Open Lapidus Surgery in Older Patients at a Minimum 1-Year Follow-Up
Supplemental material, sj-pdf-1-fao-10.1177_24730114241266843 for Comparison of Minimally Invasive Chevron Akin and Open Lapidus Surgery in Older Patients at a Minimum 1-Year Follow-Up by Allison L. Boden, Grace M. DiGiovanni, Seif El Masry, Scott J. Ellis, A. Holly Johnson and Matthew S. Conti in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from the HSS Foot and Ankle Research Steering Committee (date accepted 11/27/23).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A. Holly Johnson, MD, reports royalties or licenses and consulting fees from Novastep and consulting fees from Treace. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.