
Abstract
Background:
Achieving interfragmentary compression and stability is critical for successful bone healing in fracture fixation and arthrodesis procedures. Modern orthopaedic plating systems incorporating variable-angle screw designs offer greater versatility; however, the impact of screw trajectory on interfragmentary compression and contact area has not been adequately explored. We questioned if the resultant forces applied by screw orientation would follow the basic principles of vector geometry.
Methods:
Interfragmentary compression and contact area were quantified in foam bone surrogate osteotomy models using plates allowing maximum screw angulation of either 15 or 30 degrees, with screws inserted at various angles. Cadaveric second-tarsometatarsal (TMT) arthrodesis constructs were subsequently used to validate the mechanical findings from surrogate testing.
Results:
Compression and contact area increased from 0 degrees to 15 degrees to 30 degrees in surrogate models (overall analysis of variance P < .001). Angling screws in the second bone fragment after securing the plate to the first fragment produced the largest compression gains. In cadaveric second-TMT constructs, 30-degree divergence increased compression (~15-fold; 49.4 ± 35.1 N vs 3.4 ± 3.8 N; P < .001) and contact area (~4-fold; 47.8 ± 28.9 mm² vs 12.8 ± 7.3 mm²; P < .001) compared with 0-degree divergence.
Conclusion:
With plate fixation, screw divergence from the arthrodesis/fracture line improved interfragmentary compression and contact area, particularly when divergent screws were inserted into the second bone fragment after the plate was secured to the first fragment. As hypothesized, the findings followed basic vector geometry.
Clinical Relevance:
Surgeons can optimize plate fixation quality and enhance stability in midfoot arthrodesis (and other procedures) by strategically angling locking screws in the second bone fragment after securing the plate to the first fragment. These biomechanical insights offer practical guidance for achieving superior interfragmentary compression and potentially reducing the risk of nonunion in clinical practice.
Keywords
Introduction
Successful bone healing in fracture repair and arthrodesis procedures depends on achieving both interfragmentary stability and compression. Stability is necessary to prevent excessive micromotion at the fracture site, 5 whereas compression enhances bony contact and facilitates healing. 17 Traditional orthopaedic fixation techniques typically rely on lag screws applied outside the plate to achieve compression before the plate is secured. 10 However, lag screws can be mechanically limited, relying on precise predrilled trajectories, which may disrupt fracture fragments or lead to suboptimal fixation in complex fractures. Although effective, these methods may complicate the surgical workflow, particularly in complex fractures requiring multiplanar stabilization. These challenges are even more pronounced in small-footprint joints such as the second tarsometatarsal (TMT), where hardware prominence and limited bone stock restrict optimal screw placement. This underscores the need for alternative methods to optimize interfragmentary compression while maintaining stability.
Recent advances in plating technology, including polyaxial locking screw designs,16,20,21 have introduced new possibilities for improving interfragmentary compression through plate-based fixation. Variable-angle screws allow for controlled insertion at nonperpendicular angles, enhancing versatility in addressing intraoperative challenges such as fragment capture or hardware avoidance. Bench work demonstrates mechanism- and angle-dependent performance in polyaxial interfaces,1 -4,6 -8,11 -13,15,16,18 and limited Lisfranc data (that did not control for screw angle) show similar outcomes for variable- and fixed-angle plates. 14 However, the effect of screw angulation on compression and contact area in a midfoot arthrodesis plate construct has not been quantified.
The purpose of this study was to quantify the effects of screw angulation on interfragmentary compression and contact area using foam surrogate osteotomy models, and to validate these biomechanical principles in human cadaveric second-TMT arthrodesis constructs. We hypothesized that increasing screw angulation, particularly when screws are angled strategically into the second bone fragment after the plate is secured to the first fragment, would significantly enhance compression and contact area in both surrogate and cadaver models following the principles of basic vector geometry.
Methods
Study Design and Models
Interfragmentary fixation was simulated using (1) foam bone surrogates (SawBones; Pacific Research Laboratories, Vashon, WA) to model fractures stabilized with interlocking orthopaedic plates and (2) fresh frozen human cadaveric lower-extremity specimens to model second TMT arthrodesis. Two-plate designs with differing maximum screw angulation capabilities were used to evaluate the effects of screw angle and screw angle configuration on interfragmentary compression and contact area (series 1 experiments only). Plate 1 allowed for a maximum screw angulation of 15 degrees (VariAx 4-hole straight narrow plate; Stryker), whereas plate 2 permitted up to 30 degrees of angulation (Arsenal 4-hole straight plate; Enovis). All experiments used plates appropriate to the assigned insertion angles: 0 /15-degree conditions were performed with plate 1 (maximum 15 degrees capability), and 30-degree conditions were performed with plate 2 (maximum 30 degrees capability). All 30-degree insertions were performed exclusively with plate 2; plate 1 was not tested above its 15-degree design limit.
All construct preparation and testing protocols were identical between surrogate and cadaveric models unless otherwise noted. A bridging plating technique was used. The first screw inserted into the second fragment (third screw overall) was placed through a nonlocking compression hole.
Foam Bone Surrogate Experiments
Plates were applied to the bone surrogates following manufacturer guidelines. Screws were inserted in distinct configurations to elucidate impact of screw angle and screw angle configuration:
Screw angle (experiment series 1, Figure 1A)
1. All screws perpendicular to the plate (0 degrees angulation).
2. All screws angled at 15 degrees.
3. All screws angled at 30 degrees.
Screw angle configurations (experiment series 2,Figure 2A)
1. First and second screws angled at 30 degrees, third screw (nonlocking) perpendicular, and fourth screw at 30 degrees.
2. First and second screws angled at 30 degrees with third and fourth screws perpendicular.
3. First, second, and third screws perpendicular, with fourth screw angled at 30 degrees.
4. First and second screws perpendicular, with third and fourth screws angled at 30 degrees.
5. All screws angled at 30 degrees away from the fracture line.
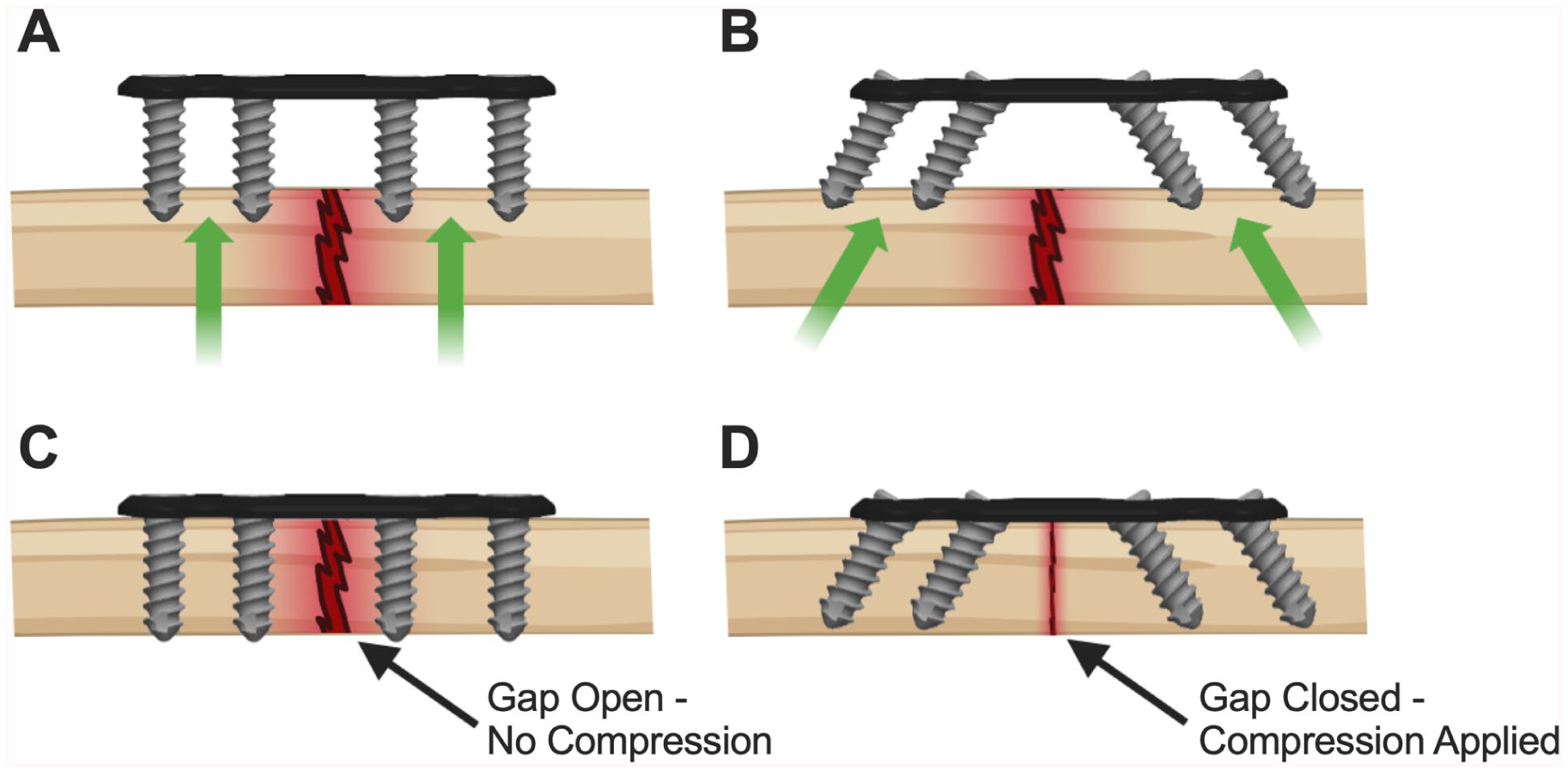
Screw angulation as a mechanism for interfragmentary compression. (A) Construct prepared with drill guides perpendicular to the plate (0 degrees) before screw insertion. (B) Construct prepared with drill guides set at 30 degrees toward the osteotomy before screw insertion; arrows indicate the convergent trajectory anticipated. (C) Image of the 0-degree construct after screws are fully tightened. Little change in fracture-gap width is seen. (D) Image of the 30-degree construct after screws are fully tightened. The osteotomy gap has closed appreciably, confirming that angled screws draw the fragments together.

Results of series 1 foam-surrogate experiments. (A) Representative constructs illustrating the 3 screw-angle conditions (0, 15, and 30 degrees) tested with plates that allow up to 15 degrees (plate 1) or 30 degrees (plate 2) of angulation. (B) Mean interfragmentary compression increased with each step from 0 to 15 to 30 degrees. (C) Contact area showed a parallel rise as screws were angled farther from perpendicular. Bars depict group means ± SD. Significant pairwise differences are marked by brackets and corresponding P values above the bars.
Cadaveric Specimen Procurement and Preparation
Twelve fresh frozen human lower‑extremity specimens (mean age ± SD = 67.8 ± 7.0 years; 14 male, 10 female) were obtained from an accredited tissue bank after institutional review board exemption. Limbs were thawed overnight and dissected to expose the second TMT joint while preserving surrounding soft tissues. Prior to instrumentation, all articular cartilage was removed using standard joint preparation tooling, replicating clinical preparation.
A fellowship-trained foot and ankle surgeon (S.A.) performed all plate placement and screw insertion under fluoroscopic guidance to ensure clinically realistic trajectories. Plates were applied dorsally in accordance with manufacturer guidelines. Informed by results of the foam bone model testing, paired cadaveric constructs used the following constructs:
All screws perpendicular (0 degrees) vs cuneiform (0 degrees), metatarsal (30 degrees, inserted after cuneiform screws)
All screws perpendicular (0 degrees) vs all screws inserted at 30 degrees.
Measurements and Instrumentation
Following the application of all screws, interfragmentary compression and contact area were quantified using calibrated pressure sensing film (TekScan Evolution) following methods adapted from prior foot and ankle arthrodesis and interfragmentary compression studies.9,19 Compression was measured as the force applied across the fracture interface, whereas contact area was evaluated as the total surface area in contact between fragments. Measurements were performed for each group to assess the effects of screw angulation and screw angle configuration.
Statistical Analysis
Experiment series 1 data were analyzed using a 2-way analysis of variance (ANOVA) with screw angle and plate type as main effects. Experiment series 2 data were analyzed using a 1-way ANOVA. All foam surrogate testing employed a Tukey post hoc test and a significance threshold of α = 0.05.
Cadaveric data were analyzed with a repeated measures ANOVA implemented in a generalized linear model framework. Two within-specimen factors were included: (1) screw angle (0 vs 30 degrees) and (2) insertion stage, defined as the measurement taken immediately after the first screw was placed in the metatarsal segment (stage 1, third screw overall) vs the measurement taken after the second screw was placed into the metatarsal segment (stage 2, fourth screw overall). The matched nature of the limbs served as the repeated measure. When a main effect or interaction reached significance (P < .05), pairwise comparisons were performed with Fisher least significant difference (LSD) test. Normality of residuals and homogeneity of variance were confirmed with Shapiro-Wilk and Mauchly sphericity tests, respectively.
Results
Experiment Series 1: Screw Angle and Plate Type
Interfragmentary compression increased with greater screw angulation (overall ANOVA P < .001; Figure 2, A and B). Mean compression across both plate designs at 15 degrees exceeded 0 degrees, and 30 degrees exceeded 15 degrees (44.7 ± 30.0 N at 0 degrees, 94.8 ± 21.2 N at 15 degrees, and 156.0 ± 27.0 N at 30 degrees), with Tukey post hoc tests confirming significant differences between every pair (all P < .001). Contact area followed the same monotonic pattern (overall ANOVA P < .001; Figure 2C), increasing from 22.1 ± 12.3 mm² at 0 degrees to 103.8 ± 23.7 mm² at 15 degrees and 211.0 ± 24.4 mm² at 30 degrees. The 2-way ANOVA did not reveal a significant difference between plate designs (P = .81); however, plate 2 at 30 degrees produced significantly increased compression as compared to both plates at 15 degrees (P < .001).
Experiment Series 2: Screw Angle Configuration
Screw angle configuration exerted a pronounced influence on construct mechanics (P < .001 for compression; Figure 3, A and B). Introducing angled screws in the first bone fragment only (group 2) produced the lowest compression (58.9 ± 23.9 N). In contrast, angling both screws within the second bone fragment, either exclusively (group 4) or in combination with angulation in the first fragment (group 5), resulted in marked gains: group 4 = 162.7 ± 51.9 N (P < .01 vs group 2) and group 5 = 198.2 ± 44.6 N (P < .001 vs group 2). No significant differences in contact area were noted between groups (P = .086; Figure 3C). These findings isolate the second-fragment screw orientation as the principal driver of interfragmentary compression and contact optimization.
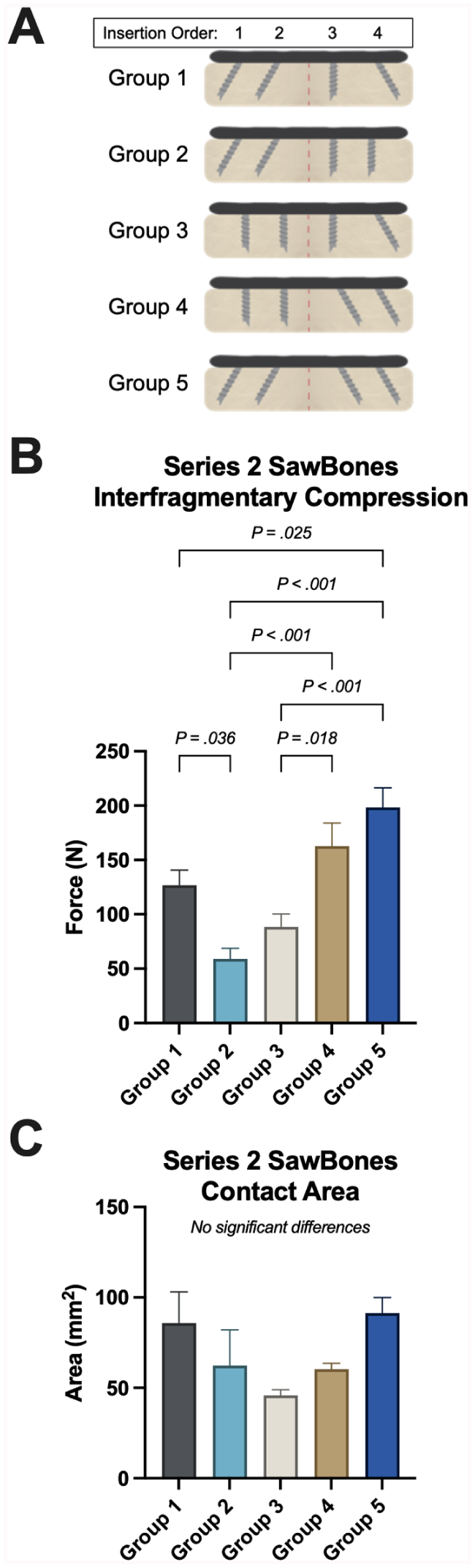
Results of series 2 foam-surrogate experiments (screw angle configuration study). (A) Representative constructs illustrate the 5 different screw configurations evaluated. (B) Interfragmentary compression rose markedly whenever the screws placed into the second bone fragment were angled 30 degrees, whereas constructs with perpendicular screws in that fragment generated far lower compression. (C) Contact area displayed the same pattern, with the greatest increases observed when the distal screws were divergent. Bars depict group means ± SD; brackets denote significant pairwise differences with corresponding P values.
Cadaveric Second-TMT Arthrodesis Validation
Angling screws away from the fusion line significantly improved construct mechanics in the cadaver model. In the first cadaveric experiment comparing fully perpendicular (0 degrees) constructs vs constructs with all screws angled at 30 degrees (Figure 4A), paired samples analysis indicated a significant increase in interfragmentary compression for the 30-degree group (14.7-fold, 30 degrees: 49.4 ± 35.1 N vs 0 degrees: 3.4 ± 3.8 N; Fisher LSD P < .001; Figure 4B). Contact area was similarly enhanced in the 30 degrees constructs (3.8-fold, 30 degrees: 47.8 ± 28.9 mm² vs 0 degrees: 12.8 ± 7.3 mm²; Fisher LSD P < .001; Figure 4C).

Cadaveric first-TMT arthrodesis validation. (A, D) Fluoroscopic radiographs depicting constructs after final tightening. (B, E) Interfragmentary compression was substantially higher in the 30 degrees constructs than in the perpendicular controls, regardless of screw angle when fixing plate in first bone segment. (C, F) Contact area likewise increased when screws were angled, regardless of screw angle when fixing plate in the first bone segment. Bars show paired specimen means ± SD, and brackets indicate significant differences with corresponding P values.
In a separate set of paired cadaveric experiments, constructs with screws inserted perpendicularly into the cuneiform segment followed by screws angled at 30 degrees into the metatarsal segment were compared against fully perpendicular constructs (Figure 4D). When only the metatarsal screws were angled at 30 degrees (after securing the cuneiform screws at 0 degrees), constructs exhibited significantly greater interfragmentary compression (3.9-fold, 30 degrees: 118.1 ± 88.3 N vs 0 degrees: 30.3 ± 38.9 N; P < .001; Figure 4E) and increased contact area (2.0-fold, 30 degrees: 53.3 ± 19.1 mm² vs 26.2 ± 30.3 mm²; P < .001; Figure 4F) compared with the all-perpendicular fixation.
Discussion
The present investigation demonstrated that controlled screw divergence is an effective plate-based method for augmenting interfragmentary compression and contact area, and that the mechanical principles identified in foam surrogates translate to a cadaveric second-TMT fusion model. This follows basic vector geometry. Where prior reports address polyaxial interface mechanics1 -4,6 -8,11 -13,15,16,18 or present screw-only compression models and clinical series that do not isolate screw angle, 14 the present data address a distinct, construct-level question specific to plate-based midfoot arthrodesis. In series 1, compression and contact area increased sequentially from 0 to 15 degrees and from 15 to 30 degrees, illustrating the benefits of plate systems designed to accommodate secure/locking fixation at high screw angulation. Series 2 clarified the underlying mechanism: once the plate is fixed to the first fragment, angling screws as they engage the second fragment pulls the bone segments together and produces a substantial rise in compression and contact area.
The mechanical advantage of divergent screw fixation arises from the angled trajectory of screws relative to the plate and bone surface. When screws are placed perpendicularly, tightening predominantly compresses bone segments directly toward the plate, limiting the achievable interfragmentary compression. Conversely, angled screws generate both perpendicular and parallel force components; the parallel component draws bone segments together, increasing compression at the osteotomy or arthrodesis interface. However, effective compression depends on the screw angle configuration. Angling screws while initially securing the plate to the first bone fragment merely translates the plate along the bone without appreciably compressing the fragments. Only after rigid fixation of the plate to the first fragment does angulation of screws into the second fragment translate directly into interfragmentary compression.
Clinically, these mechanical principles have meaningful implications for midfoot arthrodesis and other procedures. Achieving sufficient interfragmentary compression and maximal contact area is essential for generating construct stability, promoting primary bone healing, and minimizing the risk of nonunion, which remains a prevalent concern in midfoot procedures. The substantial increases in compression and contact area demonstrated in this study suggest that selecting plating systems capable of accommodating secure, locked fixation at greater screw angles could directly improve fixation quality. Importantly, this biomechanical advantage can be realized without additional operative steps or instrumentation beyond conventional plate-and-screw techniques. Practically, surgeons may optimize fixation by first rigidly securing the plate to the initial fragment, then inserting screws at a divergent trajectory into the second fragment, thereby reliably drawing the bone segments together. Such an approach maintains simplicity and efficiency in the surgical workflow, and it avoids additional tissue disruption associated with alternative compression methods, such as lag screws. These results highlight an accessible and easily adopted method of improving fixation quality in midfoot arthrodesis procedures.
Several limitations of this investigation should be acknowledged. First, the study assessed only immediate postinsertion compression and contact area without examining the effects of cyclic or physiologic loading; thus, the durability of these mechanical benefits under clinical conditions remains uncertain. Second, foam bone surrogates may not precisely replicate the biomechanical properties or variations inherent to human bone. Although validation in a cadaveric second-TMT model addressed this limitation to some extent, bone density and quality were not specifically characterized in the cadaveric specimens, potentially affecting the generalizability of findings to patients with varying bone quality. Additionally, only a single 30-degree plate system was tested, and other plating systems with differences in geometry, screw-thread design, or screw length could yield different mechanical outcomes. Future studies should incorporate cyclic fatigue testing under physiologic loading conditions to evaluate the persistence of mechanical advantages. Clinical investigations are also needed to determine whether the substantial biomechanical improvements observed here translate into improved fusion rates, faster consolidation, and enhanced patient-reported outcomes in midfoot arthrodesis. We did not evaluate screw-plate interface bending or cyclic endurance; because off-axis locking performance can be mechanism- and angle-dependent, clinical application should remain within each device’s design envelope. As these are standardized immediate postinsertion benchtop measurements, absolute compression/contact magnitudes may overestimate clinical effects and require validation under physiologic loading. These experiments were not designed to compare plate platforms; any observed differences across plates could reflect uncontrolled design factors (geometry, screw thread design, locking interface), and the 30-degree plate findings represent an angle effect within a system indicated for that angulation rather than a plate-level superiority claim.
Conclusion
In this controlled benchtop study, with plate fixation, screw divergence increased interfragmentary compression and contact area, and these effects translated from foam surrogates to a cadaveric second-TMT model. Effectiveness depended on configuration, with divergence in the second bone fragment after securing the first fragment producing the largest gains. This follows basic vector geometry. Future clinical research will be necessary to determine how these biomechanical improvements influence patient outcomes and fusion success rates.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251386359 – Supplemental material for Screw Angulation and Insertion Sequence Increase Interfragmentary Compression When Using Plates for Midfoot Arthrodesis: Foam-Surrogate and Cadaveric Validation
Supplemental material, sj-pdf-1-fao-10.1177_24730114251386359 for Screw Angulation and Insertion Sequence Increase Interfragmentary Compression When Using Plates for Midfoot Arthrodesis: Foam-Surrogate and Cadaveric Validation by James Johnson, Leah Buch, Shannon King, Mia Knauf, Joshua Kim, Christopher Gross, Daniel Scott, Samuel Adams, Kenneth Dupont and David Safranski in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
This work was internally funded and completed by Enovis. Findings should be considered in the context of industry sponsorship; the authors had full access to the data and are responsible for the analysis and manuscript content.
Author Note
All work was performed at Enovis, Inc.
Ethical Considerations
Ethical approval was not sought for the present study because the study involved only cadaveric specimens without identifiable human data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was internally funded by Enovis.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James Johnson, PhD, Leah Buch, MS, Shannon King, MS, Mia Knauf, MS, Joshua Kim, Kenneth Dupont, PhD, David Safranski, PhD, report disclosures related to manuscript of paid employee of Enovis, a manufacturer of the plates studied in this work. Christopher Gross, MD, Daniel Scott, MD, Samuel Adams, MD, report disclosures related to manuscript of paid consultant of Enovis, a manufacturer of the plates studied in this work. Disclosure forms for all authors are available online.
Data Availability Statement
Data are available upon reasonable request to the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.