
Abstract
Background:
The purpose of this study was to determine the impact of surgeon volume on outcomes following ankle fracture fixation.
Methods:
Over 7 years, 362 patients who met inclusion criteria (>18 years with rotational ankle fractures) were identified and treated by orthopaedic surgeons at several hospitals within an academic medical center and were retrospectively reviewed. Surgeons that completed less than 24 ankle fixations per year (<90th percentile) during the study period were classified as low-volume (LV) and surgeons completing 24 or more ankle fixations per year (>90th percentile) were classified as high-volume (HV). Chart review was conducted to gather data regarding perioperative, radiographic, inpatient, and long-term outcome data (average 12-month follow-up).
Results:
One hundred thirty-four patients (37.0%) were treated by LV surgeons and 228 (63.0%) were treated by HV surgeons. Although both cohorts had a similar breakdown of fracture patterns (P = .638), the LV cohort had a greater incidence of open fractures (P = .024). No differences were found regarding wait time to surgery, surgery duration, and LOS. Radiographically, more patients in the HV cohort achieved anatomic mortise after surgery (96.5% vs 89.6%, P = .008). Patients in the LV cohort took longer to heal radiographically (4.27 ± 2.4 months vs 5.59 ± 2.9 months, P < .001), and also had higher rates of reoperation and hardware removal (P < .05). Lastly, all cost variables were lower for high-volume surgeons (P < .05).
Conclusion:
In this single-center study, we found that patients treated by LV surgeons took 30% longer to heal radiographically and had greater reoperation rates than those treated by HV surgeons. Additionally, patients treated by high-volume surgeons had more anatomic postoperative radiographic ankle mortise reductions and was less cost-effective than when performed by high-volume surgeons.
Level of Evidence:
Level III, retrospective comparative study.
Keywords
Introduction
Ankle fractures are the fifth most common adult fracture type, with an incidence of 187 fractures per 100,000 persons per year.12,13,17,22 The occurrence of these fractures is on the rise, particularly in female and elderly patient populations.18,21,23,25,37 These fractures often prove difficult to treat given the complex bony anatomy, the ligamentous attachments, and the functional ability required for patient satisfaction.3,25,32 Common adverse outcomes associated with ankle fracture repairs include poor wound healing, infection, DVT, nonunion, secondary displacement, refracture, stiffness, muscular atrophy, tendon insufficiency, sensory deficit, and tarsal tunnel syndrome. 27 Multiple studies have demonstrated that patients report functional limitations up to 2 years following their ankle fracture surgery, with many patients never returning to the same level of sporting activities.7,20,31
It is well understood that surgeon volume correlates with improved outcomes.4,9,16,24,29,34,35 This has been demonstrated extensively in the hip and knee replacement literature.4,24,29,34,35 Shervin et al conducted a systematic review and found that higher hospital and surgeon volumes were associated with lower rates of hip dislocation following hip arthroplasty. 35 From a financial standpoint, Padilla et al found that arthroplasty-trained surgeons achieved lower costs during total hip arthroplasty than non–arthroplasty-trained orthopaedic surgeons. 29 Beyond the scope of arthroplasty, one study found that reconstructive surgeons with higher case volumes had fewer complications and greater success following long bone nonunion repair. 16
Although most studies support the notion that surgeon volume correlates with favorable outcomes, a few studies looking at isolated surgical procedures have found no difference, especially when analyzing the outcomes between specific fellowship-trained surgeons.5,33 A prospective analysis found no alteration in outcomes of intramedullary nail fixation of diaphyseal femur fractures between trauma and nontrauma fellowship-trained surgeons. 5 Similarly, another study found no difference in outcomes between arthroplasty and non–arthroplasty-trained surgeons for total hip arthroplasty. 33 To date, no study has directly examined the long-term outcomes based on surgeon volume of patients who undergo open reduction and internal fixation for a rotational ankle fracture. Therefore, the purpose of this study was to determine if surgeons performing more frequent ankle fracture fixation procedures have greater quality and improved long-term outcomes than surgeons performing the same procedures less frequently.
Methods
A retrospective review was conducted to identify patients who underwent an open reduction and internal fixation for a rotational ankle fracture at several hospitals within an academic medical center between January 2013 and September 2020. Inclusion criteria included patients greater than 18 years of age presenting for surgical fixation of a rotational ankle fracture (AO/OTA type 44). Exclusion criteria included patients who received any preliminary surgery at an outside hospital, ununited ankle fracture surgeries, pilon fractures, polytrauma, patients who followed up at an outpatient clinic site outside of the hospital’s electronic medical record network, and those who had less than 6 months’ follow-up. Furthermore, if a surgeon performed ankle fracture surgeries at hospitals outside of our system (no access to data) that would place them in the high-volume range, they and their patients were excluded from analysis to avoid inclusion of their patients in the lower-volume group. Of the 752 treated during the study period, 362 patients met these criteria and were treated by one of 21 board-certified orthopaedic surgeons within a single department.
To assess the impact of surgeon volume on patient outcomes, the 21 orthopaedic surgeons who treated the patients over those 7 years were labeled as either “high volume” (HV) or “low volume” (LV). In order to quantify “high volume” vs “low volume,” we chose to look at number of cases/year percentiles. Surgeons that performed below the 90th percentile (<24 ankle fracture fixations per year) were classified as low volume (LV) with a mean 17 ankle fracture repairs/year and surgeons that performed at or above the 90th percentile (>24 ankle fracture fixations per year) were classified as HV with a mean 29 ankle fracture repairs/year. Patients were subsequently grouped into either an HV or LV cohort depending on their treating surgeon. The particular subspecialty of the surgeon and number of years post-fellowship were also identified and recorded.
A retrospective chart review was conducted to gather data regarding perioperative, radiographic, inpatient, and long-term outcome data. The retrospective chart review was conducted by 2 independent observers not involved with patient care. Demographic information collected included age at time of injury, sex, body mass index (BMI), and Charlson Comorbidity Index (CCI). Additional information collected included fracture location, presenting soft tissue condition (open vs closed fracture), and whether syndesmotic fixation was needed.
Two independent orthopaedic surgeons, who were unaware to the specialty of the operating surgeon, reviewed all postoperative radiographs to assess the accuracy of the mortise reduction, identify construct patterns, and hardware irregularities, if any. Additional information collected included time to surgery from initial injury presentation; procedure duration (incision start to incision close); length of hospital stay; rate of anatomic mortise reduction after surgery; whether transsyndesmotic screws were used, and if so, how many; transsyndesmotic suture button use; and any repositioning during surgery.
At follow-up, 1 fellowship-trained orthopaedic surgeon and 1 orthopaedic trauma researcher without knowledge of treating surgeon reviewed all postoperative radiographs to determine anatomic ankle mortise reduction using the following criteria: resting talar tilt <3 degrees, syndesmotic widening ≤6 mm, medial clear space <5 mm, and medial malleolar congruity. All images reviewed were of the same views, the ankle trauma series: anteroposterior, lateral, and oblique. All images taken were nonweightbearing. Additional outcome data collected at follow-up included mortise malalignment (resting talar tilt ≥3 degrees, syndesmotic widening >6 mm, medial clear space widening ≥5 mm, and medial malleolar incongruity), time to radiographic bony union, the development of any complications, 90-day readmission, unplanned reoperation, and need for removal of hardware. Wound complications were defined as the presence of any superficial skin breakdown, deep wound infection, or delayed wound healing. Ankle range of motion parameters collected with a goniometer at follow-up included ankle dorsiflexion and ankle plantarflexion and are reported for the latest follow-up date.
Lastly, institutional cost data for ankle fracture fixation was obtained for all years (2013-2020) during our study period. Specific data points collected included variable direct costs, fixed direct costs, fixed indirect costs, and total costs (sum of variable direct, fixed direct, and fixed indirect costs). Direct costs are directly related to patient care. Variable direct costs are those that vary with patient activity, such as laboratory tests, medications, surgical supplies, and nursing expenses. In contrast, fixed direct costs do not vary with patient activity (ie, salaries, equipment, maintenance-related expenses, facilities, utilities). Indirect costs are hospital costs that cannot be identified either with a particular patient or a particular department of the hospital, such as general administration, health records, information technology, human resources, and volunteer services.6,11,36 Cost data at our institution is proprietary and thus is reported as baseline and a percentage comparison.
Statistical comparisons were generated through χ2 tests for categorical variables and independent t tests tests and Mann Whitney U tests for numerical variables using IBM SPSS Statistics, version 26 (IBM Corporation, Armonk, NY), assess if there were differences in patient treatment, inpatient course, or long-term outcomes between high-volume and low-volume orthopaedic surgeons.
Results
Of the 752 patients who underwent an open reduction and internal fixation for a rotational ankle fracture at several hospitals within a single academic medical center between January 2013 and September 2020, a total of 362 patients met our inclusion criteria and had a mean 12 months of follow-up. Two hundred twenty-eight patients (63.0%) were treated by an HV surgeon (mean 29 procedures/year), and 134 (37.0%) patients were treated by an LV surgeon (mean 17 procedures/year). Of the 21 board-certified orthopaedic surgeons who treated the patients within our study cohort, 2 surgeons were categorized as HV and the remaining 19 were categorized as LV.
Within the 2 cohorts, a breakdown of the providing surgeon’s subspecialty was reviewed and recorded (Table 1). Within the HV cohort, all 288 (100%) patients were treated by 2 orthopaedic traumatologists. Within the LV cohort, 34 (25.4%) patients were treated by an orthopaedic Foot & Ankle specialist, 18 (13.4%) were treated by an orthopaedic traumatologist, 54 (40.3%) were treated by an orthopaedic sports specialist, and 28 (20.9%) were treated by an orthopaedic hip and knee specialist. There was a difference between the 2 cohorts in regard to the providing surgeon’s subspecialty (P < .001). However, there was no difference in number of years postfellowship between the HV and LV surgeons (23.00 ± 0.0 years vs 19.42 ± 11.8 years) (P = .679).
Subspecialty breakdown of surgeons within high and low volume cohorts.
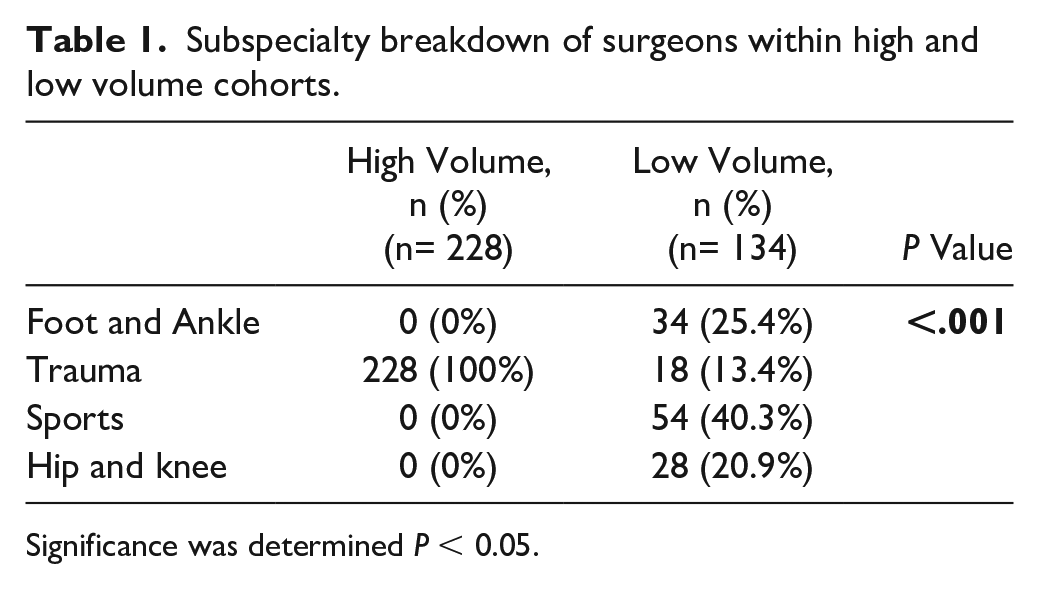
Significance was determined P < 0.05.
Demographic comparisons of the 2 cohorts are provided in Table 2. The 2 cohorts were similar in sex, age, BMI, and CCI (P > .05). Additionally, there was no difference between the 2 cohorts in regard to fracture pattern (P > .05), with most patients in both the HV and LV cohorts presenting with a trimalleolar fracture (50.9% and 43.3%, respectively). There was also no difference between the 2 cohorts as to whether syndesmotic fixation was needed during operative repair (P > .05). The 2 cohorts did differ in terms of presenting soft tissue condition, with more patients in the LV cohort initially presenting with an open fracture (P = .024).
Demographic information of patients treated.

Significance was determined p < 0.05.
Surgical parameters of the 2 cohorts are provided in Table 3. There was no difference between the 2 cohorts in wait time to surgery (P > .05). Additionally, no differences were found between the 2 cohorts in regard to surgery duration, as well as length of hospital stay (P > .05).
Surgical details of operative treatment of patients.

Significance was determined P < 0.05.
Radiographically, more patients in the HV cohort achieved an immediate and late postoperative anatomic mortise reduction than did patients in the LV cohort (96.5% vs 89.6%, P = .008). For those 22 patients graded as having 1 or multiple components of mortise malalignment (nonanatomic mortise reduction), 6 (27.3%) had excessive talar tilt (6.72 ± 2.8 degrees), 6 (27.3%) had medial clear space widening (5.50 ± 0.2 mm), 5 (22.7%) had syndesmotic widening (6.30 ± 0.3 mm), and 8 (36.4%) had a medial malleolar irregularity.
Additionally, although a transsyndesmotic screw use was more common in the HV cohort (49.1% vs 20.9%, P < .001), surgeons in the LV cohort used a greater number of screws when screws were used to repair the syndesmosis (1.63 ± 0.6 vs 1.31 ± 0.5, P = .003). Furthermore, transsyndesmotic suture button use (Tightrope; Arthrex, Naples, FL) was more commonly used in the LV cohort (19.4% vs 0.9%, P < .001). Lastly, patient repositioning during surgery was more common in the HV cohort (P < .001). The differences seen in surgical technique likely represent differences in training and preferences.
Outcomes obtained at latest follow-up are provided in Table 4. Average follow-up was 12.31 (range 6-19) months in the HV cohort and 13.13 (range 6-20) months in the LV cohort (P = .330). Radiographically, patients in the LV cohort took longer to heal than did patients in the HV cohort (5.59 ± 2.9 months vs 4.27 ± 2.4 months, P < .001). Additionally, there were no differences between the 2 cohorts regarding ankle dorsiflexion and plantarflexion at latest follow-up (P = .113, .560).
Outcomes of patients treated.
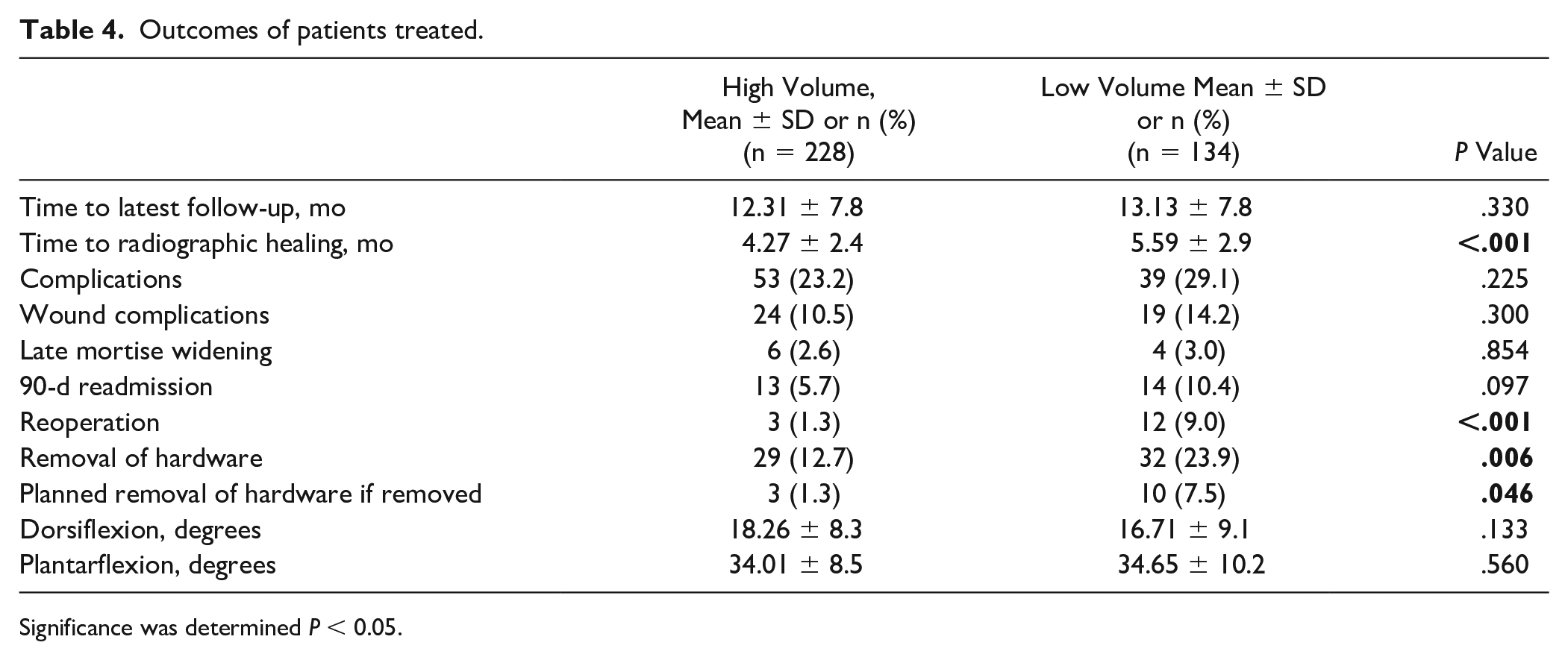
Significance was determined P < 0.05.
Patients in the LV cohort had a greater rate of reoperation than did patients in the HV cohort (9.0% vs 1.3%, P < .001). Within the HV cohort, 3 patients (1.3%) underwent reoperation. Two of these reoperations were incision and drainage procedures for wound infections, and the other reoperation was an ankle arthroscopy procedure. Within the LV cohort, 12 patients (9.0%) underwent reoperation. Seven of these reoperations were incision and drainage procedures for wound infections, 4 were revision procedures secondary to loss of reduction, and 1 was an arthroscopic ankle procedure along with tendon repair procedure.
Of note, operations for removal of hardware were not included in the analysis as an unplanned reoperation surgery. With that said, patients in the LV cohort underwent more hardware removal procedures than did patients in the HV cohort (23.9% vs 12.7%, P = .006). Of the patients that underwent removal of hardware, more of the removal procedures in the LV cohort were planned when compared to the HV cohort (7.5% vs 1.3%, P = .046). Lastly, no differences were found between the 2 cohorts when examining overall complication rates, wound complications, late mortise widening, and 90-day readmission rates.
Lastly, cost data obtained throughout the duration of our study period (2013-2020) is reported in Table 5. Total cost per procedure was 13% greater for low-volume surgeons compared with high-volume surgeons (P < .011). Additionally, all subsets of cost, variable direct costs, fixed direct costs, and fixed indirect costs were also significantly higher for low-volume surgeons when compared to high-volume surgeons (P < .05).
Cost differences between patient cohorts.
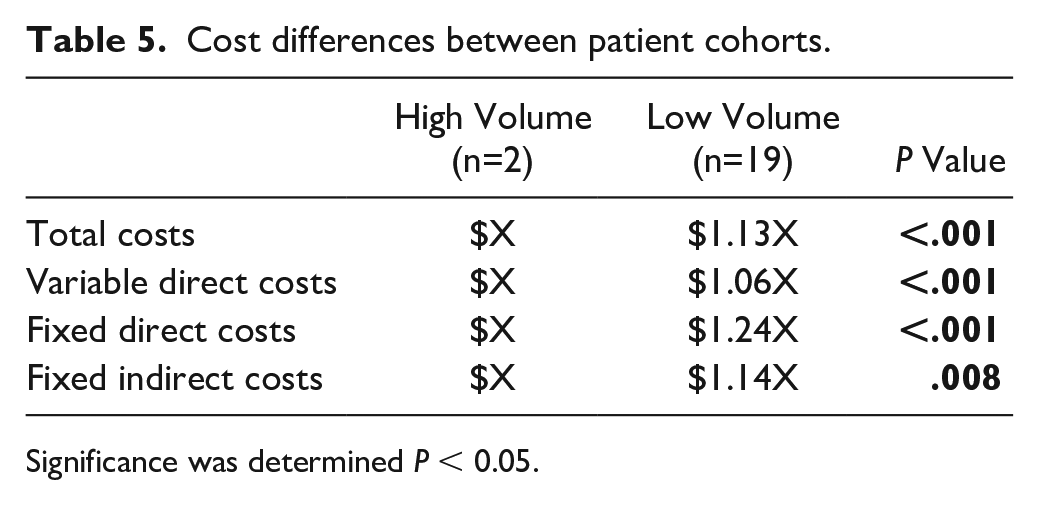
Significance was determined P < 0.05.
Discussion
Although the surgical details were similar among both cohorts, the results of our study demonstrated that patients treated by low-volume surgeons experienced longer healing times and had greater rates of both planned and unplanned reoperation than those treated by high-volume surgeons. Patients treated by high-volume surgeons also achieved better postoperative radiographic mortise reductions, which may have long-term implications for function. Additionally, our results clearly demonstrate that high-volume surgeons can perform the same ankle fracture fixation procedures with greater cost efficiency than can low-volume surgeons.
It is long understood that hospital volume and surgeon case volume correlate with improved outcomes following various orthopaedic surgeries.4,9,16,24,29,34,35 In orthopaedic residency programs, the average total number of cases logged per resident increased 17.4% from 2007 to 2013. 19 Even though trainees are gaining more experience overall, residents in the 90th percentile for case exposure consistently log more cases than those in the 10th percentile, showing that there remains a discrepancy in surgical experience among orthopaedic residents.14,23 The ACGME requires each orthopaedic resident to complete a minimum of 1000 but no more than 3000 cases. 1 Moreover, they require a minimum of 15 ankle fracture fixation cases throughout residency training. 1 Given this minimum, a resident aiming to subspecialize in a field other than trauma or foot and ankle may choose to bolster their case logs elsewhere. Although this can benefit the resident as they pursue a subspecialty, a lack of broad, continued medical training could diminish their skills in other orthopaedic areas. In a recent study on simulation-based arthroscopic surgical training for orthopaedic residents, it was found that simulation training improves performance, but the skills dissipate in the absence of continued training. 15 In this study, the skills were diminished after 1 year of no simulation-based practice. Thus, it can be expected that orthopaedic surgeons who do not regularly perform certain procedures may not maintain their surgical skill sets.
Beyond the scope of residency training, it is important to consider the impact of fellowship on orthopaedic surgical experience. Butler et al 8 compared the number of trauma cases logged in 1 year of trauma fellowship compared with 4 years of orthopaedic residency. They found that physicians reported an average of 75 leg and ankle fracture reductions in 1 year of trauma fellowship, compared to 95 over 5 years of residency. Not only is there greater specialization in fellowship, but case complexity increases as well. The same study showed that the average volume of open, complex fracture reductions was 134 during 1 year of fellowship vs 48 in 5 years of residency. 8 Accordingly, postfellowship physicians may be more comfortable surgically fixing fracture types that fall under their subspecialty. Childs et al 11 found that hand fellowship–trained surgeons treated distal radius fractures with surgical fixation more often than their non–hand surgeon counterparts, reflecting increased experience and level of comfort with complex hand fractures.
Although the number of years postfellowship did not differ between high- and low-volume surgeons, the particular subspecialty of the surgeons did, with all of the high-volume surgeons being orthopaedic trauma surgeons. Therefore, it is plausible that the increased volume of operations in an orthopaedic trauma fellowship and as an attending orthopaedic trauma surgeon allows for the fine-tuning of surgical technique when treating ankle fractures. This is especially true given that there is an initial learning curve that is overcome by repetition of the same procedures. 2
Furthermore, many nonvalidated methods have been reported to evaluate foot and ankle surgery, so it is unclear which outcome measures are most essential for good outcomes following ankle surgery. 35 In orthopaedic surgery, general quality indicators include length of hospital stay, infection, and readmission. 37 Our study analyzed radiographic and functional outcomes to ascertain whether high- or low-volume orthopaedic surgeons, specifically performing ankle fracture open reduction and internal fixation, provided the highest quality of care. We found that higher-volume surgeons—which in this study were both orthopaedic traumatologists—employed superior fixation methodology when compared to lower-volume surgeons, as evidenced by achieving anatomic ankle mortise reduction more frequently and by reducing the number of secondary operations needed.
In a large, multicenter study, Pincus et al 30 found that the reoperation rate for ankle fractures treated with open reduction and internal fixation is approximately 1.5%, whereas the rate of removal of hardware is approximately 18.1%. Our study found a similar overall reoperation rate and removal of hardware rate for the HV cohort: 1.3% and 12.7%, respectively The LV cohort had significantly higher reoperation rates and removal of hardware rates, at 9.0% and 23.9%, respectively. Again, it is plausible that these results are related to the greater volume of operations, and therefore subsequent greater expertise, that the higher-volume surgeons perform.31,32 Additionally, difference between planned vs unplanned removal of hardware procedures could be attributed to surgeon preference.
Patients treated by low-volume surgeons took longer to heal radiographically. It is well known that certain patient characteristics, injury factors, and treatment variables can all contribute to time to union. 26 Although age, sex, BMI, CCI, and fracture pattern were similar among the 2 cohorts, more patients in the low-volume cohort initially presented with an open fracture. It is plausible that these patients had a more severe initial injury, which in turn resulted in longer healing times. The greater number of open fractures in the low-volume cohort likely represents treatment by surgeons while “on call” rather than a specific referral pattern of more complex cases to these surgeons.
We did not find a significantly higher number of wound complications in the low-volume group. However, reoperations overall were significantly more common in the low-volume cohort. Various studies comparing open vs closed ankle fractures have demonstrated that complications more frequently occur after open ankle fractures, and these complications often necessitate secondary procedures, such as incision and drainage, implant removal, and amputation. 28 Out of the 7 secondary incision and drainage procedures that occurred in the low-volume cohort within our study, one was for a patient that originally sustained an open ankle fracture.
The results of our cost analysis demonstrate that high-volume surgeons in this study operated on a more cost-effective basis than do low-volume surgeons. Total costs, variable direct costs, fixed direct costs, and fixed indirect costs were all lower for high-volume surgeons when compared to low-volume surgeons. Given that surgery duration did not differ, the variation in costs is likely reflected by differences in surgical technique. For example, transsyndesmotic suture button use was 0.9% for high-volume surgeons and 18.7% for low-volume surgeons. Virkus et al 38 evaluated the costs of surgically treated rotational ankle fracture by providers who had completed a trauma fellowship and those who had not. They found markedly higher implant-related costs for the non–trauma-trained orthopaedic surgeons. The median surgical cost was also twice as more for non–trauma-trained orthopaedic surgeons. The results of our study are in line with those of Virkus et al, given that all high-volume surgeons within our study were trauma-trained and had lower overall costs.
There are several limitations to our study. Because of the retrospective nature of this study, the integrity of our results depends on the completeness and accuracy of the medical records. This was a single-site study, and may not be able to be generalizable to other sites or health care systems. Additionally, we did not have patient-reported functional outcome scores to compare between groups, so whereas one group may have had more anatomic radiographic results, we do not know how this relates to patient function or well-being. Finally, the smaller sample size of the comparison cohort study may limit the power of some of our statistical analyses. For instance, despite a higher rate of wound complications and infections in the low-volume group, which may be related to more open fractures seen in the low-volume group, the difference did not reach statistical significance, which is likely due to beta error. We also did not have enough data to parse out the specialty outcomes by subgroup and do not know if the findings were applicable more to one group of on-call surgeons than another, based on fellowship training.
In conclusion, our study demonstrated that while wait time to surgery, surgery duration, and length of hospital stay, late mortise widening rates, wound complications, and overall complications were similar between patients undergoing open reduction and internal fixation for a rotational ankle fracture by both high- and low-volume surgeons, the patients treated by low-volume surgeons on average took longer to heal and also had greater reoperation rates than those treated by high-volume surgeons. Additionally, patients treated by high-volume surgeons achieved better postoperative radiographic mortise reductions. Improved mortise reductions and decreased rate of reoperation may be indicative of tailored techniques that experienced, higher-volume surgeons employ because of their greater familiarity with the unique healing issues fracture patients face.
Footnotes
Ethical Approval
This retrospective study was approved by the NYU School of Medicine Institutional Review Board, New York, NY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.