
Abstract
Background
Ankle fracture incidence is increasing in the elderly. There is a growing trend toward early weightbearing. We investigated the effects of early weightbearing after ankle open reduction and internal fixation (ORIF) in the geriatric population.
Methods:
A retrospective cohort study was performed of patients aged ≥65 years who underwent ankle ORIF at 3 neighboring community hospitals from 2015 to 2024. A total of 97 were included, with 52 undergoing syndesmotic fixation. Postoperatively, patients were 50% partial weightbearing for 2-3 weeks. Afterward, patients were permitted to bear as much weight as tolerable. Recorded outcomes included fracture union, radiographic maintenance of alignment, hardware failures, wound complications, hardware removals, and the need for repeat surgery.
Results:
Weightbearing as tolerated was initiated at an average of 16.6 days. All patients achieved fracture union without hardware failure, catastrophic loss of reduction (>2 mm displacement), accelerated posttraumatic arthritis, or need for revision surgery. Fourteen patients (14.4%) experienced minor complications not requiring return to surgery: 3 had delayed wound healing managed with protected weightbearing, 4 had surgical site infections treated with oral antibiotics, and 7 underwent elective hardware removal for symptomatic hardware at an average of 8.6 months postoperatively.
Conclusion:
This is the largest study to date reporting on the effects of early weightbearing in the geriatric ankle ORIF population. We report no major complications and a limited number of soft tissue–related complications. In a patient population with a known morbidity from prolonged immobility, and with advances in recent fracture fixation, we hope our data help build confidence in early postoperative weightbearing.
Level of Evidence:
Level IV, retrospective cohort study.
Introduction
In an increasingly older population, there is a corresponding increase in ankle fracture incidence and prevalence.6,11,14,19 Ankle fractures are the most common fracture of a weightbearing joint and account for 10% of all fractures seen in orthopaedics.2,16 Nearly 23% of ankle fractures in the United States between 2012 and 2016 occurred in individuals aged ≥60 years. 20 Although regarded by many as a simple injury, there are many controversies associated with ankle fracture management, including timing of weightbearing after open reduction internal fixation (ORIF). Postoperative recommendations range from no weightbearing for 8 weeks to immediate full weightbearing. Swart et al 24 discussed the wide variation in the period of postoperative nonweightbearing after fixation of ankle fracture without syndesmotic injury, with the average time of nonweightbearing varying from 4.9 to 7.6 weeks. Furthermore, the authors noted that surgeons recommended a prolonged period of nonweightbearing in geriatric patients.
There is a growing trend toward early weightbearing because of its advantages in rehabilitation and return to function. 22 Early weightbearing after ORIF of unstable ankle fractures is associated with reliable fracture healing without increased morbidity or loss of reduction and improved ankle motion and function.1,7 We previously expanded on these studies to include unstable ankle fractures requiring syndesmotic fixation in patients aged 18-65 years old. We found that early weightbearing as tolerated (WBAT) after ORIF of unstable ankle fractures with syndesmotic fixation was not associated with major comorbidities, higher rates of catastrophic failure, or increased wound issues. 17 However, there is insufficient data for early postoperative weightbearing after ankle ORIF in older populations, which is relevant in an aging population with known morbidity and mortality related to prolonged immobility, as evidenced in the hip fracture literature. 10 We evaluated the outcomes of early weightbearing after ORIF of unstable ankle fractures in a geriatric population. We hypothesized that early weightbearing in this population would not lead to radiographic or clinical failures of fracture union or wound complications.
Methods
Institutional review board approval was obtained for this retrospective chart review. We collected data from 3 community hospitals to identify all patients ≥65 years old with isolated unstable ankle fractures treated with ORIF between September 2015 and June 2024. Unstable ankle fracture was defined as a trimalleolar facture, or a displaced bimalleolar or lateral malleolar fracture with increased static widening of the clear spaces or dynamic widening with stress or weightbearing on radiographs. Patients with syndesmotic fixation were included in the study. Patient demographics, comorbidities, Lauge-Hansen classification, concomitant injuries, method of fixation, time to surgery, time to weightbearing, follow-up time, and adverse events were recorded. Patients were excluded if they had concomitant injuries that affected weightbearing status, open fractures, revision cases, peripheral neuropathy or other neurologic injury to the affected extremity, dementia, seizure disorders, failure of wound healing within first 2 weeks postoperatively prior to the initiation of weightbearing, or polytrauma (Table 1). Patients with sensory intact, nonneuropathic type 2 diabetes mellitus that was well controlled with oral medications (HbA1c <7%) were included. Patients with fractures that involved 25% or more of the distal tibia weightbearing articular surface were also excluded because these were considered pilon equivalent fractures and were not allowed to weightbear early. The threshold for 25% articular involvement was estimated using clinical evaluation of lateral radiographs by drawing a line from anterior to posterior to determine where the fracture plane entered on the posterior cortex. A CT scan was also evaluated if it was available. Although Maisonneuve injuries are considered ligamentous, syndesmotic injuries, they are primarily concerned with disruption of the syndesmosis and deltoid ligaments as opposed to a syndesmotic injury that results from a rotational ankle fracture. Maisonneuve injuries may limit fibula fracture length stability because operative fixation of the proximal fibula fracture is uncommon, compared with a pronation-external rotation (PER) IV ankle fracture in which the fibula is fixed to length. Thus, Maisonneuve injuries and “log splitter” injuries, which we consider a variant of Maisonneuve injuries, were excluded from this study.
Inclusion and Exclusion Criteria.

Abbreviation: ORIF, open reduction and internal fixation.
Using the above criteria, we identified 112 patients who sustained unstable ankle fractures between September 2015 and June 2024. Fifteen of these patients were excluded for the following reasons: 4 for peripheral neuropathy, 2 for Maisonneuve injury, 3 for revision cases, and 6 for pilon equivalent fractures. The remaining 97 patients who met inclusion criteria underwent ORIF for their unstable ankle fractures. Of these, 52 patients had syndesmotic injuries requiring fixation. The fracture pattern demographics were tabulated (Table 2).
Fracture Pattern Demographics. a
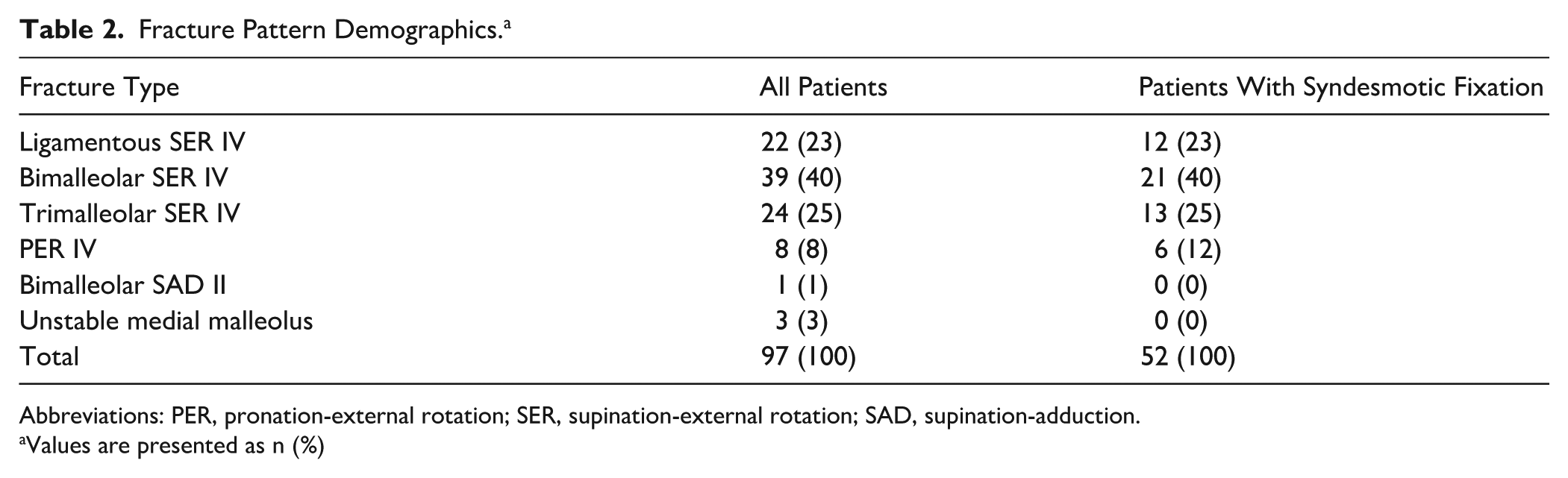
Abbreviations: PER, pronation-external rotation; SER, supination-external rotation; SAD, supination-adduction.
Values are presented as n (%)
At least 1 of 3 senior surgeons was involved in all cases. Fibula fracture fixation consisted of neutralization plates, bridging plates, or intramedullary nails. Only 1 patient received an intramedullary nail. Plates used included one-third tubular, recon, and anatomic distal fibula plates with locking and nonlocking screws. One fibula fracture sustained significant comminution and necessitated the addition of bone graft. Medial malleolus fractures were fixed with 4-mm cannulated screws, one-third tubular plates, cortical screws, or nonlocking intramedullary screws. No hook plates were used to fix any of the medial malleolus fractures. For posterior malleolus fracture fixation, locking plates or posterior-to-anterior 4.0-mm cannulated screws were applied. Patients with positive intraoperative external rotation stress test and Cotton test, as indicated by widening of the syndesmosis, underwent syndesmotic fixation, which was achieved with one, two, or three 3.5-mm or 4.0-mm syndesmotic screws, 1 or 2 suture button constructs, or a combination of screws and buttons (Figure 1). One patient underwent deltoid ligament repair. Patients were placed in well-padded, 3-sided splints and were made “limited to” 50% partial weightbearing for 2-3 weeks to allow for incisional healing. No patients were made immediate WBAT. After adequate incisional healing, sutures were removed and patients were transitioned to WBAT in a controlled ankle motion (CAM) walker boot or in a short leg walking cast (SLC) based on surgeon preference. Two authors used the boot and 1 used the SLC, with 49 patients using an SLC. We did not quantify the amount of weightbearing. However, we instructed our patients to weightbear as much as they could tolerate and to use gait aids as needed.

An illustrative case of a patient who was included in the study. The patient sustained (A) an unstable ankle fracture without dislocation that (B) needed ORIF with syndesmotic fixation. (C) The patient participated in early weightbearing postoperatively and went on to heal their ankle fracture.
Patients were followed postoperatively for clinical and radiographic outcomes. Outcomes included fracture union, radiographic maintenance of alignment, hardware failures, wound complications, and the need for repeat surgery.
Fracture union was defined as visible bridging callus with a lack of obvious fracture line as identified on radiographs, combined with no evidence of clinical examination tenderness or persistent swelling. Time to union was not measured because we did not have a long enough follow-up time to measure union. We did not apply inclusion or exclusion criteria related to a minimum follow-up time. All 3 senior authors reviewed all patients’ radiographs, which were also reviewed by 2 residents and 1 fellow to determine radiographic maintenance of alignment. All reviewers were blinded when evaluating radiographs. Catastrophic failure or loss of reduction was defined as fracture displacement or syndesmotic widening by more than 2 mm. Results were tabulated for all patients into one group, and for patients with syndesmotic fixation into a second group. Missing data were excluded from calculations such as for averages and SDs. Follow-up visits varied by surgeon preference but generally were conducted at 2-3 and 6 weeks and at 3, 6, and 12 months postoperatively, with weightbearing radiographs obtained after the 2-3-week initial postoperative visit. Not all patients completed all follow-up appointments at these time points, but patients were followed for as long as possible.
Results
Of the 97 patients included in the study, 75 (77%) were female (Table 3). The average age was 74.8 (range, 64.6-94; SD, 7.7) years, and average BMI was 26 (range, 16.6-39.3). Eight patients (8%) were type 2 diabetics, and 5 (5.3%) were smokers (Table 3). Eight patients had unknown smoking status, and 8 were without BMI data. The average time to incisional wound healing and initiation of WBAT was 16.6 (range, 12-28; SD, 3.8) days with a median of 15 days postoperatively. Patients followed up for an average of 196.8 (range, 41-739; SD, 154) days with a median of 153 days. The fracture patterns included 22 ligamentous SER IV, 39 bimalleolar SER IV, 24 trimalleolar SER IV, 8 PER IV, 1 bimalleolar SAD II, and 3 unstable medial malleolus fractures.
Separate and Grouped Results. a

Abbreviations: BMI, body mass index; WBAT, weightbearing as tolerated.
Values are presented as n, n (%), or average (range).
None of the patients had major complications, which constituted hardware failure or migration as seen radiographically, loss of reduction or alignment, need for revision or accelerated posttraumatic arthritis. All 97 patients achieved uneventful union and maintained fixation of the fractures as seen at their last follow-up visits. None of the patients developed wound dehiscence or hardware exposure. No patients were using CAM boots or bracing as of last follow-up. However, 14 patients (14.4%) had minor postoperative complications. Minor complications were defined as those complications that did not necessitate a return to the operating room. Three of these patients had delayed wound healing that was treated with a period of protected weightbearing to prevent progression of wound issues, in which they remained in a CAM boot and engaged in limited activity with regular dry dressing changes for a period of 2-6 weeks until the wounds healed. Four patients had surgical site infections that resolved with a single course of oral antibiotics, and 1 of these patients also later underwent hardware removal for symptomatic hardware. Seven patients underwent hardware removal, 6 of which were for symptomatic hardware on average at 8.6 months after the index surgery; the seventh patient had a loosened screw that was removed in clinic. Stratifying the minor complications by fracture classification shows that 2 (9.1%) of the 22 patients with ligamentous SER IV developed minor complications, as did 7 (17.9%) of the 39 bimalleolar SER IV, 3 (12.5%) of the 24 trimalleolar SER IV, and 2 (25%) of the 8 PER IV (Table 4).
Results for Patients With Minor Complications.
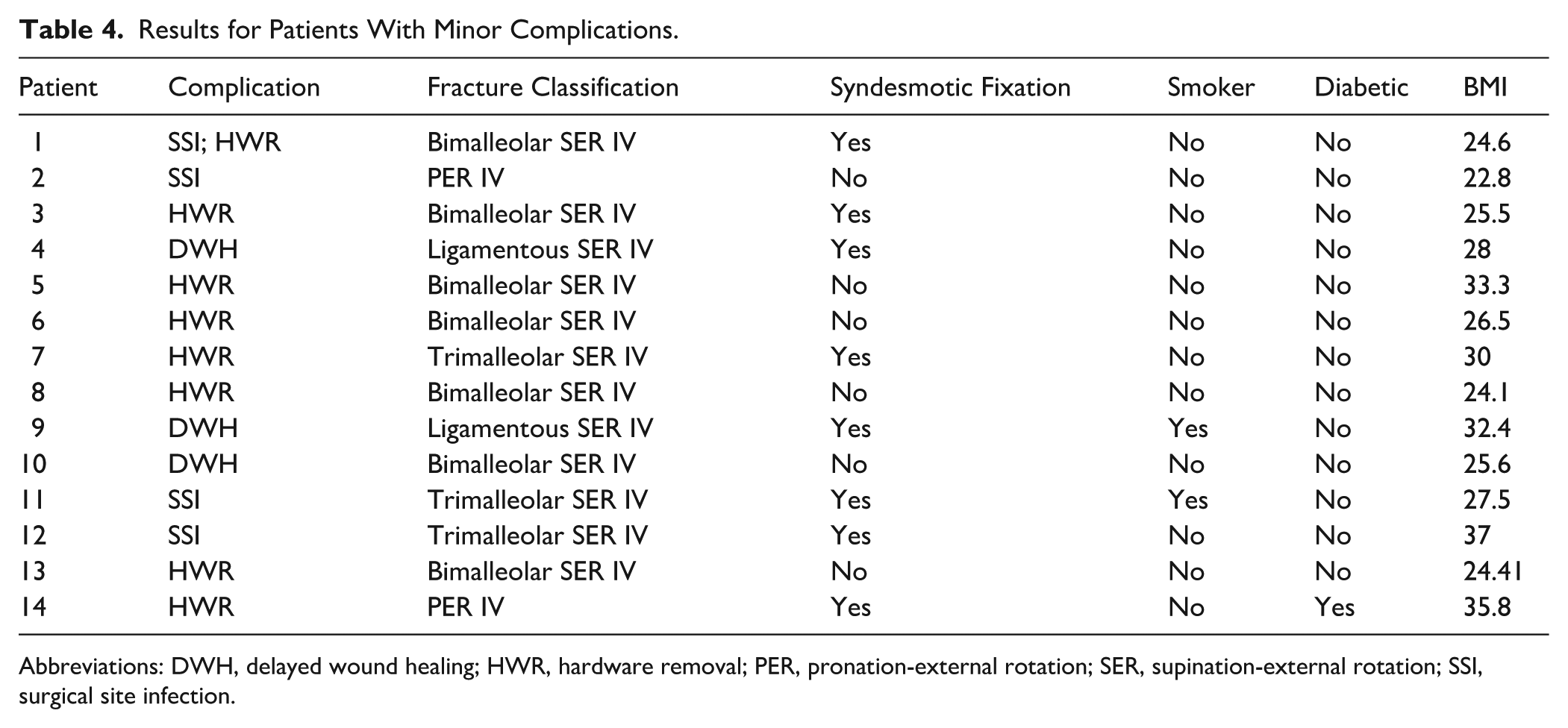
Abbreviations: DWH, delayed wound healing; HWR, hardware removal; PER, pronation-external rotation; SER, supination-external rotation; SSI, surgical site infection.
Of the 97 patients, 52 (53.6%) underwent syndesmotic fixation. Forty of these patients (77%) were female. The average age was 75 (range, 64.6-88; SD, 7) years. The average BMI was 26 (range, 16.6-37). Five patients (9.6%) had type 2 diabetes, and 4 (7.7%) were smokers. The average time to incisional wound healing and initiation of WBAT was 17.2 (range,12-28; SD, 4.2) days, with a median of 15 days postoperatively. Patients were followed up for an average of 205 (range, 42-724; SD, 150) days, with a median of 160 days. The fracture patterns within this subgroup were tabulated as follows: 12 ligamentous SER IV, 21 bimalleolar SER IV, 13 trimalleolar SER IV, 6 PER IV, 0 bimalleolar SAD II, and 0 unstable medial malleolus fractures.
Within the syndesmotic fixation subgroup, 8 (15.4%) patients had minor complications. Two patients had delayed wound healing. Three patients had surgical site infections, with 1 of these also undergoing hardware removal. Three underwent removal of symptomatic hardware on average at 5.7 months postoperatively. By fracture pattern classification, the rate of minor complications is as follows: 2 (16.7%) of 12 ligamentous SER IV, 2 (9.5%) of 21 bimalleolar SER IV, 3 (23.1%) of 13 trimalleolar SER IV, and 1 (16.7%) of 6 PER IV.
Discussion
This study demonstrates that early weightbearing after ORIF of unstable ankle fractures is safe in geriatric patients, with all patients achieving reliable fracture union without loss of alignment or hardware failure. 17 Our findings support the growing body of evidence favoring early mobilization protocols.2,20,21,23 Previous studies in younger populations have shown that early weightbearing results in reliable fracture healing and improved functional outcomes. Dehghan et al 7 reported that patients allowed to weightbear at 2 weeks postoperatively had superior ankle range of motion, function, and quality of life scores compared to those with delayed weightbearing after 6 weeks, although their study excluded patients with syndesmotic injuries and those aged ≥62 years.Our study extends these findings to a geriatric population and includes patients with syndesmotic fixation.
Bretherton et al 3 compared the Olerud-Molander Ankle Score (OMAS), health-related quality of life outcomes, rates of complications, and cost-effectiveness in patients who underwent ankle ORIF and were randomly assigned to early (2 weeks) vs delayed weightbearing (6 weeks). The complication rates were similar between the 2 groups, but the early weightbearing group was associated with improved OMAS and health-related quality of life outcomes, and reduced costs and productivity losses. This study did not capture patients older than 62 years. Park et al 15 showed that early postoperative weightbearing at 2 weeks was not inferior to delayed weightbearing at 6 weeks when comparing OMAS at 12 months postoperatively. Early weightbearing in this study was associated with shorter return to preinjury activity. Patients older than 65 years and those with syndesmotic injuries were excluded from this study.
With this trend toward early weightbearing, it is important to also address how this applies to a geriatric population because there is no established timeline of postoperative weightbearing after ankle ORIF in older populations. Furthermore, ankle fractures are common among geriatric patients and will continue to increase in incidence. Between 2012 and 2016, nearly 1 in 5 ankle fractures in the United States occurred in individuals 60 years or older. 20 As is well known in the orthopaedic community, prolonged immobility is associated with known morbidity and mortality across the general population and especially in an aging population. We must therefore evaluate the safety of early weightbearing after ankle ORIF for unstable ankle fractures in a geriatric population.
We demonstrate that geriatric patients who underwent early postoperative weightbearing after ankle ORIF had no major complications or catastrophic early failure, and a low incidence of minor adverse outcomes. This corresponds to our previous study in which patients between the ages of 18 and 65 years who underwent ankle ORIF with and without syndesmotic fixation were allowed to weightbear at 2-4 weeks postoperatively, and also did not experience any major complications or catastrophic early failure. Similar to our geriatric population, the population from our previous study experienced a relatively low incidence of minor adverse outcomes. The overall rate of minor complications in our study vs the previous study was 14% vs 13%. Both studies had similar inclusion and exclusion criteria with the exception of the age difference, inclusion of non-neuropathic patients with well-controlled diabetes, and minimum follow-up time. Although this current study did not have a minimum follow-up time, on average the patients for this study were followed up for 6.6 months. Across both studies, the methods of fixation, implants used, and operating senior surgeons were also kept the same.
It is interesting to note that the rates of complications across the 3 groups in our current study are similar. The literature shows that syndesmotic ankle fractures are generally more severe, higher-energy injuries associated with poorer functional outcomes when compared to injuries without syndesmotic disruption.4,8,12,18 For these reasons and because of the fear that excessive loading after fixation could potentially result in catastrophic failure or need for revision surgery, patients with syndesmotic injuries are generally managed more conservatively with longer periods of nonweightbearing.9,16,17,24 However, in our study, we see that patients who underwent syndesmotic fixation had a similar rate of minor complications when compared to patients without syndesmotic fixation and to the group of all patients. Early postoperative weightbearing after ankle ORIF is relatively safe in geriatric patients with and without syndesmotic injuries.
It is also important to address that we included patients with vibratory sensory intact, non-neuropathic type 2 diabetes mellitus that was well controlled with oral medications (HbA1c <7%). These patients did not have an increased rate of minor complications compared with nondiabetic patients. Of the 14 patients with minor complications, only 1 was diabetic. Among the smokers, 40% developed minor wound complications, reinforcing the role that smoking plays in impaired wound healing (Table 4). 13
To our knowledge, this is the largest study to date in which geriatric patients were able to weightbear early after ankle ORIF. Coscia et al 5 showed that immediate WBAT after ankle ORIF in a geriatric population is not associated with increased hardware failures or postoperative complications. This study, however, was limited to 44 patients. Other strengths of our study are that our patient population included diabetics, smokers, syndesmotic fixation, multiple modes of fixation of syndesmotic and malleolar injuries with varying implants, varying types of ankle fractures, posterior malleolar fixation, multiple surgeons, multiple surgery centers, and a broad age range, with the only limitation being a minimum of 65 years old. With these varying demographics, our outcomes can be generalized to an aging population and to patients with syndesmotic injuries, which currently are generally managed with prolonged periods of weightbearing.
This study has several important limitations. The retrospective design without a control group limits our ability to establish causality or compare outcomes to delayed weightbearing protocols. We lacked formal power analysis and validated functional outcome measures, focusing instead on radiographic and clinical parameters. The absence of minimum follow-up criteria, although allowing larger patient capture, may have missed late complications. Additionally, we did not quantify actual weightbearing loads or patient compliance with the protocol. Rather, we discussed with the patients that they could weightbear as much as they could tolerate. The inclusion of multiple surgeons and institutions, while improving generalizability, introduced potential variability in surgical technique and postoperative management. Finally, the relatively short follow-up period (average 6.6 months) may not capture long-term complications such as posttraumatic arthritis.
Future areas of research would include a prospective randomized controlled trial with adequately powered control and treatment groups, as well as including long-term follow-up results to evaluate for late events and outcomes. Other areas of future research could also include allowing for immediate WBAT, establishing a methodology to detect small but significant loss of reductions, showing benefits of early WBAT, and establishing a methodology for identified patients who are “at risk” for loss of reduction after early WBAT. Outcomes that we did not evaluate and would address in future studies would include functional outcomes, ankle range of motion, and 36-Item Short Form Health Survey (SF-36) questionnaires to objectively evaluate outcomes of early weightbearing in a geriatric population. However, this study does display that it is safe to start advancing weightbearing earlier than we have in the past for this patient population.
Conclusion
This retrospective cohort study of 97 geriatric patients demonstrates that early weightbearing protocols (initiated at average 16.6 days) can be safely applied following ORIF of unstable ankle fractures without compromising fracture healing or alignment. No major complications or hardware failures occurred, with only 14.4% experiencing minor complications not requiring surgical intervention. Given the established morbidity associated with prolonged immobility in elderly patients, particularly as demonstrated in hip fracture literature, these findings support confidence in early weightbearing protocols for this vulnerable population. Early mobilization may improve quality of life and reduce immobility-related complications while maintaining fracture stability. Future prospective studies with control groups and validated functional outcomes are needed to confirm these findings.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114251373087 – Supplemental material for Early Weightbearing Following Open Reduction and Internal Fixation of Unstable Ankle Fractures in a Geriatric Population: A Retrospective Cohort Study
Supplemental material, sj-pdf-1-fao-10.1177_24730114251373087 for Early Weightbearing Following Open Reduction and Internal Fixation of Unstable Ankle Fractures in a Geriatric Population: A Retrospective Cohort Study by Valerie Carbajal, Brent Kokubun, Peyton Keeling, Daniel Choi, Casey Pyle, Arash Aminian, David Lee and Thomas G. Harris in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Approval
Ethical approval was not sought for the present study because this study is a retrospective chart review study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas G. Harris, MD, reports disclosures related to manuscript of consultant for Arthrex with Royalties, IP; royalties for Globus Medical; royalties for Paragon 28 and general disclosures of associate/specialty editor for FAI; Reviewer for Techniques in Foot Surgery, JBJS, Foot and Ankle Specialist. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.